Download presentation
Presentation is loading. Please wait.

1
Ventilator-associated Pneumonia Among Elderly Medicare Beneficiaries in Long-term Care Hospitals William Buczko, Ph.D. Research Analyst Centers for Medicare & Medicaid Services

2
Introduction Ventilator-associated pneumonia (VAP) refers to nosocomial pneumonia occurring in patients receiving mechanical ventilation 48 hours or more after airway intubation. It is a common complication of care that affects approximately one fourth of patients receiving mechanical ventilation and often produces excess (and likely avoidable) length of stay, mortality and treatment costs (Kollef, 2005; Chastre and Fagon, 2002). VAP is the leading cause of nosocomial mortality for patients with respiratory failure (Kollef, 2005). Males, trauma patients and severely ill patients are at increased risk for VAP (Chastre and Fagon, 2002; Kollef, 2005). Many VAP cases are preventable if appropriate interventions are in place.
 length of stay, mortality and treatment costs (Kollef, 2005; Chastre and Fagon, 2002). VAP is the leading cause of nosocomial mortality for patients with respiratory failure (Kollef, 2005). Males, trauma patients and severely ill patients are at increased risk for VAP (Chastre and Fagon, 2002; Kollef, 2005). Many VAP cases are preventable if appropriate interventions are in place..")
3
DATA MEDPAR discharge data for LTCHs are examined for Medicare fee-for-service beneficiaries who were discharged during CY 2004 with a procedure code of 96.72 (continuous mechanical ventilation for 96 consecutive hours or more) to avoid early onset infections that may have begun prior to the LTCH admission (N=13,759). Patients with a diagnosis of ICD-9-CM codes 481.xx – 486.xx were classified as having VAP present.

4
Comorbidities Patients with a diagnosis of ICD-9-CM codes 584.xx – 586.xx were classified as having renal failure present. Patients with a diagnosis of ICD-9-CM codes 250.xx were classified as having diabetes present. Patients with a diagnosis of ICD-9-CM codes 401.xx – 405.xx were classified as having hypertension present. Patients with a diagnosis of ICD-9-CM codes 430.xx – 438.xx were classified as having stroke present. Patients with a diagnosis of ICD-9-CM codes 490.xx – 496.xx were classified as having chronic obstructive pulmonary disease (COPD) present. Patients with a diagnosis of ICD-9-CM code 428 were classified as having congestive heart failure (CHF) present.
 present. Patients with a diagnosis of ICD-9-CM code 428 were classified as having congestive heart failure (CHF) present..")
13
Survival Proportional Hazards Two Year Post-Discharge Mortality Model Standard Hazard Predictors Coefficient Error T Ratio Age 0.02510.001025.25 1.025 Female -0.09620.0205 -4.69 0.908 Black 0.19550.0250 7.81 1.216 Hispanic 0.14610.0664 2.20 1.157 VAP -0.02800.0237-1.18 0.972 Renal Failure 0.31720.024712.84 1.373 Diabetes -0.0746 0.0287 -2.60 0.928 Hypertension 0.03320.0233 1.42 1.034 Stroke -0.13960.0476 -2.93 0.870 Chronic Obstructive Pulmonary 0.04810.0205 2.35 1.049 Disease Congestive Heart Failure 0.1284 0.0208 6.18 1.137 N = 13,759 Likelihood Ratio X2 = 1,082.25 with 11 Degrees of Freedom

14
Length of Stay Effects of VAP and other Comorbidities on Length of Stay Standard Predictors Coefficient Error T. Age -0.0639 0.0294 -2.17 Female 0.4197 0.6635 0.63 Black 0.9570 0.8362 1.14 Hispanic 1.9004 2.2316 0.85 VAP 2.4054 0.7691 3.13 Renal Failure 1.8517 0.8440 2.19 Diabetes -1.8961 0.9113 -2.08 Hypertension -3.0587 0.7616 -4.02 Stroke -2.4759 1.4989 -1.65 Chronic Obstructive Pulmonary -0.5111 0.6675 -0.77 Disease Congestive Heart Failure 1.2193 0.6842 1.78 Intercept48.2573 N = 13,759, R2 = 0.004, F= 4.84 with (11, 13,747) Degrees of Freedom
 Degrees of Freedom.")
15
Medicare Covered Charges Effects of VAP and other Comorbidities on Total Medicare Covered Charges Standard Predictors Coefficient Error T. Age - 65.50 135.3 -0.48 Female 620.023,051.1 0.20 Black 11,426.003,845.7 2.97 Hispanic 36,959.00 10,263.0 3.60 VAP 14,883.003,537.1 4.21 Renal Failure 27,885.003,881.4 7.18 Diabetes -20,539.00 4,191.0 -4.90 Hypertension - 729.193,502.6 -0.21 Stroke -30,536.006.893.2 -4.43 Chronic Obstructive Pulmonary - 2,358.263,069.5 -0.77 Disease Congestive Heart Failure 12,491.003,146.4 3.97 Intercept 176,235.0 N = 13,759, R2 = 0.012, F= 15.07 with (11, 13,747) Degrees of Freedom
 Degrees of Freedom.")
16
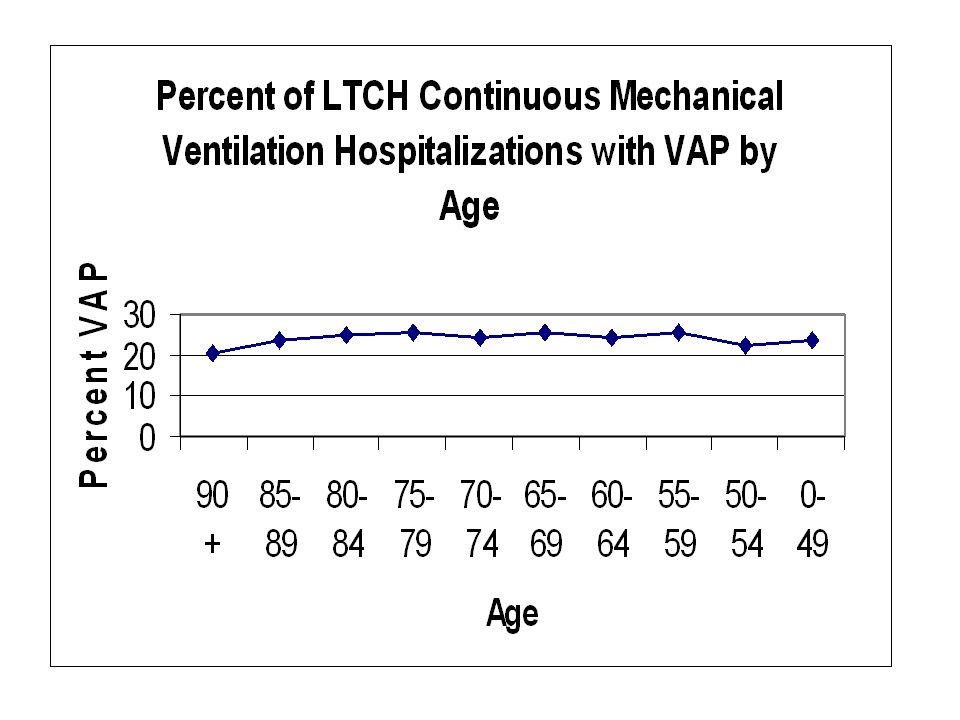
Summary The data indicate that LTCHs have an incidence rate of VAP that is similar to if not greater than that found in inpatient short stay facilities and home care settings. These findings suggest that VAP was not associated with increased mortality in LTCHs and is consistent with the findings of Kollef, et al. (1995), Bregeon, et al. (2001) and Rello, et al. (2002) among short stay inpatients. Since the data show no correlation of VAP incidence with increasing age, each of the comorbidities examined except COPD, and number of comorbid conditions, patients acquiring VAP appear to be no more frail or infirm than ventilator patients without VAP. Similarly, patients with VAP have lower in-LTCH mortality rates and post-discharge mortality rates than patients without VAP. LTCH ventilator patients with VAP consume more resources and generate higher costs than other ventilator patients. This finding is consistent with the excess resource consumption and billed charges found among short stay inpatients with VAP (Rello, et al. 2002). One should be concerned about the high rate of VAP among Medicare LTCH ventilator patients and that a substantial portion of their excess length of stay and Medicare charges may well be avoidable through improved management of ventilator patients and improved quality of care.
, Bregeon, et al. (2001) and Rello, et al. (2002) among short stay inpatients. Since the data show no correlation of VAP incidence with increasing age, each of the comorbidities examined except COPD, and number of comorbid conditions, patients acquiring VAP appear to be no more frail or infirm than ventilator patients without VAP. Similarly, patients with VAP have lower in-LTCH mortality rates and post-discharge mortality rates than patients without VAP. LTCH ventilator patients with VAP consume more resources and generate higher costs than other ventilator patients. This finding is consistent with the excess resource consumption and billed charges found among short stay inpatients with VAP (Rello, et al. 2002). One should be concerned about the high rate of VAP among Medicare LTCH ventilator patients and that a substantial portion of their excess length of stay and Medicare charges may well be avoidable through improved management of ventilator patients and improved quality of care..")
Similar presentations







 Dr Ian Williams Greater Metro South Brisbane Medicare.>")
 Lee Feb. 9 th, 2007.>")

















