Download presentation
Presentation is loading. Please wait.

1
Jeffrey Borkan, MD, PhD & Paul George, MD, MHPE
The New Primary Care – Population Medicine Program at Brown University: Training the workforce we need for the triple aim Jeffrey Borkan, MD, PhD & Paul George, MD, MHPE Assistant Deans for Primary Care – Population Medicine and Curriculum Department of Family Medicine Alpert Medical School of Brown University The overall topic for the meeting is creation of next generation health systems based on advanced primary care, partnering with public health and patients. One focus will be the health system in Wuhou District, Chengdu, China, which has been designated a demonstration site to build PCMH in their community health (primary care) center, linked to their very hospital-centric main system of care. Another will be the new practice we are developing in Salt Lake City, designed from the “outside in” based on community needs and with an advanced interdisciplinary team designed to care for the population. We’ll also likely have some other demonstration sites to consider. This kind of transformation requires a convergence of public health, community and patient leadership, interdisciplinary teams, health professions training (family medicine, PAs, care managers, health educators, etc.), IT, chronic care programs, payment models, etc. We think of this as next generation care, or sometimes “PCMH 3.0.” At the meeting we will have a variety of people interested in these issues. For example, from China we’ll have medical, government, IT, economics, clinic, and family medicine residency leaders. From the US, health system, public health, nurse care managers, and others. Paul Grundy will keynote, and others from IBM Watson will provide perspective on advanced IT, Glen Stream will speak about FMAH, Andrew Morris-Singer of Primary Care Progress on interdisciplinary team training, Jed Constantz of EAHCS on measuring high value primary care providers. So, in this context, your perspective on evolution of family medicine education to support health care transformation (with a nod to FMAH as appropriate?), including your MD-ScM program and strategic directions led by CAFM, would be terrific. And actually, anything you feel inspired to talk about would be more than welcome! I am quite confident that your always-thoughtful input into the conversation throughout the meeting will be a great contribution.
 center, linked to their very hospital-centric main system of care. Another will be the new practice we are developing in Salt Lake City, designed from the outside in based on community needs and with an advanced interdisciplinary team designed to care for the population. We’ll also likely have some other demonstration sites to consider. This kind of transformation requires a convergence of public health, community and patient leadership, interdisciplinary teams, health professions training (family medicine, PAs, care managers, health educators, etc.), IT, chronic care programs, payment models, etc. We think of this as next generation care, or sometimes PCMH 3.0. At the meeting we will have a variety of people interested in these issues. For example, from China we’ll have medical, government, IT, economics, clinic, and family medicine residency leaders. From the US, health system, public health, nurse care managers, and others. Paul Grundy will keynote, and others from IBM Watson will provide perspective on advanced IT, Glen Stream will speak about FMAH, Andrew Morris-Singer of Primary Care Progress on interdisciplinary team training, Jed Constantz of EAHCS on measuring high value primary care providers. So, in this context, your perspective on evolution of family medicine education to support health care transformation (with a nod to FMAH as appropriate ), including your MD-ScM program and strategic directions led by CAFM, would be terrific. And actually, anything you feel inspired to talk about would be more than welcome! I am quite confident that your always-thoughtful input into the conversation throughout the meeting will be a great contribution.")
2
Outline Need for a new kind of primary care physician Intellectual basis for the PC-PM program Medical school exemplars in healthcare transformation education Primary Care-Population Medicine Program at the Alpert Medical School of Brown University

3
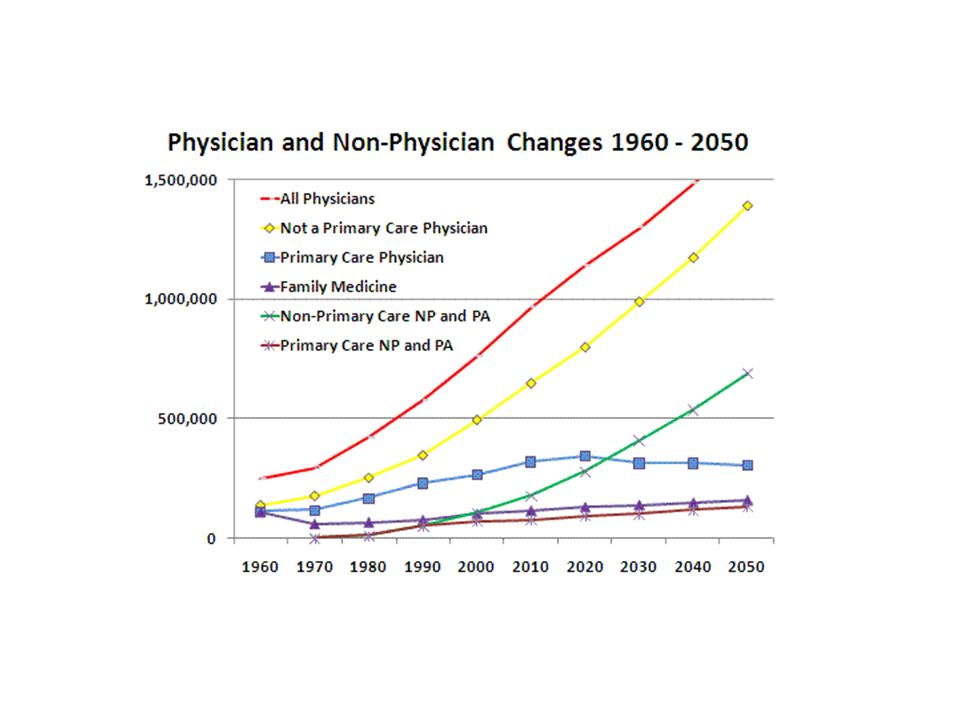
Why the Need? Rapid changes in the US healthcare system have accelerated the need for physicians trained in the care of individuals, families, communities, and populations The projected shortage of primary care physicians is a major impediment to achievement of the Triple Aim The United States healthcare system has been in a period of rapid evolution over the past decade, a trend that is anticipated to continue for the foreseeable future. Physicians are increasingly responsible for the quality and cost of care they provide, and are being held accountable not just for the patient in front of them, but also for the outcomes of their patient panels, communities, and populations.

4
United States Health Care 2016
Most technologically advanced, responsive, and expensive healthcare in the world Poor health outcomes Non-system system Perverse Incentives >7% uninsured & 23% underinsured Fragmented, disorganized, lacking coordination Commonwealth Fund 2015 BOX #1. WHO IS UNDERINSURED?In this analysis, we use a measure of underinsurance that takes into account an insured adult’s reported out-of-pocket costs over the course of a year, not including premiums, and the health plan deductible. The measure was developed by Cathy Schoen and first used in The Commonwealth Fund’s 2003 Biennial Health Insurance Survey. These actual expenditures and the potential risk of expenditures, as represented by the deductible, are then compared with household income. Specifically, someone who is insured all year is underinsured if: out-of-pocket costs, excluding premiums, over the prior 12 months are equal to 10 percent or more of household income; or out-of-pocket costs, excluding premiums, are equal to 5 percent or more of household income if income is under 200 percent of the federal poverty level ($22,980 for an individual and $47,100 for a family of four); or deductible is 5 percent or more of household income. The out-of-pocket cost component of the measure is only triggered if a person uses his or her plan. The deductible component provides an indicator of the financial protection the plan offers and the risk of incurring costs even before a person uses the plan. The definition does not include people who are at risk of incurring high costs because of other design elements, such as exclusion of certain covered benefits and copayments. It therefore provides a conservative measure of underinsurance in the United States.
; or. deductible is 5 percent or more of household income. The out-of-pocket cost component of the measure is only triggered if a person uses his or her plan. The deductible component provides an indicator of the financial protection the plan offers and the risk of incurring costs even before a person uses the plan. The definition does not include people who are at risk of incurring high costs because of other design elements, such as exclusion of certain covered benefits and copayments. It therefore provides a conservative measure of underinsurance in the United States.")
5
Triple Aim

7
US entering residency classes – 2016: 14.5 % (NRMP)
US % & shrinking US entering residency classes – 2016: 14.5 % (NRMP)
")
8
The Intellectual Basis of Family Practice J Fam Pract. 1975 2(6):423-8
The sine qua non of family practice is the knowledge and skill which allow the family physician to confront relatively large numbers of unselected patients with unselected conditions and to carry on therapeutic relationships with patients over time. The Intellectual Basis of Family Practice J Fam Pract. 1975 2(6):423-8 G. Gayle Stephens, MD Although progress is being made toward defining the family physician and the specialty of family practice, there remains a need to describe more clearly a conceptual base for family medicine as an academic discipline.
: G. Gayle Stephens, MD. Although progress is being made toward defining the family physician and the specialty of family practice, there remains a need to describe more clearly a conceptual base for family medicine as an academic discipline.")
9
The Need for a New Medical Model: a Challenge for Biomedicine. Science
George Engel , MD

10
The Case for Primary Care
There is now good evidence, from a variety of studies at national, state, regional, local, and individual levels that good primary care is associated with better health outcomes (on average), lower costs (robustly and consistently), and greater equity in health. Barbara Starfield, MD, MPH
, lower costs (robustly and consistently), and greater equity in health. Barbara Starfield, MD, MPH.")
11
Institute of Medicine Report 2012
“Although primary care and public health share a goal of promoting the health and well-being of all people, these two disciplines historically have operated independently of one another. …new opportunities are emerging for bringing the sectors together in ways that will yield substantial and lasting improvements in the health of individuals, communities, and populations.”

12
Health Systems Science
Goal Preparing students for 21st Century practice in the broader context of patient’s lives and population health Seamlessly integrating with the First Science and the Second Science Third Science of Medicine Third Science of Medical Education Third medical science should ideally synergize, complement, and be integrated with the core content and concepts of the first two sciences -- basic and clinical sciences Health Systems Science

13
Health Systems Science Definition
Principles, methods, and practice of improving quality, outcomes, and costs of healthcare delivery for patients and populations within systems of medical care Conceptualized as factors that impact the health outcomes for individual patients and populations of patients beyond the basic and clinical sciences

14
Health Systems Science
Domains for Curriculum Design Population Health Informatics Health Determinants Policy Quality JED Practice Improvement Other Teamwork High-Value Care

15
Core Strategies: Ensure a well-trained primary care workforce
Ensure every person will have a personal relationship with a trusted family physician or other primary care professional, in the context of a medical home Increase the value of primary care Reduce health care disparities Lead the continued evolution of the patient-centered medical home Ensure a well-trained primary care workforce Improve payment for primary care by moving away from fee for service and towards comprehensive primary care payment

16
Transforming Training to Build the Family Physician Workforce Our Country Needs Hughes, et. al. Family Medicine 2015;47(8):620-7.) Reforms are needed across the entire educational continuum, including how we recruit, train, and help practicing family physicians refresh their skills Must provide opportunities to acquire skills needed in new practice and payment environments develop effective interprofessional training, and to design educational programs that are socially accountable to the patients, families, and communities we serve

17
Medical School Exemplars in Training for Healthcare Transformation
University of New Mexico: health extension services School of Community Medicine at the University of Oklahoma-Tulsa: health of the community Duke University: Primary Care Leadership Track Penn State: health system science including a navigator program Mayo Clinic: Science of Health Care Delivery Brown: Primary Care – Population Medicine Program

18
Health Extension Rural Offices (HERO) in New Mexico: An Academic Health Center and the Social Determinants of Disease
 in New Mexico: An Academic Health Center and the Social Determinants of Disease")
19
Mayo Medical School Innovative Science of Health Care Delivery curriculum, in which students learn how health care systems work Students earn a certificate in the Science of Health Care Delivery upon graduation

20
The New Primary Care-Population Medicine Program at Alpert Medical School

21
A Vision for the Program
A bold and innovative scholarly program that trains “clinicians-plus” with a primary care and population medicine focus 4-year program– dual degree MD-ScM Research requirement in primary care, population medicine, and health policy Interdisciplinary and leadership training Methods for integrated, active learning Up to 24 students per class Building an airplane while flying it

22
Basic Science, Clinical Medicine & Population Medicine
Readies students for leadership roles in health care on the local, state, or national level ranging in areas from: Primary Care Clinical Service Population Health Research Education Health Policy

23
The Four Year Continuum:
Active Learning/Flexibility/Creativity/Scholarship Basic Sciences and Population Medicine Clinical Sciences and Population Medicine

24
Specific Curricular Elements
Longitudinal Integrated Clerkship (LIC) 32 weeks of LIC with weekly outpatient (Pediatrics, IM, FM, OB-GYN, Surgery, Psychiatry/ Neurology) sessions Inpatient experiences based on curricular needs (total 12 weeks starting with a 6 week Med-Surg immersion) Students in groups that meet for tailored didactics, morning reports, and special activities (e.g., homeless and incarceration medicine) ScM in Population Medicine 9 course integrated curriculum Special journal club and group activities Scholarly work related to PC-PM with thesis requirement 5th Year (research fellow status), if needed
 32 weeks of LIC with weekly outpatient (Pediatrics, IM, FM, OB-GYN, Surgery, Psychiatry/ Neurology) sessions. Inpatient experiences based on curricular needs (total 12 weeks starting with a 6 week Med-Surg immersion) Students in groups that meet for tailored didactics, morning reports, and special activities (e.g., homeless and incarceration medicine) ScM in Population Medicine. 9 course integrated curriculum. Special journal club and group activities. Scholarly work related to PC-PM with thesis requirement. 5th Year (research fellow status), if needed.")
25
Year 1 Aug Sept Oct Nov Dec Jan Feb Mar Apr May June IMS I IMS II
Scientific Foundations of Med Brain Sciences SS Micro/ID Histology Gen Path Human Anatomy Head/Neck Anatomy SS Anat. Doctoring I Doctoring II (with extension into summer) Population Medicine I Population Medicine II (semester), III, IV, V (summer)
 Population Medicine I. Population Medicine II (semester), III, IV, V (summer)")
26
Clinical Skills Clerkship
Year 2 Aug Sept Oct Nov Dec Jan Feb Mar Apr May June IMS III IMS IV Cardio Renal Pulm End HR Heme GI USMLE Step 1 Begin Clerkships All blocks integrate systemic physiology, pathophysiology, pathology and pharmacology with relevant nutrition and genetics. Clinical Skills Clerkship Doctoring III Doctoring IV Population Medicine VI HR, Human Reproduction; End, Endocrine

27
Longitudinal Integrated Clerkship
Year 3 Quarter 1 Quarter 2 Quarter 3 Quarter 4 April May June July Aug Sept Oct Nov Dec Jan Feb Mar Longitudinal Integrated Clerkship Inpatient Internal Medicine Surgery Pediatrics Obstetrics & Gynecology Psychiatry/Neurology Family Medicine Population Medicine VI and VII

28
Sample Weekly Schedule

29
Subinternship(s) / Electives/ICU
Year 4 Residency Interviews June July Aug Sept Oct Nov Dec Jan Feb Mar April May Subinternship(s) / Electives/ICU Population Medicine IX Thesis Completion In Year 4, students will participate in elective rotations and a sub-internship offered at Alpert Medical School and complete their thesis
 / Electives/ICU. Population Medicine IX. Thesis Completion. In Year 4, students will participate in elective rotations and a sub-internship offered at Alpert Medical School and complete their thesis.")
30
Admissions Sought-after qualities, PC-PM matriculants:
Outstanding academic credentials – ability to excel in basic science, clinical, and population science Experience beyond college Experience in helping activities, advocacy, and social welfare Ability to function in teams Single (AMS) Brown Med application with extra essay Applicants must be admitted to (AMS) Brown Med Inclusion of Program in Liberal Medical Education (Brown), Early Identification programs, and Post-Bac
 Brown Med application with extra essay. Applicants must be admitted to (AMS) Brown Med. Inclusion of Program in Liberal Medical Education (Brown), Early Identification programs, and Post-Bac.")
31
Expected Products of the Program
Primary Care “clinicians plus” Halo effects – on faculty and mentors, physician groups, hospitals, and healthcare systems Diffusion of innovations to the categorical program Improvements in the outcomes, quality, and cost and the organization of healthcare in Rhode Island Strengthening of the bonds between the Medical School and the State Fostering further research in primary care, population medicine, and health policy Enhancements to Brown’s reputation

32
Evaluation: Early Key Findings
Methods: focus groups, surveys, student reps No differences in students applying to PC-PM program and traditional MD program Additional workload in PC-PM program not an issue (at least in first year) Students love the LIC model (piloted with students not in the PC-PM program)
 Students love the LIC model (piloted with students not in the PC-PM program)")
33
Steps for Second class of up to 24 students to began August 2016 LIC Pilot expands to 12 students starting May 2016 ScM courses in first and third years underway Seeking more sites & partners: primary care, outpatient, inpatient, systems Further evaluation of students, faculty, and program

34
Unfinished Business Ever more Sites & Partners: primary care, outpatient, inpatient, systems Financial Incentives for Students & Mentors Relationship with other parts of the University and other RI institutions Extending interprofessional education IT support for student’s patient panels More (saved) primary care residency slots
 primary care residency slots.")
35
Consortium Medical Schools
Alpert Medical School of Brown University Brody School of Medicine Indiana University Mayo Medical School New York University School of Medicine Oregon Health & Science University School of Medicine Penn State College of Medicine UC Davis School of Medicine UC San Francisco School of Medicine University of Michigan Medical School Vanderbilt University School of Medicine

36
What’s Next? The healthcare system is transforming more rapidly than medical education – how do we prepare students for the context in which they will work, and prepare them to adapt to and ideally lead the change?

37
For more information: Brown
For more information: Brown.edu/population-medicine (401) @BrownPopMed
")
Similar presentations