Download presentation
Presentation is loading. Please wait.

1
BYBY

2
DEFINITION CIH was defined as blood glucose level > 140 mg/dl on two separate tests 1 hour apart or >180 mg/dl at any time (Preissig & Rigby, 2009). The ability to control BG is known to be impaired in patients subjected to the stress of critical illness resulting in high BG levels (stress induced hyperglycemia or CIH (Yung et al., 2008). CIH is often considered an extreme form of 'stress' hyperglycaemia (infection (sepsis), dextrose-containing crystalloid, dextrose absorption during peritoneal dialysis, lack of muscular activity, overfeeding, hypokalemia, and drugs) (Halverson-Steele, 2005).
. CIH is often considered an extreme form of stress hyperglycaemia (infection (sepsis), dextrose-containing crystalloid, dextrose absorption during peritoneal dialysis, lack of muscular activity, overfeeding, hypokalemia, and drugs) (Halverson-Steele, 2005)..")
3
It is one of the most prevalent problems in PICUs (Hirshberg et al., 2008). About 2/3 of children in PICU requiring MV developed CIH, while more than 90% of patients with both respiratory and CVS failure developed CIH (Preissig et al., 2009). The occurrence of hyperglycemia has been shown to be associated with poor outcomes including death, sepsis, and increased LOS (Srinivasan et al., 2004). Most clinicians are convinced that BG really matters, that glycemic management and strategy should be performed in critically ill patients, and that excessive hyperglycemia should be avoided. While efforts are undertaken to implement TGC, but still only a minority of the centers have a standard approach for screening and treating hyperglycemia and the majority of the centers (80%) lack even the standard approach to screen for and treat elevated BG levels (Preissig &Rigby, 2010).
. The occurrence of hyperglycemia has been shown to be associated with poor outcomes including death, sepsis, and increased LOS (Srinivasan et al., 2004). Most clinicians are convinced that BG really matters, that glycemic management and strategy should be performed in critically ill patients, and that excessive hyperglycemia should be avoided. While efforts are undertaken to implement TGC, but still only a minority of the centers have a standard approach for screening and treating hyperglycemia and the majority of the centers (80%) lack even the standard approach to screen for and treat elevated BG levels (Preissig &Rigby, 2010)..")
4
Challenges that prevent achieving TGC in practice including (Kovalaske & Gandhi, 2009).; Increased risk of hypoglycemia, Increased utilization of resources, Significant revamping of infrastructure to implement glycemic management protocols, Additional personnel training, Need for intense coordination among varied involved specialties, Data on TGC with the use of insulin in critically ill children have been lacking.
.; Increased risk of hypoglycemia, Increased utilization of resources, Significant revamping of infrastructure to implement glycemic management protocols, Additional personnel training, Need for intense coordination among varied involved specialties, Data on TGC with the use of insulin in critically ill children have been lacking.")
6
AIMS AND OBJECTIVES The aim of this randomized controlled study was to compare the effects of standard (SGC) versus tight glycemic control (TGC) on mortality. Secondary endpoints involved the LOS, need for mechanical ventilation (MV), cardiovascular support (CVS), morbidity, and number of hypoglycemic attacks.
, cardiovascular support (CVS), morbidity, and number of hypoglycemic attacks..")
8
Trial profile (Assessment and randomization of the studied patients)
")
10
Ethical Consent RandomizationData collection Physical examination Routine Lab investigations Interventions *

11
Informed consent was obtained from the parents or legal guardians of the eligible subjects. Patients were randomized. Each child was subjected to data collection including: age, sex, diagnosis, and indication for PICU admission, clinico-laboratory assessment including general examination with emphasis on anthropometric measurements, and vital signs. Detailed systemic examination was done to verify the inclusion and exclusion criteria and level of respiratory and CVS support. Routine laboratory assessment including CBC, kidney function tests, liver function tests, CRP and cultures (blood and endotracheal) was performed. Pediatric Logistic Organ Dysfunction (PELOD) scores were calculated for every included patient in his/her first 24 hours of PICU admission. The patients’ hospital courses were followed to determine the outcome (survival to discharge).
 was performed. Pediatric Logistic Organ Dysfunction (PELOD) scores were calculated for every included patient in his/her first 24 hours of PICU admission. The patients’ hospital courses were followed to determine the outcome (survival to discharge)..")
12
INTERVENTION Patients were randomly assigned to SGC (n=14) and TGC (n=16) by sealed envelopes. Both groups were compared regarding: LOS The need of respiratory and/or cardiovascular support. Development of any associated infections. Survival to discharge. The number of hypoglycemic attacks. The time needed to normalization of blood glucose.

13
Tight glycemic control This group proceeded through glucose control methods, in stepwise approach, aiming to achieve a target blood glucose level of 80-140 mg/dl. Removal of correctable causes of stress hyperglycemia such as analgesia for pain and and reduction of the sources of glucose input to the limit of maintaining a minimum caloric intake from glucose to 50% of daily caloric needs determined by Schoefield and White formulas (Sentongo et al., 2000).
..")
14
Starting insulin infusion when the blood glucose concentration exceeded the upper limit (140 mg/dl) in spite of the previous two steps. The dose was titrated to maintain the BG values within the defined target (80-140 mg/dl). Insulin infusion was prepared as 50 IU Actrapid in 50 ml NaCl 0.9%. The insulin dose was adjusted by measuring BG concentration using commercially available analyzer which was rigorously maintained.
. Insulin infusion was prepared as 50 IU Actrapid in 50 ml NaCl 0.9%. The insulin dose was adjusted by measuring BG concentration using commercially available analyzer which was rigorously maintained..")
15
Repetition of BG level measurement at the following intervals: 30 minutes when treating hypoglycemia, 1 hour throughout insulin infusion and after changing fluids or other interventions. 2 hours when the values are within the target (140-180). 6 hours for 24 hours when the values are within the target for 24 hours. 12 hours for the next 24 hours when the values are within the target for 48 hours. Every 24 hours when the values are within the target for 72 hours until discharge from the PICU.
. 6 hours for 24 hours when the values are within the target for 24 hours. 12 hours for the next 24 hours when the values are within the target for 48 hours. Every 24 hours when the values are within the target for 72 hours until discharge from the PICU..")
16
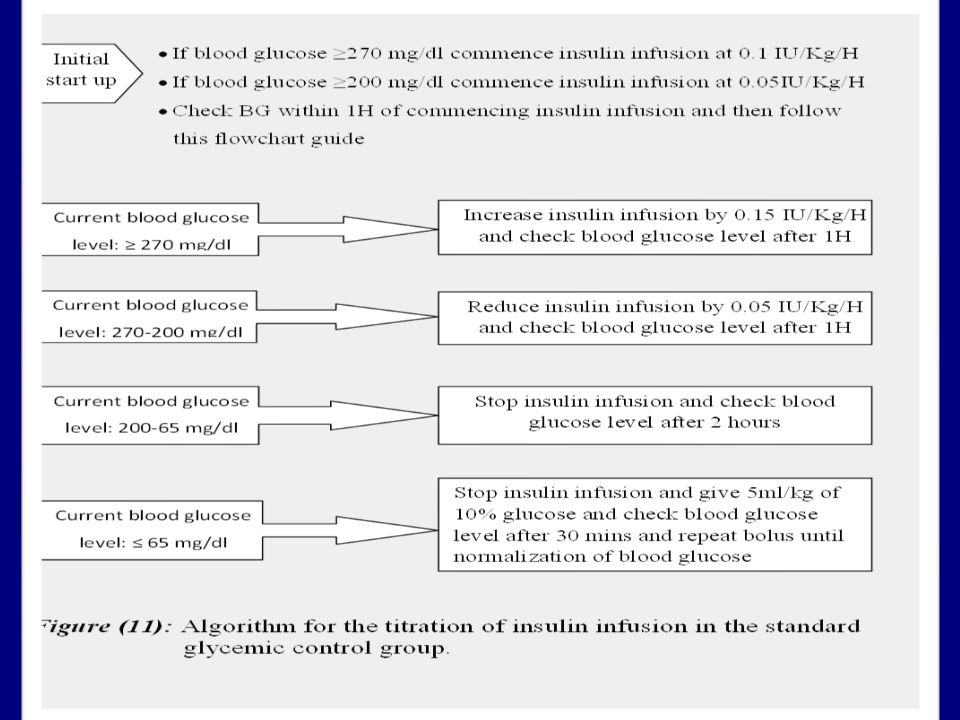
Standard glycemic control Children in this group were treated when the BG levels exceeded 200 mg/dl using the same stepwise approach aiming to achieve BG levels less than 200 mg/dl.

20
Item SGC N = 14 TGC N = 16 P-value Age (months) 21.14 ± 31.14 (4 - 111) 34.06 ± 44.01 (4 - 153) 0.37 ●Gender (no, %) Male/Female 7/7 (50/50%) 10/6 (62.5/37.5%) 0.37 Weight (kg) 8.54 ± 5.32 (4 - 20) 10.97 ± 8.87 (4 - 40) 0.3 Length (cm) 76.36 ± 23.23 (57 - 138) 83.25 ± 23.87 (54 - 147) 0.41 LOS (hours) 257.14 ± 147.98 (86 - 611) 231.06 ± 166.69 (35 -659) 0.67 ●Comorbidity Positive (no, %) 4 (28.6%) 7 (43.9%) 0.32 Pediatric Logestic Organ Dysfunction Score 15.89 ± 19.89 (0 - 79.6) 10.19 ± 5.75 (0 – 21) 0.42 ● Mechanical ventilation Positive (no, %) 7 (50%) 13 (81.3%) 0.08 ● Cardiovascular support Positive (no, %) 10 (71.4%) 12 (75%) 0.57 ● Complete Blood Count Shift (no, %) 3 (21.4%) 2 (12.5%) 0.43 ● C-reactive protein Positive (no, %) 8 (57.1%) 7 (43.8%) 0.36 ●Culture: Growth (no, %) 6 (42.9%)3 (13%)0.15 Table (1): Comparison between the “ Standard ” and “ Tight ” glycemic control groups for the baseline parameters
 ± ( ) ± ( ) 0.37 ●Gender (no, %) Male/Female 7/7 (50/50%) 10/6 (62.5/37.5%) 0.37 Weight (kg) 8.54 ± 5.32 (4 - 20) ± 8.87 (4 - 40) 0.3 Length (cm) ± ( ) ± ( ) 0.41 LOS (hours) ± ( ) ± ( ) 0.67 ●Comorbidity Positive (no, %) 4 (28.6%) 7 (43.9%) 0.32 Pediatric Logestic Organ Dysfunction Score ± ( ) ± 5.75 (0 – 21) 0.42 ● Mechanical ventilation Positive (no, %) 7 (50%) 13 (81.3%) 0.08 ● Cardiovascular support Positive (no, %) 10 (71.4%) 12 (75%) 0.57 ● Complete Blood Count Shift (no, %) 3 (21.4%) 2 (12.5%) 0.43 ● C-reactive protein Positive (no, %) 8 (57.1%) 7 (43.8%) 0.36 ●Culture: Growth (no, %) 6 (42.9%)3 (13%)0.15 Table (1): Comparison between the Standard and Tight glycemic control groups for the baseline parameters")
21
Item SGC N = 14 TGC N = 16 P-value Max BG (mg/dl) 478.64 ± 105.65485.44 ± 185.32 0.98 Hours for CIH to develop 147.93 ± 127.02 166.81 ± 145.62 0.69 Frequency of BG measurement per hour 0.48 ± 0.180.71 ± 0.19 0.006* Total BG measurement (measurements/LOS) 43.93 ± 19.7540 ± 15.92 0.51 Minimal BG (mg/dl) 66.21 ± 22.5943.5 ± 23.6 0.025* Mean BG (mg/dl) 103.23 ± 46.87130.73 ± 52.68 0.281 Starting insulin infusion rate (U/kg/h) 0.77 ± 0.580.72 ± 0.37 0.72 Maintenance insulin infusion rate (U/kg/h) 0.52 ± 0.370.46 ± 0.42 0.87 Peak insulin requirement (U/kg/h) 0.85 ± 0.531.06 ± 0.9 0.35 Total insulin requirement in 1 st day (U/kg) 0.55 ± 0.430.48 ± 0.3 0.61 Total insulin requirement per LOS (U/kg) 8.1 ± 9.2610.13 ± 12.98 0.56 Duration of insulin requirement (U/h) 12.64 ± 9.6918.94 ± 11.040.16 Table (2): Comparison between the “ Standard ” and “ Tight ” glycemic control groups for the BG and insulin parameters
 ± ± Hours for CIH to develop ± ± Frequency of BG measurement per hour 0.48 ± ± * Total BG measurement (measurements/LOS) ± ± Minimal BG (mg/dl) ± ± * Mean BG (mg/dl) ± ± Starting insulin infusion rate (U/kg/h) 0.77 ± ± Maintenance insulin infusion rate (U/kg/h) 0.52 ± ± Peak insulin requirement (U/kg/h) 0.85 ± ± Total insulin requirement in 1 st day (U/kg) 0.55 ± ± Total insulin requirement per LOS (U/kg) 8.1 ± ± Duration of insulin requirement (U/h) ± ± Table (2): Comparison between the Standard and Tight glycemic control groups for the BG and insulin parameters")
22
Outcome SGC N = 14 TGC N = 16 P-value Non-survivors7 (50%)11 (68.8%)0.25 Hypoglycemic event (no, %)7 (50%)12 (75%)0.15 Renal Function Test Elevation (no, %)5 (35.7%)3 (18.8%)0.26 Liver Function Test Elevation (no, %)5 (35.7%)2 (12.5%)0.14 Table (3): Comparison between the “ Standard ” and “ Tight ” glycemic control groups for the outcome parameters
11 (68.8%)0.25 Hypoglycemic event (no, %)7 (50%)12 (75%)0.15 Renal Function Test Elevation (no, %)5 (35.7%)3 (18.8%)0.26 Liver Function Test Elevation (no, %)5 (35.7%)2 (12.5%)0.14 Table (3): Comparison between the Standard and Tight glycemic control groups for the outcome parameters")
23
Hypoglycemic events (Blood glucose ≤ 65mg/dl) SGC (n=14)TGC (n=16)P-value None7 (50%)4 (25%)0.15 13 (21.43%)4 (25%)0.58 2-32 (14.29%)5 (31.25%)0.26 3<2 (14.29%)3 (18.75%)0.57 Time to Blood glucose level Normalization (hours) Mean ± SD (Range) 0.29 ± 0.32 (0-1) 0.91 ± 1.1 (0-4.5) Table (4): Frequency distribution of the studied patients according to the number of hypoglycemic events
 SGC (n=14)TGC (n=16)P-value None7 (50%)4 (25%) (21.43%)4 (25%) (14.29%)5 (31.25%)0.26 3<2 (14.29%)3 (18.75%)0.57 Time to Blood glucose level Normalization (hours) Mean ± SD (Range) 0.29 ± 0.32 (0-1) 0.91 ± 1.1 (0-4.5) Table (4): Frequency distribution of the studied patients according to the number of hypoglycemic events")
24
Table (5):Comparison between the survivors and non-survivors in the studied patients Item Survivors N = 12 Non-survivors N = 18 p-value Length of stay (hours) 206.42 ± 124.38 (86 - 533) 267.78 ± 173.07 (35 - 659) 0.24 Max blood glucose 440.5 ± 136.77510.11 ± 157.17 0.18 Pediatric Logestic Organ Dysfunction Score 9.08 ± 6.212.5 ± 8.15 0.76 Hours for critical illness hyperglycemia to develop 97.77 ± 36.23 131.32 ± 55.99 ) 0.53 Frequency of blood glucose measurement 0.55 ± 0.130.64 ± 0.25 0.5 Total blood glucose measurement 36.25 ± 12.53 45.56 ± 19.76 0.12 Minimal blood glucose 69.83 ± 17.96 43.61 ± 24.67 0.009* Mean blood glucose 97.77 ± 36.23131.32 ± 55.99 0.13 Starting insulin infusion rate 0.72 ± 0.490.76 ± 0.47 0.76 Maintenance insulin infusion rate0.47 ± 0.470.5 ± 0.34 0.82 Peak insulin requirement1.05 ± 1.020.9 ± 0.51 0.5 Total insulin requirement in 1 st day0.42 ± 0.240.58 ± 0.42 0.22 Duration of insulin requirement11.75 ± 7.7518.83 ± 11.690.13 ● Mechanical Ventilation (no, %) 4 (33.3%) 16 (88.9%) 0.003* ● CVS Support (no, %) 8 (66.7%) 14 (77.8%) 0.4 ● Culture: Growth (no, %)3 (25%)6 (33.3%)0.47
:Comparison between the survivors and non-survivors in the studied patients Item Survivors N = 12 Non-survivors N = 18 p-value Length of stay (hours) ± ( ) ± ( ) 0.24 Max blood glucose ± ± Pediatric Logestic Organ Dysfunction Score 9.08 ± ± Hours for critical illness hyperglycemia to develop ± ± ) 0.53 Frequency of blood glucose measurement 0.55 ± ± Total blood glucose measurement ± ± Minimal blood glucose ± ± * Mean blood glucose ± ± Starting insulin infusion rate 0.72 ± ± Maintenance insulin infusion rate0.47 ± ± Peak insulin requirement1.05 ± ± Total insulin requirement in 1 st day0.42 ± ± Duration of insulin requirement11.75 ± ± ● Mechanical Ventilation (no, %) 4 (33.3%) 16 (88.9%) 0.003* ● CVS Support (no, %) 8 (66.7%) 14 (77.8%) 0.4 ● Culture: Growth (no, %)3 (25%)6 (33.3%)0.47")
25
Conclusion Although, not showing statistical significant differences, TGC was associated with higher mortality rates and more frequent hypoglycemic episodes compared with SGC (75% vs 50%). Moreover, it was associated with a significantly higher frequency of blood glucose measurement requiring higher costs. Thus, TGC might not be recommended for managing CIH.

26
Recommendations Examine and characterize the underlying pathophysiologic mechanisms behind stress hyperglycemia to prevent its adverse consequences. Conduct further studies to examine cut-off levels of blood glucose for controlling hyperglycemia taking in consideration the necessity of avoiding hypoglycemia and its serious effects.

27
TAKE HOME MESSAGE CIH and its glycaemic control have emerged as prominent issues in critical care. It is important to reassess cost-effectiveness of controlling hyperglycemia in the critically ill children; as IIT and monitoring certainly is more expensive than conventional therapy and monitoring. TGC was associated with increased frequency of hypoglycemic attacks that require more frequent monitoring, in addition to its increased rate of mortality, it is recommended to use SGC as alternative.

28
References Preissig CM, Rigby RM. Hyperglycaemia results from beta-cell dysfunction in critically ill children with respiratory and cardiovascular failure: a prospective observational study Critical Care 2009, 13: 27. Yung M, Wilkins B, Norton L, Slater A. Glucose control, organ failure, and mortality in pediatric intensive care. Pediatr Crit Care Med. 2008; 9: 147–152. Halverson-Steele B. The influence of hyperglycaemia on outcome in children following cardiac surgery. Pediatric Critical Care Medicine 2005. Hirshberg E, Larsen G, Van Duker H. Alterations in glucose homeostasis in the pediatric intensive care unit: Hyperglycemia and glucose variability are associated with increased mortality and morbidity. Pediatr Crit Care Med 2008; 9: 361-366. Preissig CM, Rigby RM. A disparity between physician attitudes and practice regarding hyperglycemia in pediatric intensive care units in the United States: a survey on actual practice habits. Crit Care 2010, 14: 11. Preissig CM, Hansen I, Roerig P-L, Rigby MR. A protocolized approach to identify and manage hyperglycemia in a pediatric critical care unit. Pediatr Crit Care 2009; 15: 127. Srinivasan V, Spinella PC, Drott HR, Roth CL, Helfaer MA, Nadkarni V. Association of timing, duration, and intensity of hyperglycemia with intensive care unit mortality in critically ill children. Pediatr Crit Care Med. 2004; 5: 329–336. Macrae D, Pappachan J, Grieve R, et al. Control of Hyperglycaemia in Paediatric Intensive Care (CHiP): study protocol. BMC Pediatr 2010;10:5.
: study protocol. BMC Pediatr 2010;10:5..")
29
My thanks and grateful appreciation to Prof Dr. Isis Ghali, Prof Dr. Mona Hafez, Prof Dr. Mona Mammdouh who shared me their valuable remarks and advice and offered great help and guidance to prepare such work.

Similar presentations






>")
 Fellow of KIMS Endocrine, Diabetes and Metabolism.>")


![MODELING METHOD Glucose-Insulin System Model CLINICAL DATA DATA: Are taken from the SPRINT [3] TGC cohort totalling 393 patients and ~40,000 patient hours.](/14/4293157/big_thumb.jpg "MODELING METHOD Glucose-Insulin System Model CLINICAL DATA DATA: Are taken from the SPRINT [3] TGC cohort totalling 393 patients and ~40,000 patient hours.>")













 Trial Adverse Event Reporting Catherine Dillon.>")