Download presentation
Presentation is loading. Please wait.

1
Great Vessels Anatomy: Innominate Injuries Martha A. Quiodettis

2
Incidence World War I, II, Korea…….no report. Viet Nam.. 3 in 1000 arterial injuries (Rich) Civilian Population: up to 3.2% 71% die prehospital
 Civilian Population: up to 3.2% 71% die prehospital.")
3
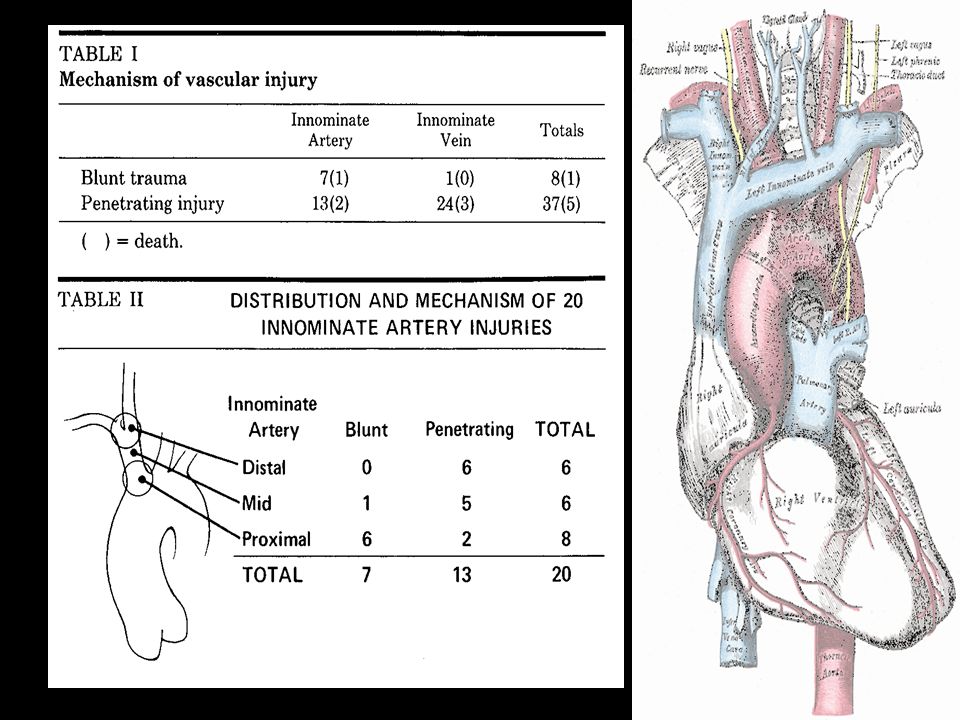
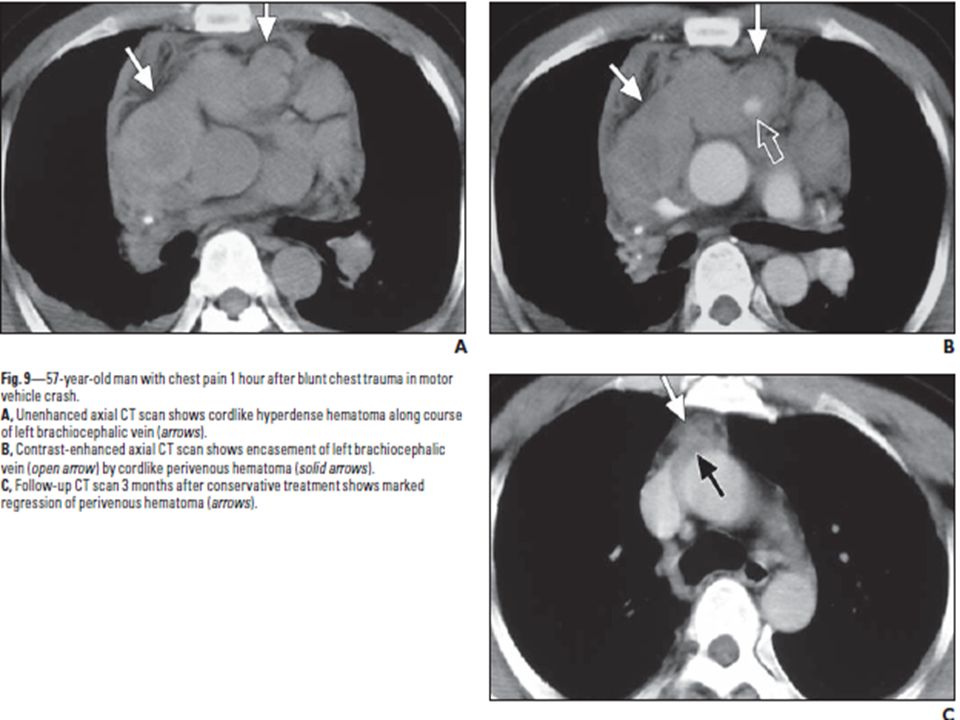
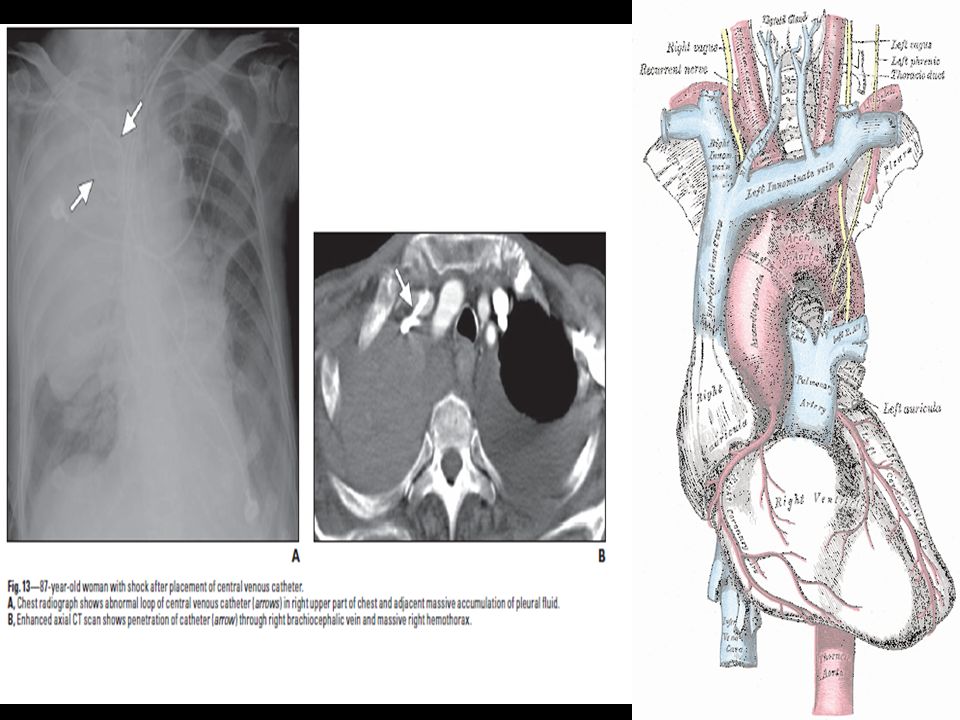
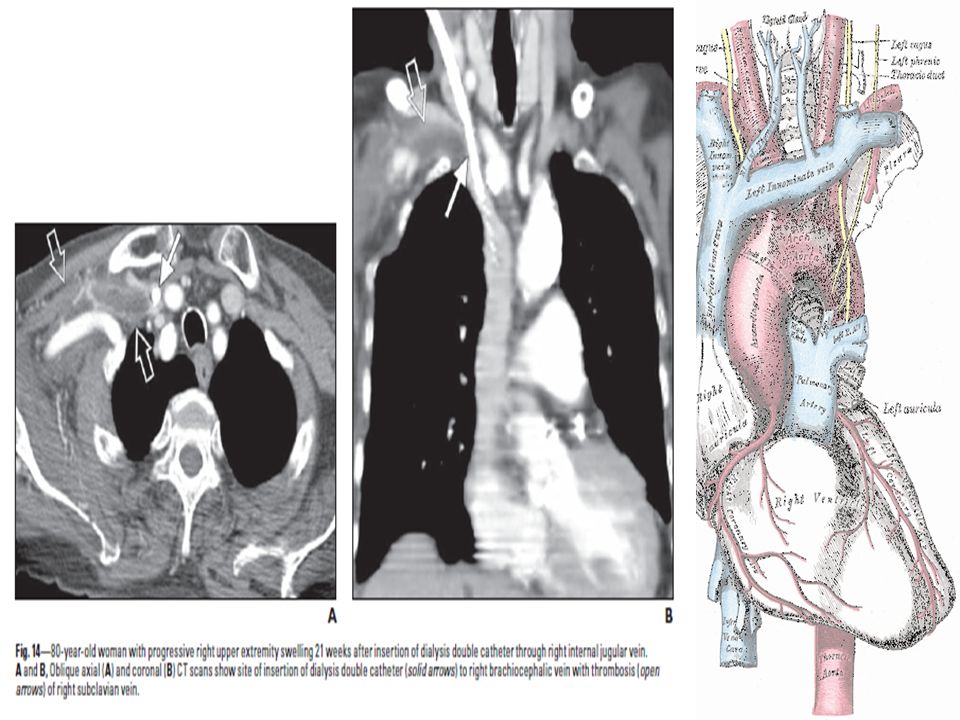
Mechanisms Penetrating traumaPenetrating trauma –> 90% of thoracic great vessel injuries GSWGSW SWSW ShrapnelShrapnel IatrogenicIatrogenic –CVC placement –CT placement –IABP –ER Thoracotomy –Swan-Ganz balloon overinflation –Self-expanding metal stents (esophageal/tracheal) –Low-riding tracheostomy tubes
 –Low-riding tracheostomy tubes")
4
Mechanisms Blunt TraumaBlunt Trauma –Particularly susceptible… Innominate ArteryInnominate Artery Sudden compresion between the sternum and vertebra and hyperextension of the neckSudden compresion between the sternum and vertebra and hyperextension of the neck Pulmonary VeinsPulmonary Veins Vena CavaVena Cava Thoracic AortaThoracic Aorta

5
Blunt TraumaBlunt Trauma –Mechanisms… Shear forcesShear forces –Relative immobility of a portion of the vessel adjacent to a fixed portion CompressionCompression –Between two bony structures »Innominate Artery – May be pinced between sternum and vertebrae Profound intraluminal HTNProfound intraluminal HTN

7
Clavicle fracture and flail chest

8
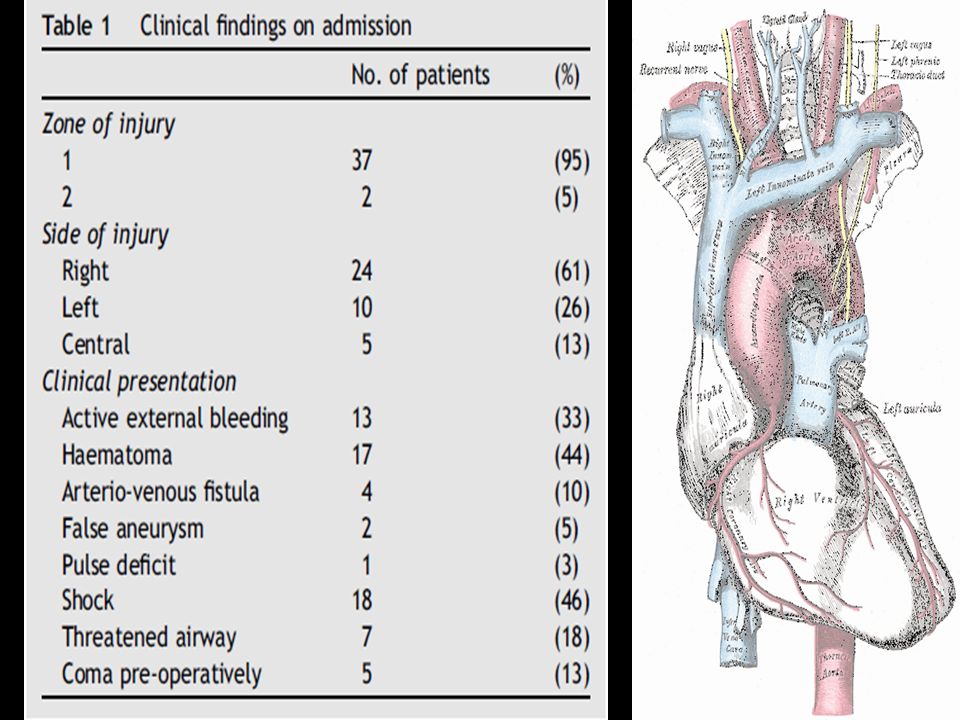
PhysicalPhysical –ATLS Protocol –Clinical findings… Pericardial tamponade +/-Pericardial tamponade +/- HypotensionHypotension Upper extremity HTNUpper extremity HTN Unequal BP or pulses in the extremitiesUnequal BP or pulses in the extremities External evidence of major chest traumaExternal evidence of major chest trauma Expanding hematoma at the thoracic outletExpanding hematoma at the thoracic outlet Intrascapular murmurIntrascapular murmur Palpable fracture of the sternumPalpable fracture of the sternum Palpable fracture of the thoracic spinePalpable fracture of the thoracic spine Left flail chestLeft flail chest –50% of pts with aortic/great vessel injury present without physical signs of injury –FAST U/S Pericardial bloodPericardial blood +/- tamponade+/- tamponade

10
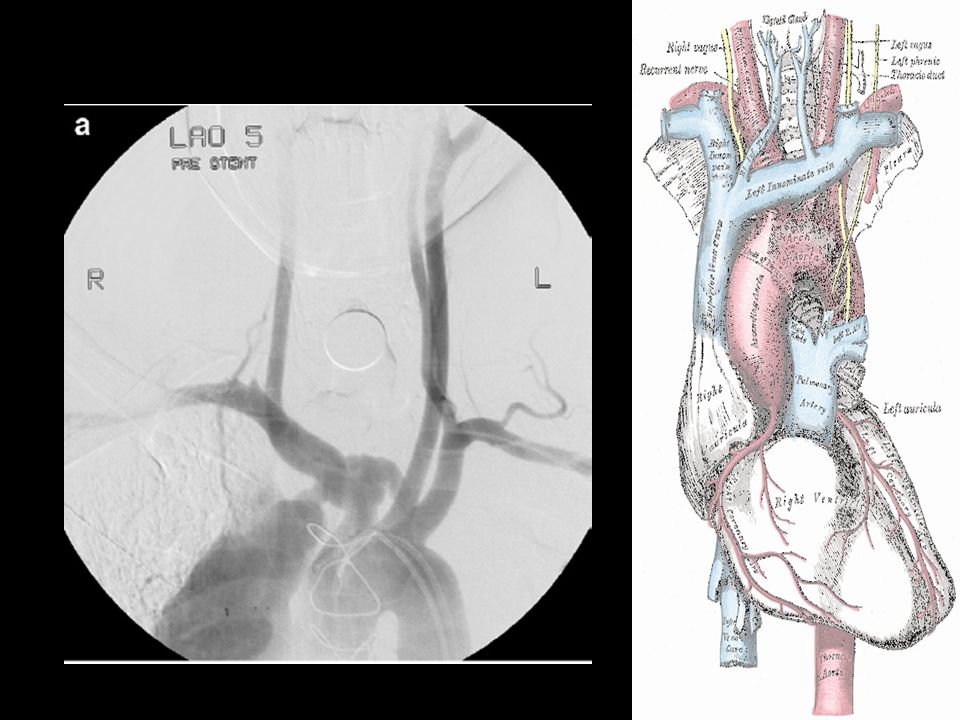
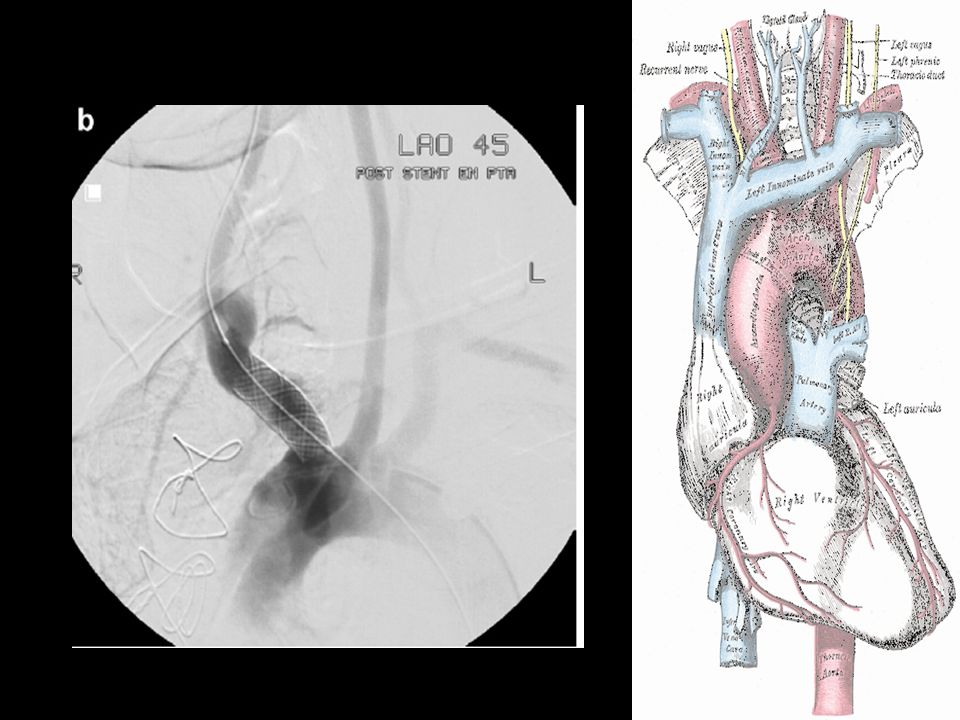
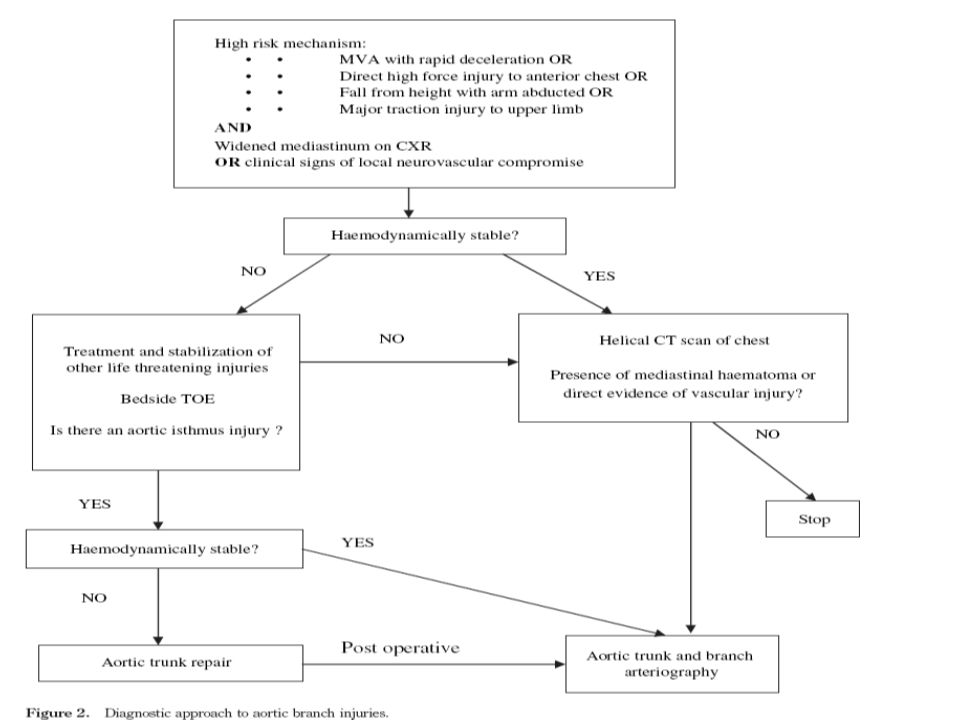
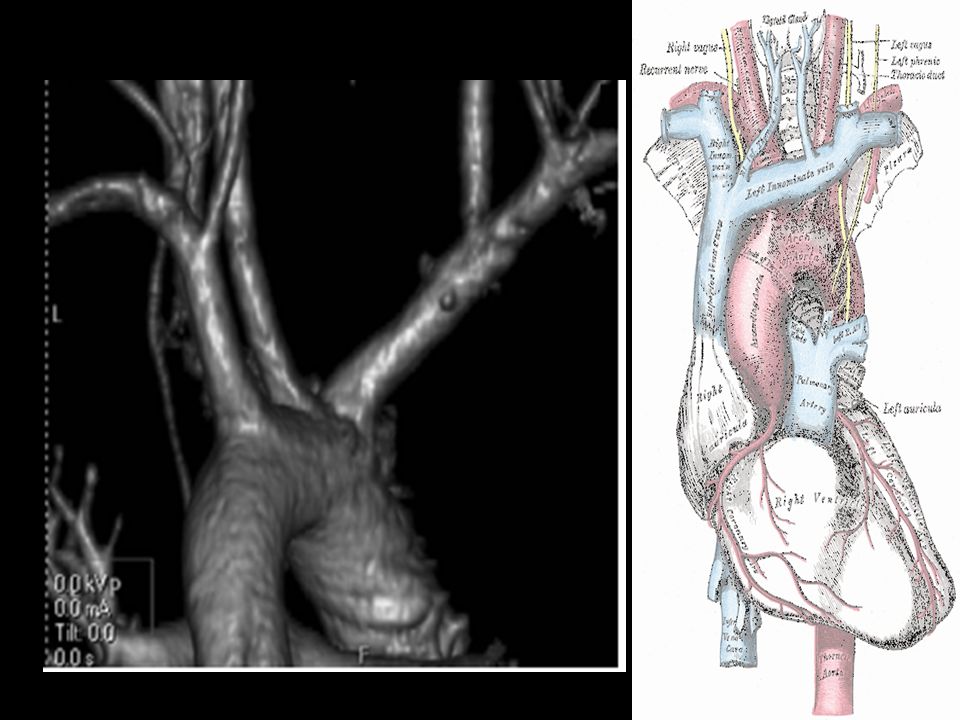
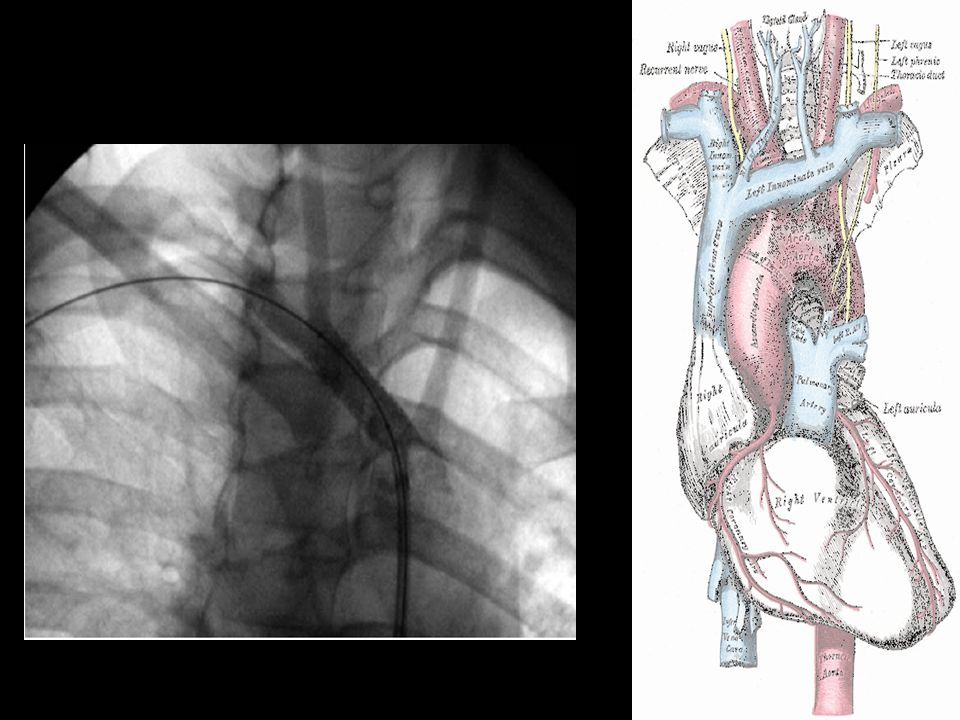
Diagnostic options Chest X Ray FAST Helical CT Angiography Transesophageal ecocardiogram

13
ED Thoracotomy

15
“Clam Shell” Exposure

16
Clam Shell Exposure

17
Median Sternotomy Incision

19
Extending Sternotomy into Neck

24
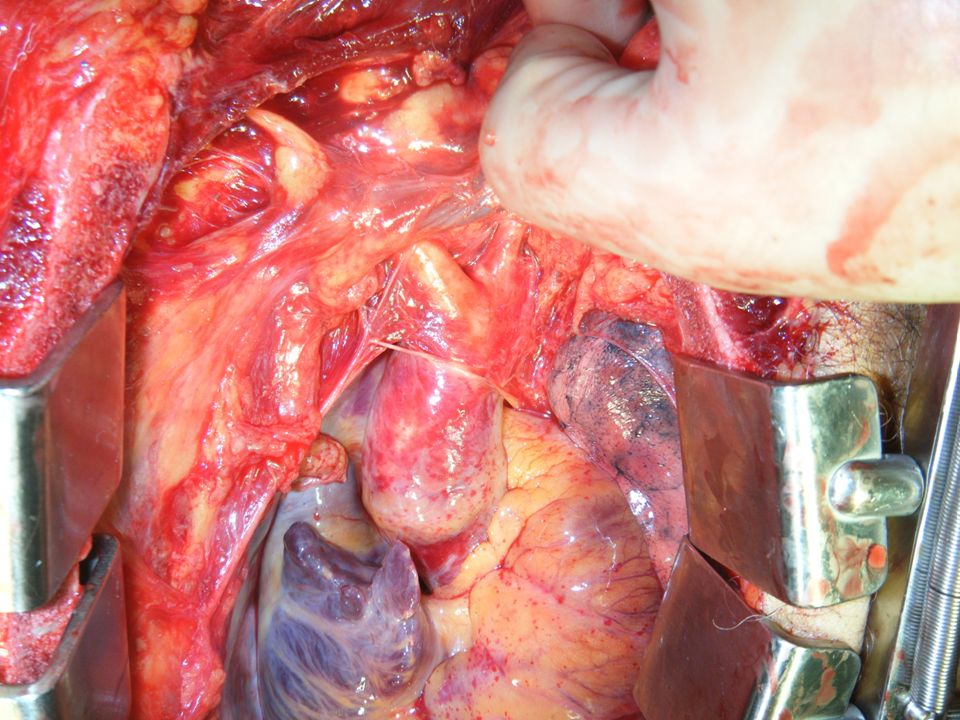
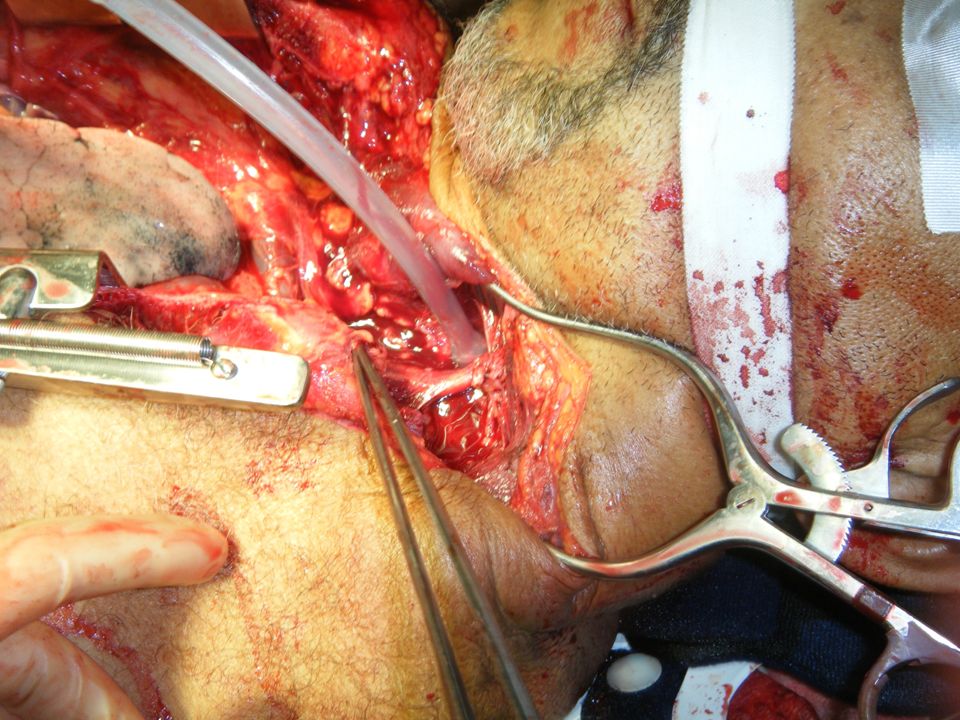
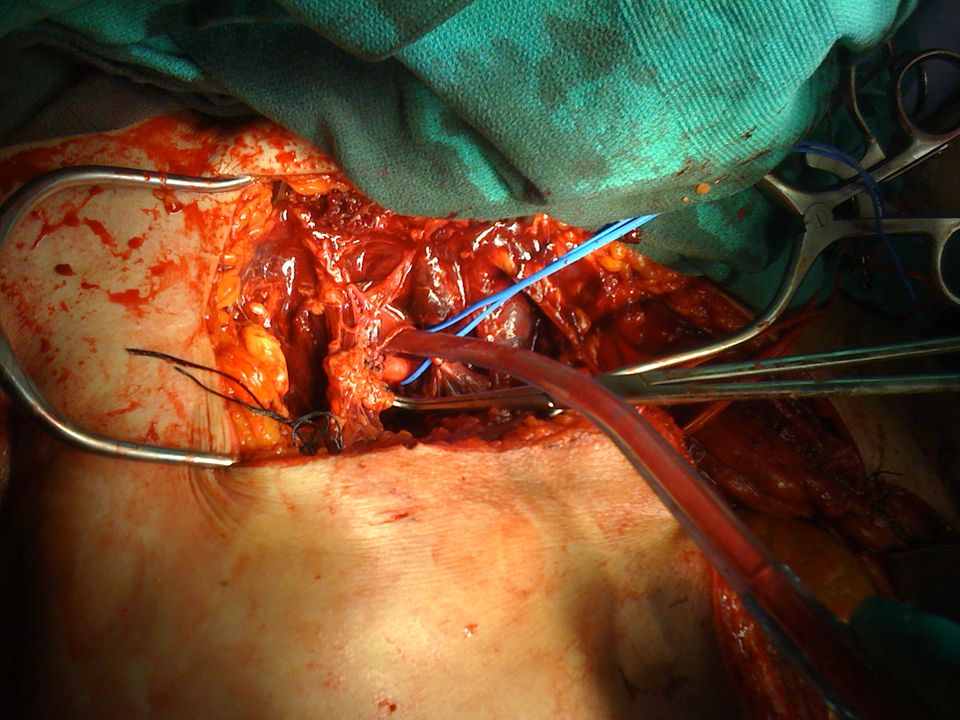
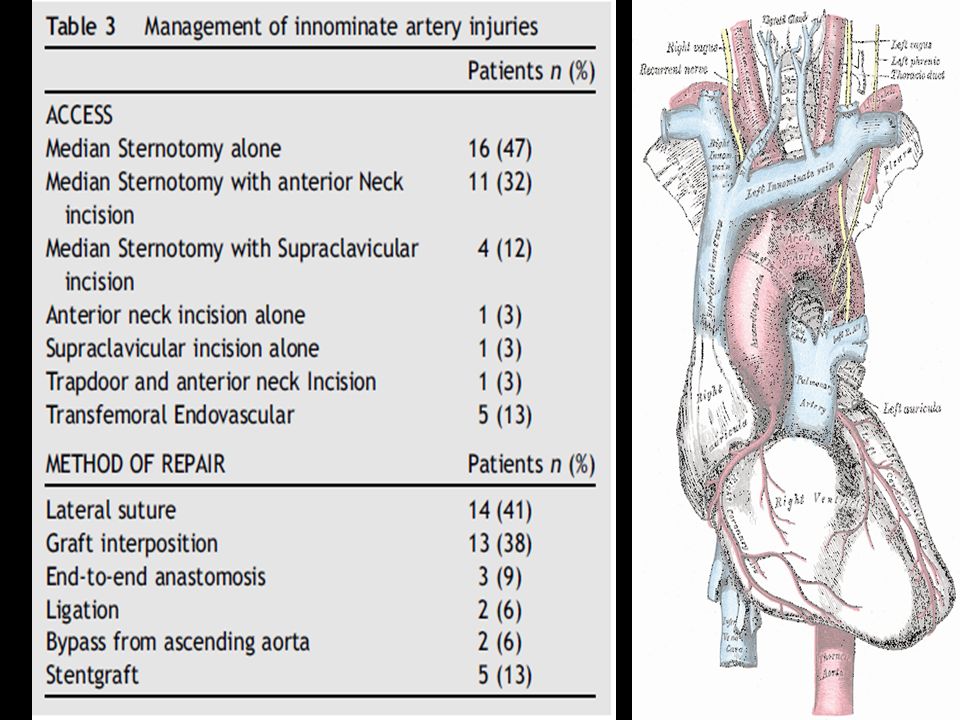
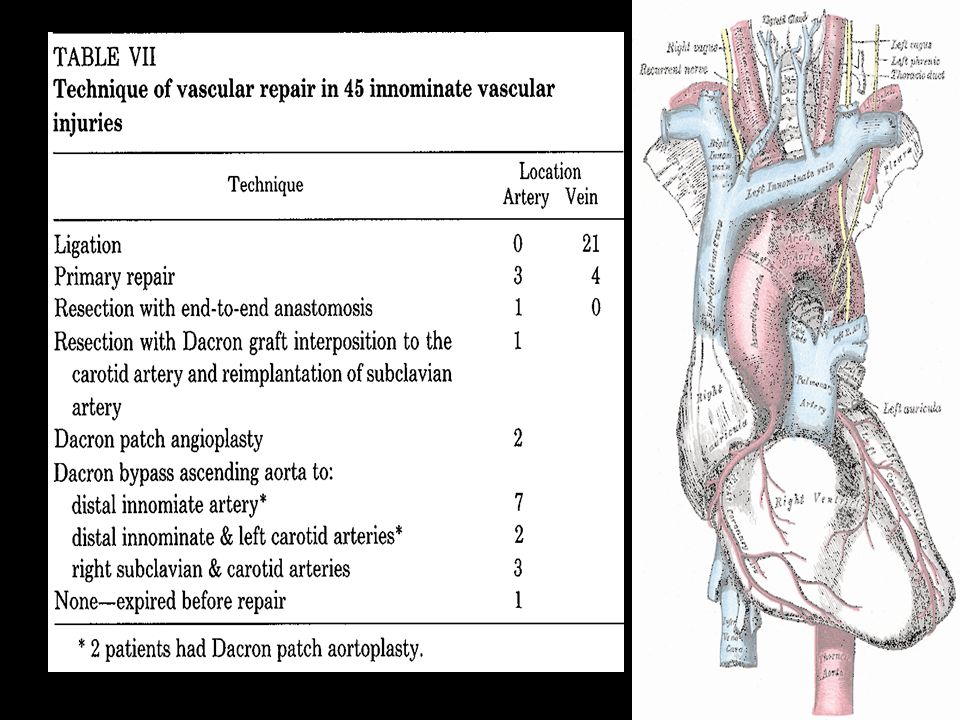
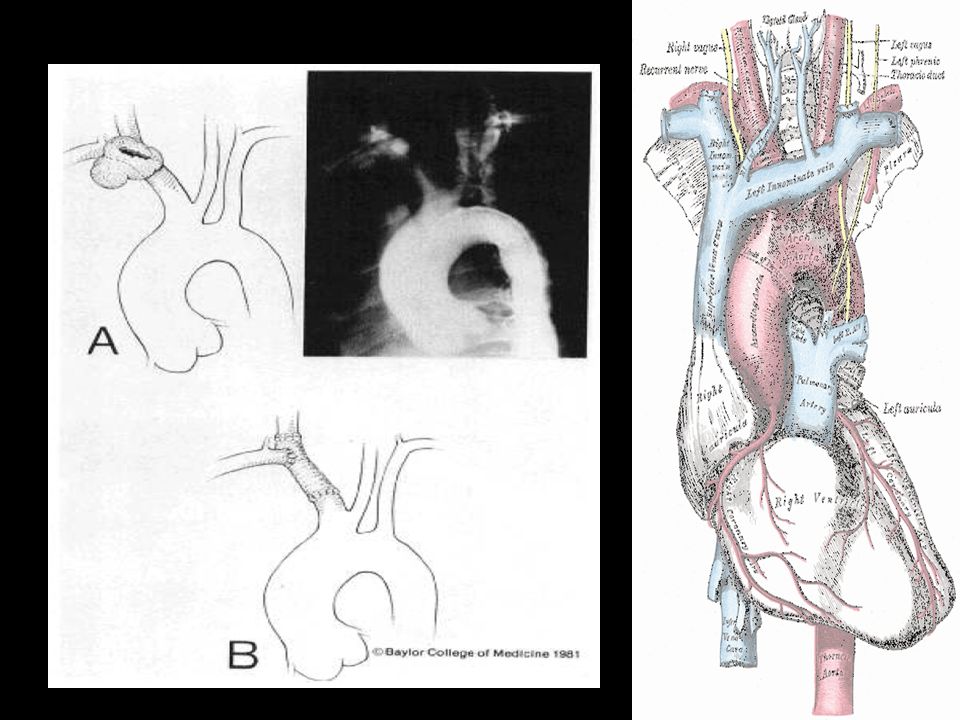
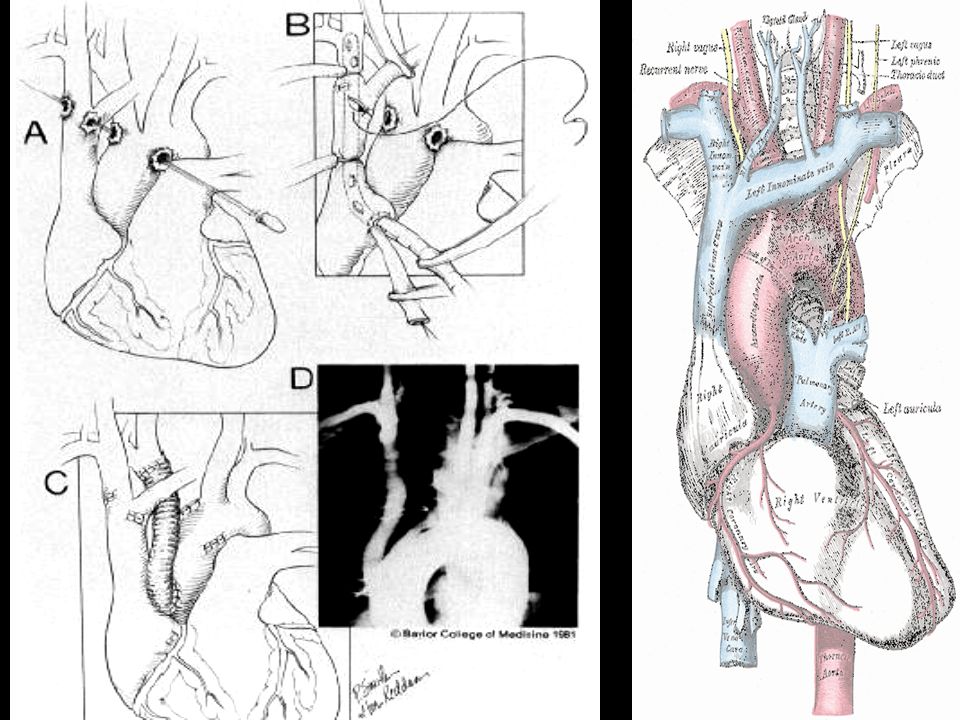
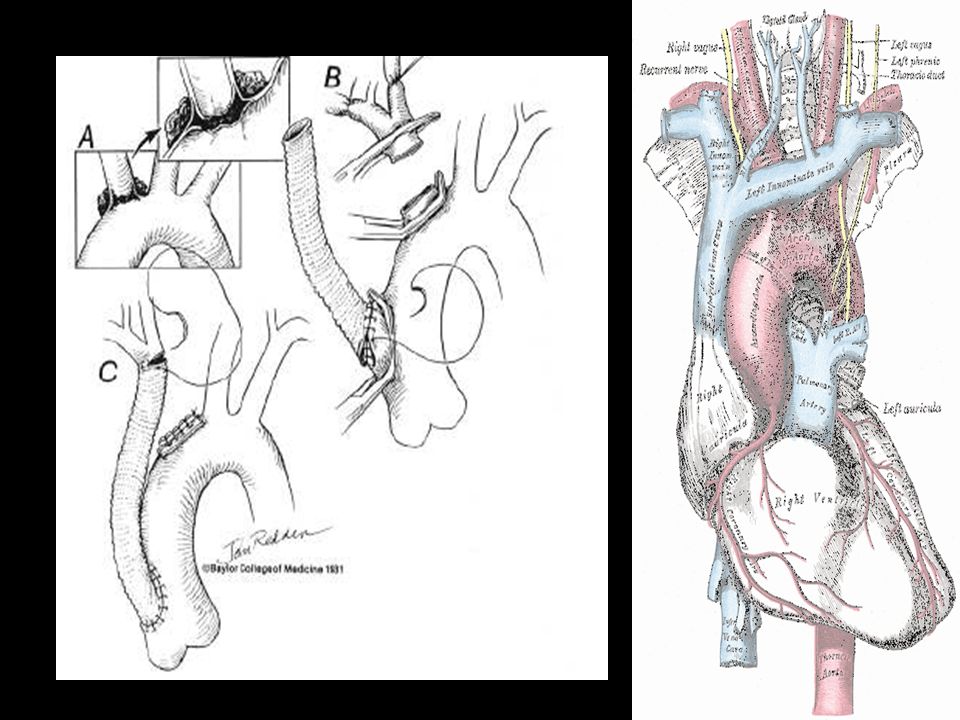
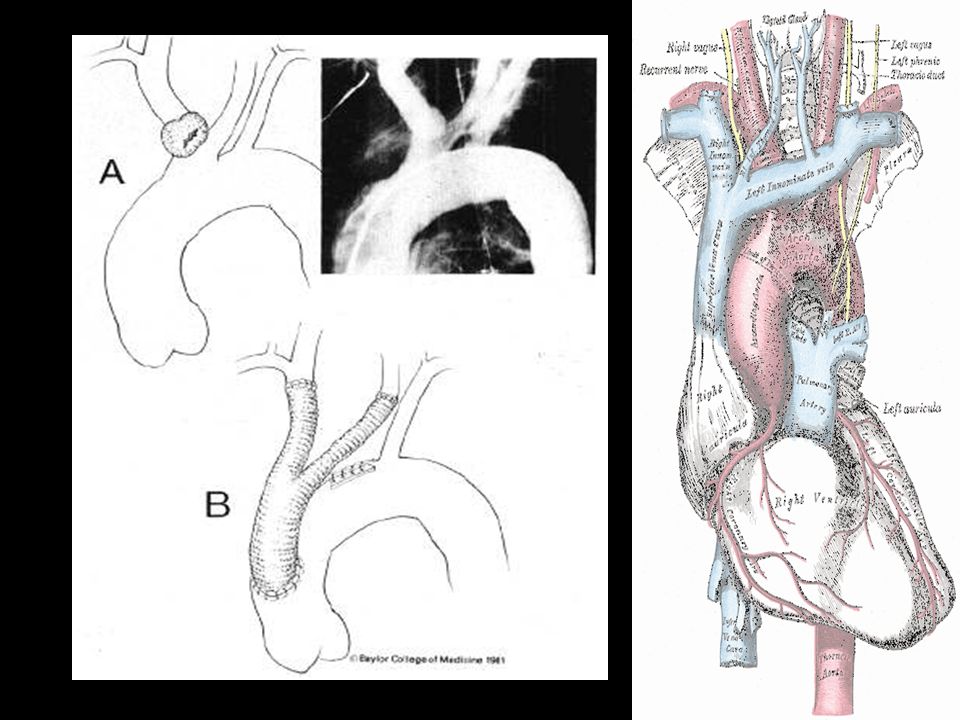
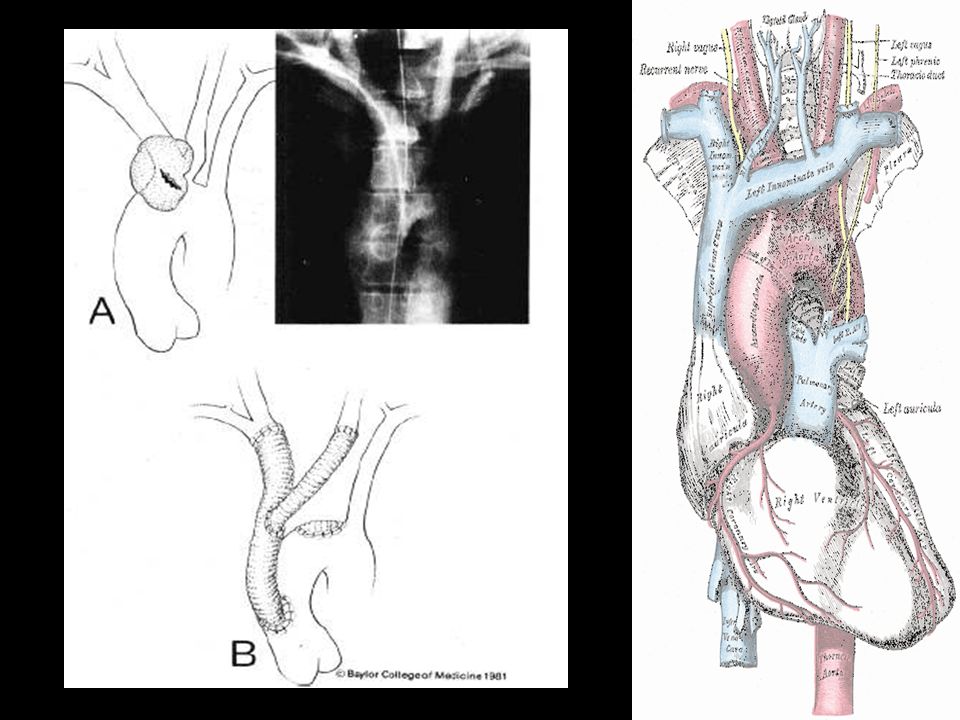
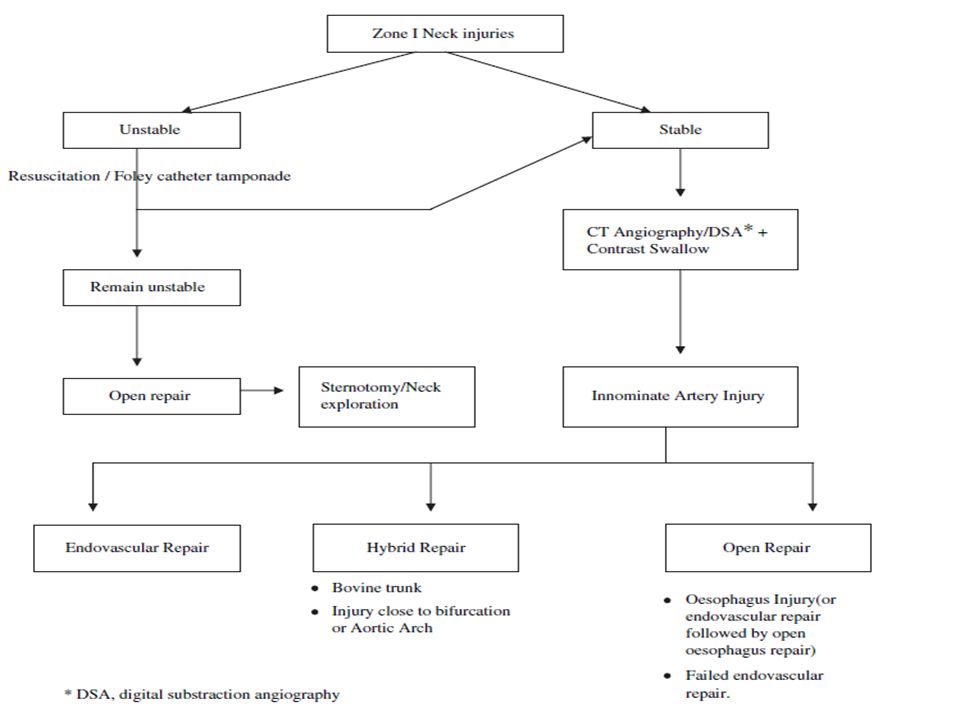
Innominate Artery Partial Tears –Running lateral arteriorrhaphy 5- 0 Prolene suture Complex Tears –Bypass Exclusion Technique Ascending Aorta to the distal innominate artery Dacron graft Avoid the area of injury until the areas for bypass insertion are exposed No need for hypothermia, systemic heparinization or shunts… Place a pericardial flap between the graft and the vein ( if vein left intact)
")
25
Tips from the Masters Proximal and distal control before entering the hematoma Keep MAP at least 60 Fragile structure. 5-0 or less. 8-12mm Dacron graft Routine use of shunts or CP bypass are not mandatory Be aware of anatomic variants (Up to 30%)
.")
44
Systemic Air Embolism Caused by a penetrating wound that injures a pulmonary vein and bronchiole and forms a fistula Allows air bubbles to enter the L heart and embolize to the systemic circulation –Coronary Arteries – MI, cardiac arrest –Cerebral Arteries – Seizures, CVA, death Treatment –Thoracotomy –Clamping of the pulmonary hilum to prevent further embolization –Aspiration of the air from the left ventricle Trendelenburg position with right side down

45
Foreign Body Embolism Thoracic great vessels may serve as both an entry site or final resting place for intravascular bullet emboli –May produce infection, ischemia, or injury to organs distant from the site of trauma –25% lodge in the pulmonary arteries Should be removed to prevent pulmonary thrombosis, sepsis or other complications May be done via fluoroscopic guidance or open technique

47
Remember……… Transection of the innominate artery at is origin is extremely rare, but is the second most common aortic injury from which a patient survives enough to have diagnosis and surgical repair.

48
QUESTIONS?????

Similar presentations






 Division of Thoracic Surgery May 28, 2009.>")

















