Download presentation
Presentation is loading. Please wait.

1
GROWTH & PUBERTAL ABNORMALITIES IN CHILDREN AND ADOLESCENTS WITH BETA THALASSEMIA Ashraf T Soliman MD PhD FRCP Professor of Paediatrics and Endocrinology

2
I-CET-A Course - Countries

5
Farag Talaat. http://ambassadors.net/archives/issue28/selected_studies2.htm

6
INDIA

7
Musallam K M et al. Haematologica 2013;98:833-844

8
Clinical complications profile of regularly transfused β-thalassemia major patients. Musallam K M et al. Haematologica 2013;98:833-844 ©2013 by Ferrata Storti Foundation Growth failure

9
Do Patients with Thalassemia have significant Growth and Pubertal Disorder? What is the Magnitude of these problems?

13
Genes Nutrition T4 Genes Nutrition GH – IGF-I T4 Genes Nutrition T4 GH-IGF-I Sex Steroids

16
How to Assess Growth Axis Measure Growth and bone age Measure IGF-I GH Stimulation test GHRH test History Nutrition Physical exam Anthropo metry

22
How to Assess Gonadal Axis Physical Exam Growth- Tanner Staging Testicle size, US ovary -uterus Bone age Basal Testosterone and T after HCG Basal Estradiol & Progesterone FSH- LH Basal + Pulsatile properties GnRH test History Tanner stage Growth

33
How to Investigate Short Thalassemic Patient GH stimulati on test IGF-I Generati on test Ca, PO4, ALP, Vit D, PTH IGF-I FBG, OGTT

34
Do Patients with Thalassemia have significant Growth and Pubertal Disorder? What is the Magnitude of these problems?

35
35 SURVEYS Prevalence of Growth & Pubertal Abnormalities in Patients with Thalassaemia Major ?

36
I. Growth and Pubertal Survey Qatar Egypt Iran Italy Cyprus Romania

37
Growth and Pubertal Surveys Country surveyGrowth DelayHypogonadism Cyprus35%32% Greece32%42% Italy---49% Egypt62%73% males, 42% females Qatar42%46% Romania54%77% males 41% females N. America----35% TIF30.8%40.5% Pediatr Endocrinol Rev. 2007 Dec;5(2):642-8.,& Clin Endocrinol (Oxf). 1995 Jun;42(6):581-6. Acta Endocrinologica (Buc), vol. I, no. 2, p. 201-212, 2005
:642-8.,& Clin Endocrinol (Oxf) Jun;42(6): Acta Endocrinologica (Buc), vol. I, no. 2, p ,")
38
QATAR SURVEY

39
39 HtSDS 49% < -2 83% < -1 17 % > -1 Alexandria Survey ( n = 120)
")
40
40 GVSDS < -1 in patients and controls

41
41 Thalassaemia (males) n = 45, all > 14 yr Age = 16.9 +/- 3.5 yr 73 % had test. vol < 3 ml
 n = 45, all > 14 yr Age = /- 3.5 yr 73 % had test. vol < 3 ml")
42
42 Age of Thelarche

43
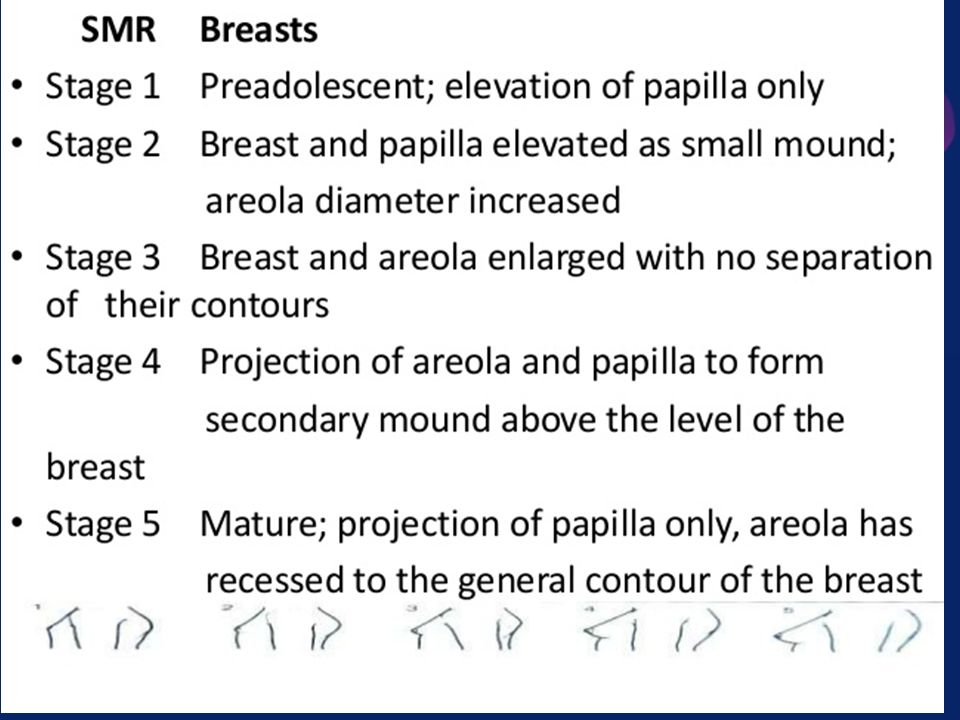
43 Thal: Breast Development n = 49, All >14 y Age = 17.2 +/- 3.2 yr 42 % --No breast development

44
44 Age of Menarche (years)
")
45
Qatar- Growth and Endocrine Complications in Thalassemic Children and Adolescents (6-18 years)
")
46
46 CONCLUSIONS Thalassaemia 49% had HtSDS <-2 and 83% <-1 73% of boys (>14 y) lack pubescent changes 42% of girls ( >14) lack pubescent changes
 lack pubescent changes 42% of girls ( >14) lack pubescent changes")
48
What is the Growth Pattern of these Patients ? Which Stage of Growth is more affected ?

50
Anita Saxena, Int J Hum Genet, 3(4): 237-246 (2003)
: (2003)")
51
Disturbed Upper /Lower segement because of short trunk due to vertebral pathology Anita Saxena, Int J Hum Genet, 3(4): 237-246 (2003)
: (2003)")
52
Weight Curves for Thalassemics Vs Normal Anita Saxena, Int J Hum Genet, 3(4): 237-246 (2003)
: (2003)")
53
Time of Growth Abnormalities 1. Late Childhood (Nutrition, GH-IGF-I, T4) 2. Pubertal Growth Spurt (attenuated) (Sex steroids, GH-IGF-I, Nutrition, T4, Insulin)
 (Sex steroids, GH-IGF-I, Nutrition, T4, Insulin).")
54
Summary Thalassemic patients are short Slow rate of linear growth +/- low body weight and BMI Delayed or absent pubertal spurt Growth faltering sets in earlier but becomes obvious after the age of 8 years

55
High Prevalence of short stature (Soliman et al., 1999; Low et al., 1998; Theodoridis et al., 1998; Caruso-Nicoletti, 1998; Roth et al., 1997; Kwan et al., 1995; Grundy et al., 1994). Truncal shortening: Rodda et al., 1995; Hamidah et al., 2001).
..")
56
Why patients with TM do not grow well ???

57
What is the effect of Intensive Chelation Therapy on Growth ? Started early-Positive effect on linear growth. 80% attained normal adult height ( Garcia-Mayor et al, Horm Res 1993; 40, 5.)
.")
58
??? Effectiveness of Different Transfusion Treatment Regimes Growth impairment and pubertal abnormalities in thalassemia major, has persisted despite major treatment advances. Chelation therapy may not always prevent or ameliorate late growth failure and/or delayed or absent puberty. (Chan et al. 2000; De Sanctis et al. 2000).
..")
59
POSSIBLE FACTORS AFFECTING GROWTH AND PUBERTY IN THALASSAEMIA Growth

60
Reported Endocrine abnormalities: Thalassaemia : 1.GH/IGF-I abnormalities 2.Hypogonadism(1ry, 2ry) 3.Thyroid dysfunction 4.IGT, IDDM 5.PTH deficiency
 3.Thyroid dysfunction 4.IGT, IDDM 5.PTH deficiency")
64
GH-IGF-I Growth Axis In Thalassemia Major

65
65 Studies / questions on GH /IGF-I in TM 1.GH response to provocation ? 2.Spontaneous GH secretion ? 3.IGF-I / BP3 secretion ? 4.IGF-I/BP3 generation in response to exogenous GH in these patients ? 5.GH-IGF-I response to blood transfusion 6.Effect of GH treatment on linear growth ?

66
66 Studies on GH-IGF-I axis Effect of associated hypogonadism, hypothyroidism, DM ? Nutrition effect on IGF-I secretion ? A natomy (MRI) of the hypothalamic/pituitary area in these patients ?
 of the hypothalamic/pituitary area in these patients .")
68
1. Do patients with Thalassemia have GH deficiency ?

69
Prevalence of GH deficiency in thalassemia Country Prevalence % Qatar –Doha ( n =81) 45% Egypt – Alexandria ( n = 120) 40% Egypt – Cairo ( n = 30) 33% Greece- Athens 38% Turkey-Izmir 40% Iran-Shiraz (n= 138) (53.5% ) boys, (46.5%) girls Italy - Ferrara ( adults) 8% males, 9% females Italy – Rome (adults) 32 % Italy- Milan (adults) 22% (severe) 19% (partial) J Endocrinol Invest. 2010 Sep;33(8):534-8. Epub 2010 Feb 15. Clin Endocrinol (Oxf). 2007 Nov;67(5):790-5. Epub 2007 Jul 3. IJMS. Vol 27, No. 2, June 2002 Arch Med Sci 2010; 6, 1: 90-95 J Trop Pediatr (1999) 45 (1): 23-30. J Trop Pediatr. 2002 Feb;48(1):50-4.
: Epub 2010 Feb 15. Clin Endocrinol (Oxf) Nov;67(5): Epub 2007 Jul 3. IJMS. Vol 27, No. 2, June 2002 Arch Med Sci 2010; 6, 1: J Trop Pediatr (1999) 45 (1): J Trop Pediatr Feb;48(1):")
70
70 Thal : GH after stimulation 40% of patients had peak GH < 7 Ug/L

72
Short Thalassemic With Normal GH response to provocation 2. Do they secrete normal GH spontaneously at night ??

73
73 Thal : Nocturnal GH (patient-1) and age-matched control 0 5 10 15 20 25 30 89 10 11 121314151617181920 GH Patient 1 Control
 and age-matched control GH Patient 1 Control")
74
74 Thal: Nocturnal GH secretion (patient -2) vs control Patient 2 Control
 vs control Patient 2 Control")
75
Tha: Nocturnal GH secretion (patient-4) vs control Patient-4 Control
 vs control Patient-4 Control")
76
76 Thal: Nocturnal GH secretion (patient -5) vs control Patient 5 Control
 vs control Patient 5 Control")
77
77 Thal: Nocturnal GH secretion (patient-6) vs control Patient-6 Control
 vs control Patient-6 Control")
78
78 Thal: Nocturnal GH secretion (patient -7) vs control Patient-7 Control
 vs control Patient-7 Control")
79
79 Thal: Nocturnal GH secretion (patient -8) vs control Patient-8 Control
 vs control Patient-8 Control")
80
80 Thal: Nocturnal GH secretion (patient -9) vs control Patient-9 Control
 vs control Patient-9 Control")
81
81 Thal: Nocturnal GH secretion (patient-10) vs control Patient10 Control
 vs control Patient10 Control")
82
High incidence of GH Neuro-secretory Dysfunction (40% of short patients)
")
84
3. Do They Secrete Normal IGF-I ??

85
85 IGF-I in TM vs GHD vs CDGP

86
Low IGF-I High Prevalence (50-85%) with Defective GH secretion Soliman et al., 1999) (Shamshirsaz A A et al) 2003) Vannasaeng.S et al, 1980 Normal GH response Neurosecretory dysfunction Roth C et al., 1997 Soliman et al., 1999 Spoliotis BE; 1996 Pasqualetti et al 1992
 with Defective GH secretion Soliman et al., 1999) (Shamshirsaz A A et al) 2003) Vannasaeng.S et al, 1980 Normal GH response Neurosecretory dysfunction Roth C et al., 1997 Soliman et al., 1999 Spoliotis BE; 1996 Pasqualetti et al 1992")
87
What is the pattern of IGF-I throughout childhood ? The age-related levels in serum total IGF-I in thalassemic males were significantly decreased from early childhood to 18 years of age compared to normal subjects.

89
IGF-I Generation in GHD vs GHS Thalassemic males with GHD did not show any significant peak of IGF-I levels until 18 years of age. Thalassemic males with normal GH response to provocation (GHS) achieved a significant peak level of IGF-I that was attenuated and late compared to normal males.
 achieved a significant peak level of IGF-I that was attenuated and late compared to normal males..")
91
IGF-I Secretion The basal serum IGF-I concentrations at different ages did not differ between the GHD and GHS groups until the age of 12 years. After 12 years of age, IGF-I levels were significantly higher in thalassemic children with GHS.

92
Comparison between Growth and IGF-I secretion throughout childhood and puberty Soliman AT, PER, 2010 Anita Saxena, Int J Hum Genet, 3(4): 237-246 (2003)
: (2003)")
94
Short Patients with Thalassemia 4. Do They Generate Enough IGF- I in Response To GH ?? Partial GH Resistance ?

95
95 Thal: IGF-I generation

96
IGF-BP3 in Thalassemia

97
IGFBP3 after GH injection

98
98 GH/IGF-I/BP3 axis Children with thalassemia: 1.High incidence of GHD and GH- NSD 2.Low IGF-I 3.Lower IGFBP3 4.Decreased IGF-I synthesis after GH vs CDGD and GHD

100
Does correction of anemia increase secretion of IGF-I in T children with low IGF-I ? and /or Does it improve the response of IGF-I to exogenous stimulation by GH?

101
5. What is the effect of anemia on IGF-I Secretion ?

102
Correction of anemia significantly increased IGF-I Secretion

105
IGF-I levels increased significantly with correction of anemia. GH injections increased IGF-I significantly in TM. The peak IGF-I response to GH injections did not differ before vs after blood transfusion.

106
7. What is the Effect of Pubertal Delay /Failure on Growth and IGF-I ? 8. What is the effect of defective GH- IGF-I axis on puberty ?

107
Thalassaemic Boys Have high incidence pubertal delay/failure and short stature 1. Gonadotropin deficiency (pituitary) 2. Defective sex-steroid secretion (testes) have been described 3. Defective growth spurt
 2. Defective sex-steroid secretion (testes) have been described 3. Defective growth spurt.")
108
Deprivation of GH and IGF-I: 1) Delays the timely onset of puberty 2) Slows the pace of pubertal maturation (all species); 3) Attenuates phallic growth (human); 4) Reduces adult testicular size (rodent); but does not affect fertility in the mature individual (all species) Zachmann M, 1970. J Clin Endocrinol Metab 30:85–92 Young IR1989 J Endocrinol 121:563–570 Ernst M, 1991 Mol Endocrinol 5:1081–1089 Slootweg MC, 1997, J Endocrinol 155:159–164

110
PUBERTAL ASSESSMENT IN THALASSEMIA MAJOR

111
6-9-2012 Pubertal Surveys In BTM Country surveyHypogonadism Cyprus32% Greece42% Italy49% Egypt73% males, 42% females Qatar46% Romania77% males 41% females N. America35% TIF40.5% Pediatr Endocrinol Rev. 2007 Dec;5(2):642-8.,& Clin Endocrinol (Oxf). 1995 Jun;42(6):581-6. Acta Endocrinologica (Buc), vol. I, no. 2, p. 201-212, 2005
:642-8.,& Clin Endocrinol (Oxf) Jun;42(6): Acta Endocrinologica (Buc), vol. I, no. 2, p ,")
112
6/29/2016Ashraf T Soliman 6-9-2012 Thalassaemia (males) n = 45, all > 14 yr Age = 16.9 +/- 3.5 yr 73 % had test. vol < 3 ml 112

113
6/29/2016Ashraf T Soliman 6-9-2012 Testicular Volume 113

114
6/29/2016Ashraf T Soliman 6-9-2012 Age of Thelarche 114

115
6/29/2016Ashraf T Soliman 6-9-2012 Thal: Breast Development n = 49, All >14 y Age = 17.2 +/- 3.2 yr 42 % --No breast development 115

116
6/29/2016Ashraf T Soliman 6-9-2012 Age of Menarche (years) 116
 116")
117
6-9-2012 CONCLUSIONS Thalassaemia 40-70% of boys (>14 y) lack pubescent changes 40-60% of girls ( >14y) lack pubescent changes 117
 lack pubescent changes 40-60% of girls ( >14y) lack pubescent changes 117")
118
Hypogonadism Effect on Growth in TM Deprivation of sex-steroids at or after the time of expected puberty : o Loss or attenuation of pubertal growth spurt o predisposes to reduced peak bone mass (osteopenia, osteoporosis) Testosterone, GH, IGF-I concentrations correlate with bone mass in some analyses Ongphiphadhanakul B, Clin Endocrinol (Oxf) 1998; 49:803–809 van den Beld AW, J Clin Endocrinol Metab 2000; 85:3276–3282 Seeman E, Am J Physiol 1996; 270:E320–E327
 Testosterone, GH, IGF-I concentrations correlate with bone mass in some analyses Ongphiphadhanakul B, Clin Endocrinol (Oxf) 1998; 49:803–809 van den Beld AW, J Clin Endocrinol Metab 2000; 85:3276–3282 Seeman E, Am J Physiol 1996; 270:E320–E327")
119
Puberty : Thalassemic Patients 1. Delayed puberty 2. Hypo gonadotropic hypogonadism 3. Defective testosterone secretion 4. Defective spermatogenesis 5. Delayed onset of menstruation 6. Primary Amenorrhea 7. Secondary Amenorrhea

120
Basal Investigations 1. Low Sex steroid (testosterone- Estradiol) 2. low Gonadotropin (LH and FSH) (Hypogonadotrophic hypogonadism)
 (Hypogonadotrophic hypogonadism).")
126
Pubertal Induction And Growth

127
Testosterone replacement in HH males The anabolic effects of testosterone are associated with : 1) Increased pulsatile GH secretion 2) Increased IGF-I synthesis in liver and bone cells 3) Increased GI absorption and skeletal retention of calcium and magnesium 4) Increased mass, mechanical loading and energy expendature. Cicognani A, Acta Endocrinol (Copenh) 1989; 121:777–783 Hansen TB, J Clin Endocrinol Metab 1996; 81:3352–3359
 1989; 121:777–783 Hansen TB, J Clin Endocrinol Metab 1996; 81:3352–3359.")
130
WHAT IS THE EFFECT OF NUTRITION ON GROWTH AND IGF-I IN TM ?

131
Nutrition is an important factor in growth and development Protein/Calorie Defect due to hyper- catabolism (BM, Cardiac and Resp ) Zinc deficiency exists as a growth-limiting factor in thalassemia major : Short stature, low weight, anorexia, and hypogonadism found in the zinc deficiency, has been found in most of the patients (Arcasoy and Cavadar 1981; Arcasoy et al. 1983). Vitamin D Deficiency
. Vitamin D Deficiency.")
132
Wt, BMI and IGF-I Before vs after Nutritional Supplementation

133
Vitamin D Deficiency Vitamin D deficiency was detected in 50-100% of thalassemic adolescents. An IM injection of a mega dose of cholecalciferol is an effective therapy for treatment for 3 months. Correction of VDD --- Increased Linear Growth and IGF-I level Pediatric Endocrinology Reviews (PER), 6 Supp 1, 2008 NAPOLI N. Bone ISSN, 2006; 8756-328 Br J Haematol. 2008 Jun;141(6):891-4
, 6 Supp 1, 2008 NAPOLI N. Bone ISSN, 2006; Br J Haematol Jun;141(6):")
134
Zinc Deficiency and Treatment Biochemical evidence of Zn deficiency in 40% of Thalassemic patients Those who received Zn for 1-7 years had higher growth velocity and HTSDS. Arcasoy A et al. Am J Hematol 1987, 24:127

136
PATHOLOGY Pituitary Liver Pancreas

137
MRI studies in patients with defective GH secretion (n = 9) Evidence of iron deposition in the pituitary gland and midbrain (n = 7) Marked diminution of the pituitary size (n = 4) Thinning of the pituitary stalk (n = 3) with its posterior displacement (n = 2),
 Evidence of iron deposition in the pituitary gland and midbrain (n = 7) Marked diminution of the pituitary size (n = 4) Thinning of the pituitary stalk (n = 3) with its posterior displacement (n = 2),")
138
A T Soliman J Trop Pediatr. 1999 Dec;45(6):327-37. T1 T2
: T1 T2")
139
A T Soliman J Trop Pediatr. 1999 Dec;45(6):327-37.
:")
140
Pituitary Siderosis Pediatr Radiol. 2007 December; 37(12): 1191–1200. A 12-year-old β-thalassaemia major. Midsagittal T1-weighted (TR/TE 500/20 ms) scan shows low-signal intensity of the anterior pituitary lobe (arrow) and the bone marrow (asterisks) suggesting iron overload. The pituitary gland is small measuring 3.5 mm. This patient developed hypogonadotropic hypogonadism. b An 11-year-old male with β-thalassaemia major. Mid-sagittal T1-weighted (TR/TE 500/20 ms) shows normal signal intensity of the anterior pituitary lobe (arrow) along with normal pituitary gland height (6 mm). The bone marrow (asterisk) shows low-signal intensity suggesting iron overload b An 11-year-old male with β-thalassaemia major. Mid-sagittal T1-weighted (TR/TE 500/20 ms) shows normal signal intensity of the anterior pituitary lobe (arrow) along with normal pituitary gland height (6 mm). The bone marrow (asterisk) shows low-signal intensity suggesting iron overload Control patient
 scan shows low-signal intensity of the anterior pituitary lobe (arrow) and the bone marrow (asterisks) suggesting iron overload. The pituitary gland is small measuring 3.5 mm. This patient developed hypogonadotropic hypogonadism. b An 11-year-old male with β-thalassaemia major. Mid-sagittal T1-weighted (TR/TE 500/20 ms) shows normal signal intensity of the anterior pituitary lobe (arrow) along with normal pituitary gland height (6 mm). The bone marrow (asterisk) shows low-signal intensity suggesting iron overload b An 11-year-old male with β-thalassaemia major. Mid-sagittal T1-weighted (TR/TE 500/20 ms) shows normal signal intensity of the anterior pituitary lobe (arrow) along with normal pituitary gland height (6 mm). The bone marrow (asterisk) shows low-signal intensity suggesting iron overload Control patient.")
141
Siderosis of Liver and Pancreas Pediatr Radiol. 2007 December; 37(12): 1191–1200 A 17-year-old male with β-thalassaemia major. Axial scan, fourth echo of a multiecho spin-echo sequence (TR/TE: 2000/20, 40, 60, 80, 100, 120, 140, 160 ms), shows low-signal intensity in the liver, bone marrow of the spinal body and the pancreas suggesting iron overload.
: 1191–1200 A 17-year-old male with β-thalassaemia major. Axial scan, fourth echo of a multiecho spin-echo sequence (TR/TE: 2000/20, 40, 60, 80, 100, 120, 140, 160 ms), shows low-signal intensity in the liver, bone marrow of the spinal body and the pancreas suggesting iron overload..")
142
The photomicrograph (iron stain; magnification, 500) of undecalcified bone section illustrates the thick linear deposition of iron (blue line) along the mineralization front (thick arrows). The unmineralized zone is also stained blue, but with lighter intensity (areas between thin arrows). Active osteoblasts (arrowheads) are also present along the osteoid surface.
. Active osteoblasts (arrowheads) are also present along the osteoid surface..")
143
Iron deposition in Kupffer cells and spilling into parenchymal cells in late stages of hemosiderosis

145
What is the Effect of GH therapy on Growth and IGF-I in TM ??

146
146 Thal: Growth on GH therapy

147
147 Thal: IGF-I & GV after GH therapy

148
Short term (one year) GH Therapy Studies Demonstrated that treatment for one year resulted in significant increase in the growth velocity without increase in rate of skeletal maturation. The growth rate on GH therapy was significantly slower in TM and their IGF-I were lower vs non- thalassemic children with GHD or ISS on same GH doses.

149
Short term (> 2 years) GH Therapy Studies A positive growth response to GH was demonstrated in the second year of treatment in the report by ( Wu et al ) And for 3 to 4 years with improvement in the height SDS for both bone age and chronological age in other studies (Kwan EYW, J Pediatr Endocrinol Metab 2000; 13 : 545-552
 GH Therapy Studies A positive growth response to GH was demonstrated in the second year of treatment in the report by ( Wu et al ) And for 3 to 4 years with improvement in the height SDS for both bone age and chronological age in other studies (Kwan EYW, J Pediatr Endocrinol Metab 2000; 13 :")
150
(Final adult height) after GH Therapy for 2-9 years (n =13) Before Treatment Final adult Ht Boys-3.7-1.75 Girls-2.8-1.58 Theodoridis et al. J Pediatr Endocrinol Metab 1998; 11 (Suppl 3) : 835-844. HtSDS Before Treatment Final Adult Height SDS Improvement compared to mid-parental Ht N= 10 Started -age 11 y -2.63-0.61.6 Low LC, Ind J Ped 2005, 159, 64
 : HtSDS Before Treatment Final Adult Height SDS Improvement compared to mid-parental Ht N= 10 Started -age 11 y Low LC, Ind J Ped 2005, 159, 64.")
152
What is the effect of Bone Marrow Transplantation on Growth ?

153
BMD after bone marrow transplantation in TM (n = 32) F/U > 2 yr The HtSDS increased by 0.6 SD ( from -1.6 to 1) 5 years after BMT. Before BMT 40% had HtSDS < -2 40 % were < -2 5 Years after BMT only 15% had HtSDS < -2. Pediatr Hematol Oncol. ;21 (5):411-9
:")
154
TM – Effect of bone marrow transplantation (BMT) ( n= 47) A strict correlation between age at time of transplant and final adult height. T M who were 7 years. The greatest loss in height was observed with High Ferritin and ALT. Subjects who received BMT before 7 years had normal adult Ht in relation to the genetic target height. Subjects who received BMT after 7 years of age, failed to achieve their full genetic potential. A close effect of the age at time of transplant on subsequent growth rate. Bone Marrow Transplantation (2001) 28, 201-205.
 28,")
155
GH therapy (2y): effect On TM patients after BMT (IGF-I secretion & growth) Responders Increased GV Increased IGF-I secetion Decreased Ferritin Decreased ALT and AST Non-responders Decreased GV No change in IGF-I Increased Ferritin Higher ALT and AST There was a significant correlation between IGF-I, ALT, AST & ferritin in all patients before and after therapy. Bone Marrow Transplant. 1997 Oct;20(7):567-73.
:")
157
Thalassaemia (Summary) Slow linear growth (HtSDS, GV) High prevalence of impaired spontaneous and provoked GH secretion Low IGF-I and BP3 secretion Low of IGF-I after GH injection and therapy. GV improved on GH therapy but < those for ISS and GHD Partial improvement of final adult ht with GH therapy.

160
RECOMMENDATIONS

161
161 Increasing IGF-I : Proper transfusion and Chelation Improving nutritional status ( Protein-Calorie, Vitamin D, Zn, Carnitine) Correcting GHD (GH / IGF-I therapy) Inducing puberty at proper time, Prevention of hepatitis Bone marrow transplantation (before 7 y) All can improve growth and BMD
 Correcting GHD (GH / IGF-I therapy) Inducing puberty at proper time, Prevention of hepatitis Bone marrow transplantation (before 7 y) All can improve growth and BMD")
162
IGF-I Therapy TM patients with and without GHD have low IGF-I secretion. Their Growth and IGF-I response to GH is suboptimal (GH resistance) They need bigger GH doses for accelerating growth. Final adult height after GH treatment is still short IGF-I has growth promoting as well as insulin-like activities while GH is lipolytic. IGF-I therapy with or without GH is on small trials now ????
 They need bigger GH doses for accelerating growth. Final adult height after GH treatment is still short IGF-I has growth promoting as well as insulin-like activities while GH is lipolytic. IGF-I therapy with or without GH is on small trials now .")
163
Algorithm 1.If the patient is GH deficient ---Start GH therapy early 2.If he responds to normal dose (0.02-0.03 mg/kg/day) with proper increase of IGF-I--- continue 3.If GV is slow and/or IGF-I low - Increase GH dose 4.At or after (13 (F) and 14 (M) years slowly induce puberty simulating the normal physiology 5.At all stages supplement nutrition +/- Zinc +/- vit D therapy to increase IGF-I --- growth. 6.Correct any Thyroid hormone deficiency

164
Puberty Guidelines (6-months Intervals) Tanner staging should be recorded every six months. Girls without evidence of an advancing pubertal stage by 12-13 years and boys by 14 years require screening with LH/ FSH, and se steroid. If LH and FSH levels are low for the patient’s age, suspect hypogonadism. GnRH stimulation may help to dx HH. (This should to be done prior to a blood transfusion on a different day than the oral glucose tolerance test.)
.")
165
BTM: Male Hypogonadism Testosterone level should be checked annually in boys, starting in the early adolescent years (at approximately 13 years old). If testosterone level is low--- endocrine consultation --- start monthly Testosterone vs HCG treatment. The starting dose is usually 50 mg, given monthly as an intramuscular shot. The dose needs to be adjusted periodically for the patient’s age and pubertal status, as well as for a sexually active man.

166
BTM: Female Hypogonadism Estrogen replacement is recommended for amenorrheic adolescent girls and adult women: 2.5-5ug Ethinyl Estradiol with increasing doses q 6mon Afterward, an oral contraceptive pill may replace Premarin. A gynecological consultation and fertility evaluation is recommended for women on estrogen therapy.

167
adults Recommendation for GH testing in adults with BTM Short stature (Height SDS <−2.5), Severe and/or prolonged iron overload, Severe osteoporosis and/or serum IGF-I level <−2 SD Patients with childhood-onset GHD, in the presence of pituitary iron deposition and/or atrophy are highly suggestive of GHD. In adult TM patients, with normal liver function, an IGF-I level <50th percentile should be taken in consideration as a cut-off level for the GH assessment. De Sanctis V et al. IJEM, 2014

168
Thank You

Similar presentations