Download presentation
Presentation is loading. Please wait.

1
Case 324 SH/EAH Workshop - Huston TX, 24-26 October 2013 Leonardo Boiocchi, M.D. & Attilio Orazi, M.D. Weil Cornell Medical College, New York, NY Università degli Studi di Brescia, Italy

2
Clinical history (August 2009) 73 y/o woman. Diagnosis of PV in 1987 Treatment: anagrelide for two yrs, then hydroxyurea plus phlebotomies (2-4 per year) until 2009 Since 2009 no therapy or phlebotomies because of anemia and decreased hematocrit (36%) Diagnosis of post-PV myelofibrosis in August 2009 Since 2009, increasing persistent leukocytosis (WBC >30x10 9 /L), increased splenomegaly, and weight loss No response to treatment with IFN, JAK2 inhibitor (Incyte) or non-selective histone deacetylase inhibitor (pabinostat)
 until 2009 Since 2009 no therapy or phlebotomies because of anemia and decreased hematocrit (36%) Diagnosis of post-PV myelofibrosis in August 2009 Since 2009, increasing persistent leukocytosis (WBC >30x10 9 /L), increased splenomegaly, and weight loss No response to treatment with IFN, JAK2 inhibitor (Incyte) or non-selective histone deacetylase inhibitor (pabinostat).")
3
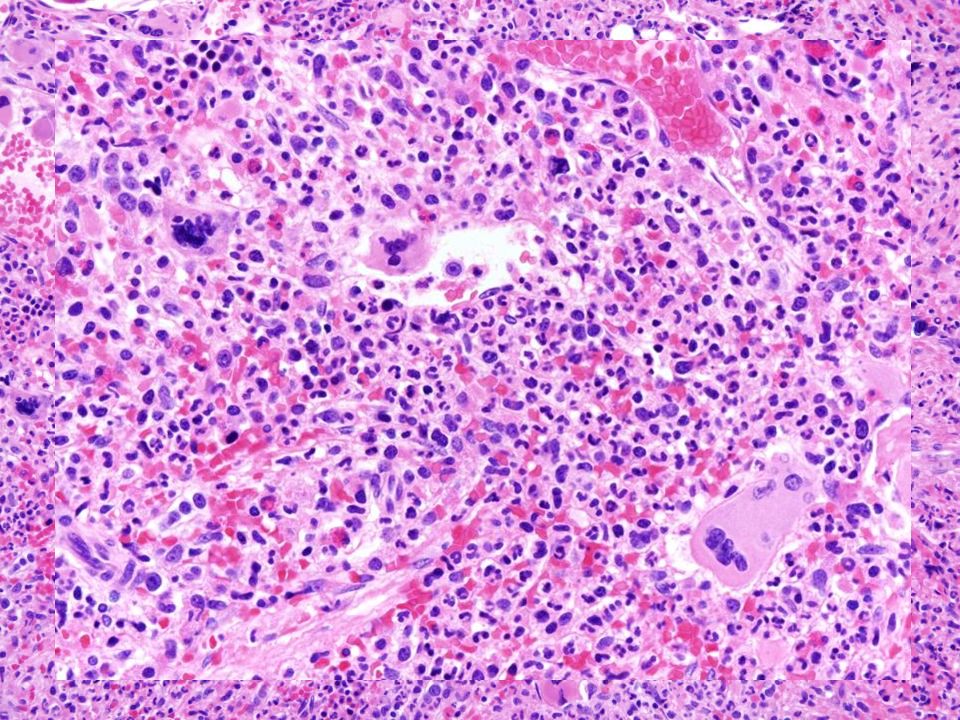
BM, April 2010

5
MF-3

6
Molecular studies: JAK2V617F positive (allele burden not performed) Cytogenetics: 46,XX,del(13)(q12q14)[9]/46,XX,+add(1)(p11),-6[8]/46,X, -X,+2,del(4) (q21)[2] Multiple clones (absent during polycythemic phase) and no Philadelphia chromosome Previous cytogenetic results (June 2009, post-PV MF): 46,XX,del(13)(q12q14)[14]/46,idem,+add(1)(p11),-6[5]/ 46,idem,del(4)(q21)[1] BM, April 2010
![Molecular studies: JAK2V617F positive (allele burden not performed) Cytogenetics: 46,XX,del(13)(q12q14)[9]/46,XX,+add(1)(p11),-6[8]/46,X, -X,+2,del(4) (q21)[2] Multiple clones (absent during polycythemic phase) and no Philadelphia chromosome Previous cytogenetic results (June 2009, post-PV MF): 46,XX,del(13)(q12q14)[14]/46,idem,+add(1)(p11),-6[5]/ 46,idem,del(4)(q21)[1] BM, April 2010](http://images.slideplayer.com/39/10886987/slides/slide_6.jpg "Molecular studies: JAK2V617F positive (allele burden not performed) Cytogenetics: 46,XX,del(13)(q12q14)[9]/46,XX,+add(1)(p11),-6[8]/46,X, -X,+2,del(4) (q21)[2] Multiple clones (absent during polycythemic phase) and no Philadelphia chromosome Previous cytogenetic results (June 2009, post-PV MF): 46,XX,del(13)(q12q14)[14]/46,idem,+add(1)(p11),-6[5]/ 46,idem,del(4)(q21)[1] BM, April 2010")
7
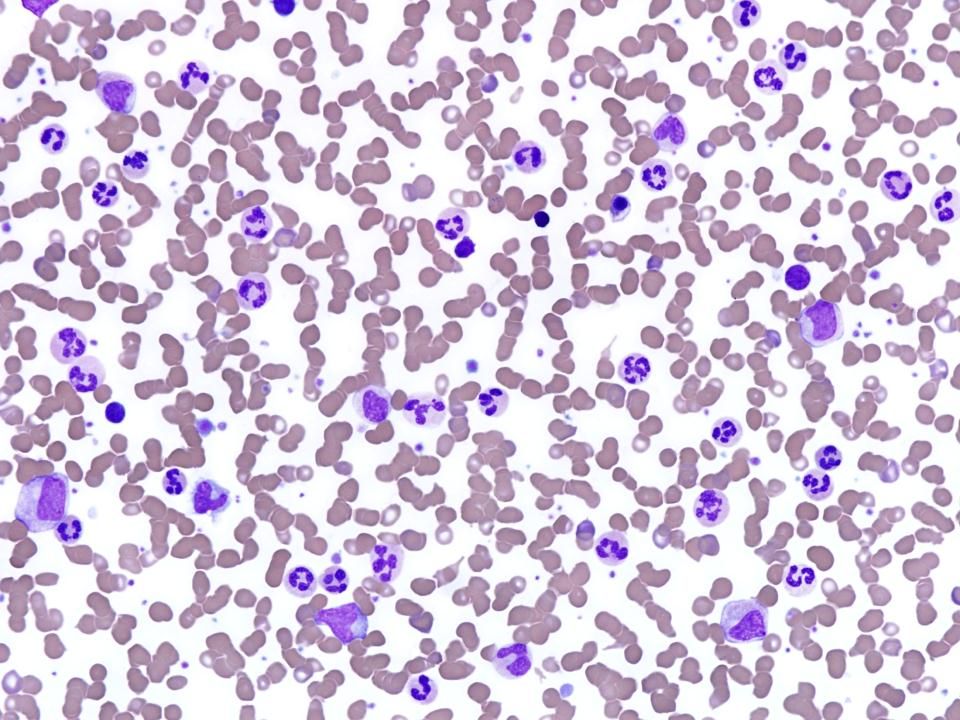
PB smear, April 2010 CBC: Hb: 10.5 g (MCV: 88.3fl); WBC: 50.2x10 9 /L (N 67%; Band 8%; Meta 6%; Myelo 9%; Promyelo 1%; Eos 1%; Baso 2%; Blasts 1%; Mono 1%; Lymph 4%); 1% NRBC; Plts: 192x10 9 /L
; WBC: 50.2x10 9 /L (N 67%; Band 8%; Meta 6%; Myelo 9%; Promyelo 1%; Eos 1%; Baso 2%; Blasts 1%; Mono 1%; Lymph 4%); 1% NRBC; Plts: 192x10 9 /L")
10
Final diagnosis: bone marrow Post-polycythemic myelofibrosis, associated with neutrophilic proliferation

11
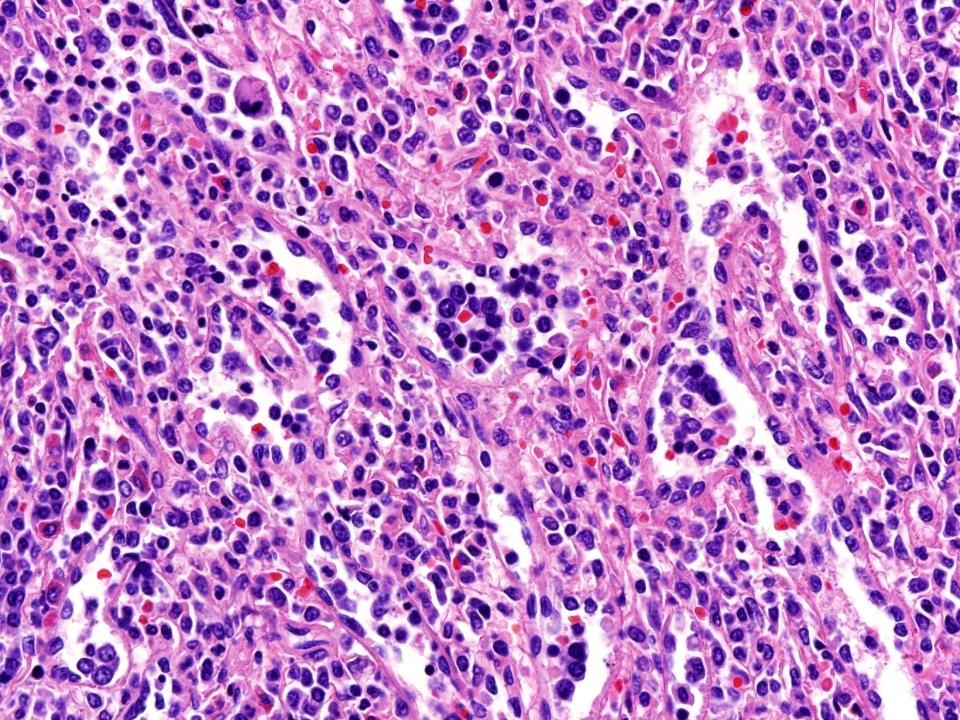
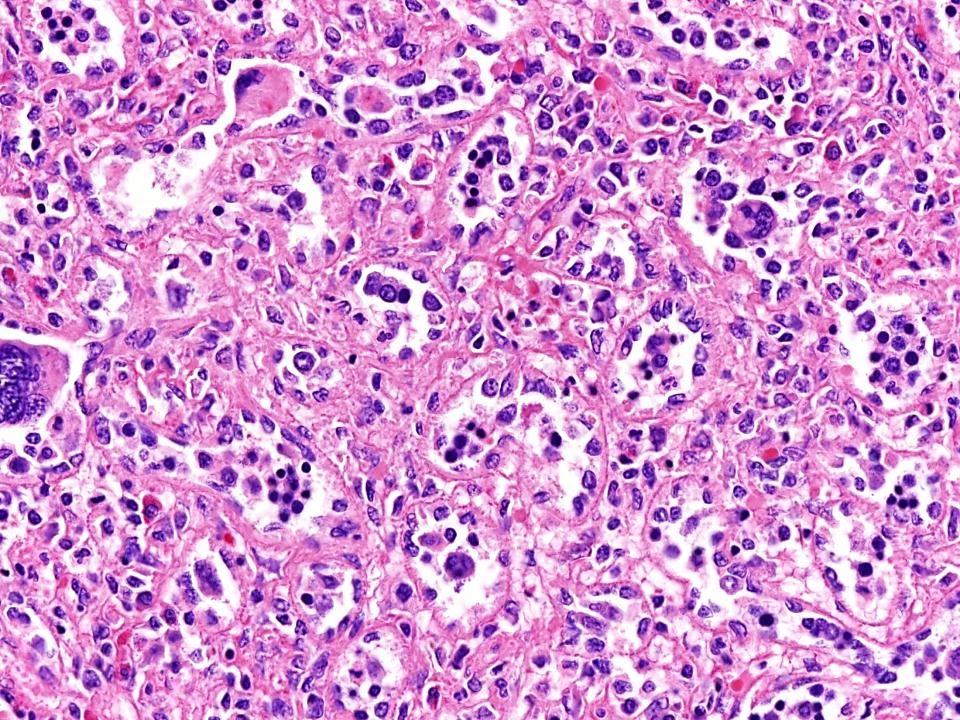
June 2010: treatments ineffective, palliative splenectomy Spleen, June 2010

14
MPO 2% blasts (confirmed by flow) - - - - - - - - - - - JAK2V617F + Complex karyotype
 JAK2V617F + Complex karyotype")
15
Spleen histology interpretation “Expanded splenic red pulp with extensive extramedullary hematopoiesis, characterized predominantly by a maturing granulocytic proliferation largely neutrophilic, associated with foci of megakaryopoiesis and predominantly intrasinusoidal erythropoiesis. No blast accumulation is appreciated although MPO immunostain highlights the presence of an increased proportion of promyelocytes.”

16
Case fulfills 2008 WHO criteria for Post-PV MF It does not represent a classical accelerated phase (no increased blasts) Persistence of significant neutrophilic leukocytosis associated with an increased proportion (>10%) of circulating immature myeloid cells is consistent with disease progression Comments
 Persistence of significant neutrophilic leukocytosis associated with an increased proportion (>10%) of circulating immature myeloid cells is consistent with disease progression Comments")
17
Additional Cases Inclusion criteria: Post-PV MF diagnosis Sustained neutrophilia (>3 months) with exclusion of reactive conditions or steroids therapy Two thresholds for neutrophilia: >13x10 9 /L with dysgranulopoiesis >25x10 9 /L without dysgranulopoiesis Nine cases collected from 2 institutions (WCMC, NY and Ospedale Policlinico of Milan, Italy)
 with exclusion of reactive conditions or steroids therapy Two thresholds for neutrophilia: >13x10 9 /L with dysgranulopoiesis >25x10 9 /L without dysgranulopoiesis Nine cases collected from 2 institutions (WCMC, NY and Ospedale Policlinico of Milan, Italy)")
18
Pt. #Sex Age (yrs) Diagnosis PV duration (yrs) WBC x10 9 /L Neutrophils x10 9 /L (%) BM Blasts (%) Splenomegaly 1M88 PV, early fibrotic phase 2099.493.4 (94)0%yes 2F53post-PV MF917.513.1 (75)0%no 3*F73post-PV MF2350.233.6 (67)1%yes 4M70post-PV MF489.770.9 (79)0%no 5M67post-PV MF422.218.6 (84)2%yes 6M76post-PV MF1729.525.6 (87)1%no 7M75post-PV MF1519.716.5 (84)1%yes 8 M64post-PV MF103025.2 (84)1%yes 9F72 PV, early fibrotic phase 1731.927.1 (85)0%yes Clinical data *In bold the presented case.
 Diagnosis PV duration (yrs) WBC x10 9 /L Neutrophils x10 9 /L (%) BM Blasts (%) Splenomegaly 1M88 PV, early fibrotic phase (94)0%yes 2F53post-PV MF (75)0%no 3*F73post-PV MF (67)1%yes 4M70post-PV MF (79)0%no 5M67post-PV MF (84)2%yes 6M76post-PV MF (87)1%no 7M75post-PV MF (84)1%yes 8 M64post-PV MF (84)1%yes 9F72 PV, early fibrotic phase (85)0%yes Clinical data *In bold the presented case..")
19
Pt. #DiagnosisJAK2CytogeneticsFollow-up 1 PV, early fibrotic phase V617F47,XY,+8[5]/46,XY[15]na 2 post-PV MF V617Fnormalhealthy 3* post-PV MF V617F 46,XX,del(13)(q12q14)[14]/46,idem,+add(1)(p11), -6[5]/ 46,idem,del(4)(q21)[1] dead 4 post-PV MF V617Fnormal Transfusion dependent, worsening 5 post-PV MF V617Fnadead 6 post-PV MF V617Fnormalhealthy 7 post-PV MF V617F47XY,+der(1;9)(q10;p10)[17]/47XY,+9[2]healthy 8 post-PV MF V617Fnahealthy 9 PV, early fibrotic phase V617F 46XX, del(20)(q11.2) [15]/48XXX, +9, del(20)(q11.2)[2] healthy Molecular results and follow-up *In bold the presented case.
(q12q14)[14]/46,idem,+add(1)(p11), -6[5]/ 46,idem,del(4)(q21)[1] dead 4 post-PV MF V617Fnormal Transfusion dependent, worsening 5 post-PV MF V617Fnadead 6 post-PV MF V617Fnormalhealthy 7 post-PV MF V617F47XY,+der(1;9)(q10;p10)[17]/47XY,+9[2]healthy 8 post-PV MF V617Fnahealthy 9 PV, early fibrotic phase V617F 46XX, del(20)(q11.2) [15]/48XXX, +9, del(20)(q11.2)[2] healthy Molecular results and follow-up *In bold the presented case..")
20
1.Progression to a neutrophilic predominant proliferative pattern can be observed in a proportion of post-PV MF 2.Rare: 3% of all PV cases 3.It could represent a yet not clearly established manifestation of acceleration similar to what recently reported in cases of primary myelofibrosis developing sustained monocytosis Conclusions

21
References Billio A, et al. Chronic neutrophilic leukemia evolving from polycythemia vera with multiple chromosome rearrangements: a case report. Haematologica. 2001;86(11):1225-1226. Boiocchi L, et al. Development of monocytosis in patients with primary myelofibrosis indicates an accelerated phase of the disease. Mod Pathol. 2013;26(2):204-12. Maxson JE, et al. Oncogenic CSF3R mutations in chronic neutrophilic leukemia and atypical CML. N Engl J Med. 2013;368(19):1781-1790. Pardanani A, et al. CSF3R T618I is a highly prevalent and specific mutation in chronic neutrophilic leukemia. Leukemia. 2013 Apr 22. doi: 10.1038/leu.2013.122
: Boiocchi L, et al. Development of monocytosis in patients with primary myelofibrosis indicates an accelerated phase of the disease. Mod Pathol. 2013;26(2): Maxson JE, et al. Oncogenic CSF3R mutations in chronic neutrophilic leukemia and atypical CML. N Engl J Med. 2013;368(19): Pardanani A, et al. CSF3R T618I is a highly prevalent and specific mutation in chronic neutrophilic leukemia. Leukemia Apr 22. doi: /leu")
Similar presentations








II Dr. Ibrahim. A. Adam.>")
 Verstovsek M.D., Ph.D. Professor of Medicine Department of Leukemia University of Texas MD Anderson Cancer Center Houston, Texas, USA Therapy.>")


 Myelodysplastic / myeloproliferative diseases (MDS/MPD) >")




 - Essential Thrombocythemia - Myelofibrose Myeloid Methaplasia.>")

>")
