Download presentation
Presentation is loading. Please wait.

1
Never a dull moment…….. Leland Carr, O.D. Oklahoma College of Optometry CarrLW@nsuok.edu

2
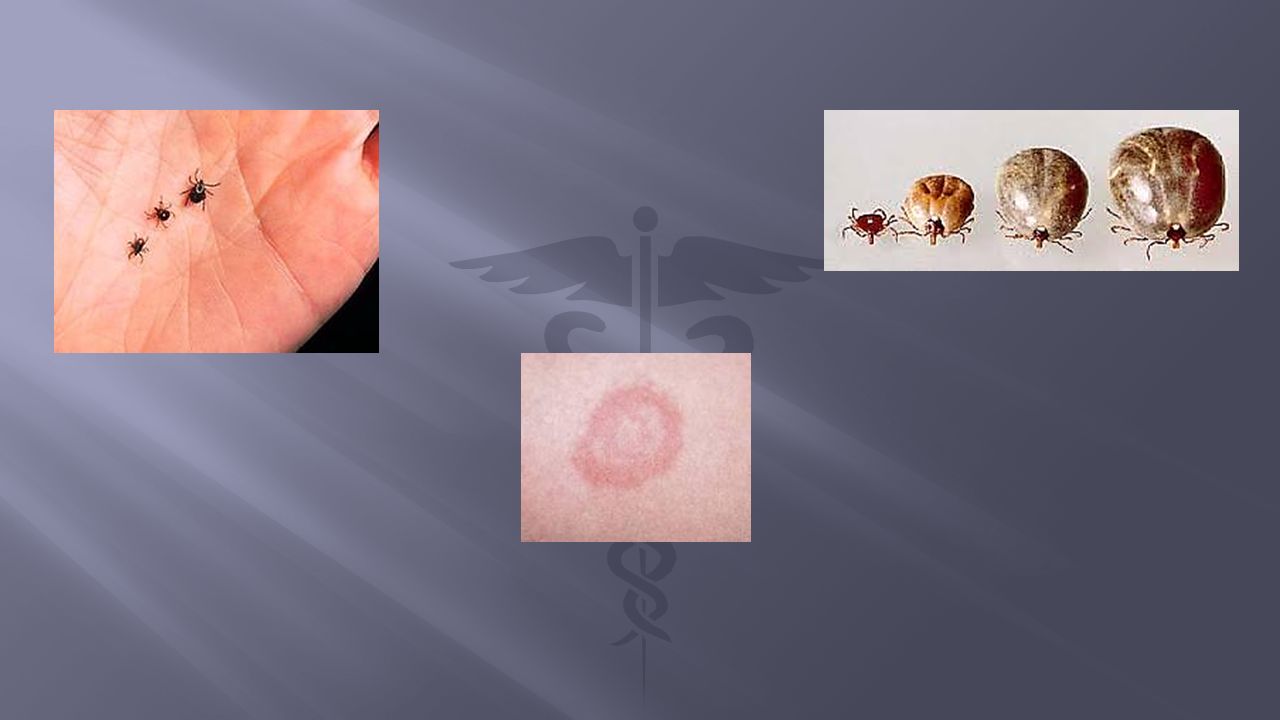
E.R. visit #1: “Horrible headache x 2 days. Worsening.” “Something’s not right with my vision.” Seen in another E.R. two days prior Dx: MIGRAINE HEADACHE (+) for Tick Bite “about two weeks ago”
 for Tick Bite about two weeks ago .")
4
Poorly-controlled Type 1 Diabetic History of Major Depressive Disorder History of Obstructive Sleep Apnea Meds: Insulin Gabapentin Fenofibrate Omeprazole

5
Temperature: 99.8 Blood pressure: 132/88 Random/Manifest Glucose: 247 Complete Blood Count: Elevated W.B.C. slightly reduced platelet count C-reactive Protein: 8.3 Rapid Plasma Reagin: (-) Tick Panel ordered H.I.V. ordered OPTOMETRY RESIDENT CALLED IN C.T. Scan (without contrast) of Head, Ordered
 Tick Panel ordered H.I.V. ordered OPTOMETRY RESIDENT CALLED IN C.T. Scan (without contrast) of Head, Ordered.")
6
C.T. results: “No acute intracranial pathology noted.” Optometry Resident assessment: “Papilledema. Bilateral swollen disks.” PATIENT ADMITTED TO HOSPITAL Following Day: Tick Panel (+) for Rocky Mountain Spotted Fever, (-) for Lyme Disease and Tularemia Lumbar Puncture performed Opening pressure of 24 Clear C.S.F. sample M.R.I. Order Placed
 for Rocky Mountain Spotted Fever, (-) for Lyme Disease and Tularemia Lumbar Puncture performed Opening pressure of 24 Clear C.S.F. sample M.R.I. Order Placed.")
7
Intramuscular Rocephin 100mg. Doxycycline b.i.d. x 14 days Phenergan tabs as needed for nausea

8
RETURNS TO E.R. ONE DAY LATER C/O: “Front of my head feels like it’s going to explode.” C/O: “My headaches worse and I’m sick to my stomach.” Given morphine i.v. x 3 CONSULT REQUESTED OF OPTOMETRY BY E.R. PHYSICIAN: “Please re check eye pressure, visual disturbance, and headache.” Patient to be seen 24 hours later in eye clinic.

9
VA’s: 20/50 20/40 Motilities: Full. Pain increase on rotations. (+) for intermittent “bright flickers of light” Clear anterior chamber I.O.P. 14mmHg 15mmHg DISSOCIATED PUPIL RESPONSE NO relative afferent pupillary defect Weak responses to Direct & Consensual Strong response to Near pupil testing
 for intermittent bright flickers of light Clear anterior chamber I.O.P. 14mmHg 15mmHg DISSOCIATED PUPIL RESPONSE NO relative afferent pupillary defect Weak responses to Direct & Consensual Strong response to Near pupil testing.")
11
Consult Report back to Hospitalist: M.R.I. of Brain M.R.I. of Orbits Advise re-check in Optometry in 1 week Visual Fields O.C.T. of nerve and nerve fiber layer (RNFL) Consider oral prednisone, starting at 60mg. Daily What about the Optic Neuritis clinical trials ???? What about the Diabetes ????
 Consider oral prednisone, starting at 60mg. Daily What about the Optic Neuritis clinical trials . What about the Diabetes .")
13
Headpain “Back of my head and neck. But kind of all over…” “Pounding pain. Annoying.” “Vision getting worse over about 6 weeks.” CONSULT REQUESTED BY URGENT CARE CLINIC History of intramuscular steroid injections Dexamethasone and Triamcinolone For painful lower back sprain Given weekly for 3 weeks

14
Type 2 Diabetic, “Pretty good control. Yes, my doctor’s happy.” Systemic Hypertension, “Pretty well controlled. Happy doctor.” No prior records at facility. OUR EXAM: VA’s: 20/200 20/400 Pinhole: No improvement OD or OS DISSOCIATED PUPIL RESPONSE Sluggish to Light, OU. 1(+) A.P.D., OS Motilities: Full, Pain-free, Convergence intact External Exam: Mild “watery eye” without hyperemia Anterior: Corneas clear. Anterior Chambers clear. I.O.P.: 23mmHg. 25mmHg. Dilated with Tropicamide and Phenylephrine
 A.P.D., OS Motilities: Full, Pain-free, Convergence intact External Exam: Mild watery eye without hyperemia Anterior: Corneas clear. Anterior Chambers clear. I.O.P.: 23mmHg. 25mmHg. Dilated with Tropicamide and Phenylephrine.")
Similar presentations





>")















