Download presentation
Presentation is loading. Please wait.

2
Dr.H-Kayalha Anesthesiologist

4
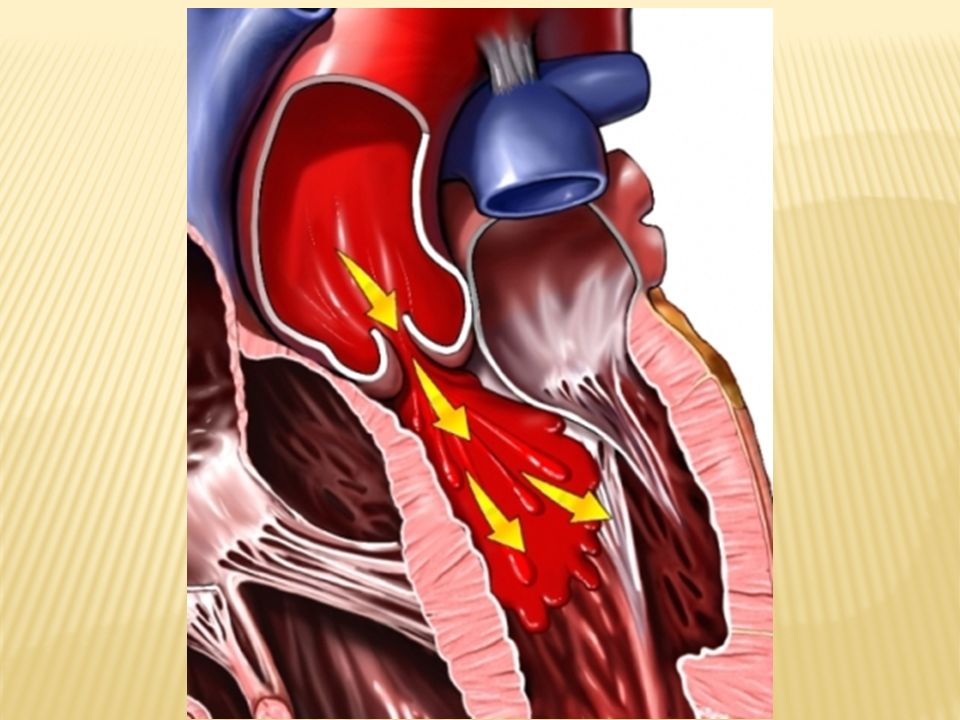
Aortic regurgitation results from failure of aortic leaflet coaptation caused by disease of the aortic leaflets or of the aortic root.

6
Common causes of leaflet abnormalities include: 1-infective endocarditis 2-rheumatic fever 3-bicuspid aortic valve 4-use of anorexigenic drugs.

7
Abnormalities of the aortic root causing aortic regurgitation include : 1-idiopathic aortic root dilation 2-hypertension-induced aortoannular ectasia 3-aortic dissection 4-syphilitic aortitis 5-Marfan syndrome 6-Ehlers-Danlos syndrome 7-rheumatoid arthritis 8- ankylosing spondylitis 9- psoriatic arthritis.

8
Acute aortic regurgitation is :usually the result of endocarditis or aortic dissection.

10
The basic hemodynamic derangement in aortic regurgitation is a decrease in cardiac output because of regurgitation of a part of the ejected stroke volume from the aorta back into the left ventricle during diastole.

11
This results in a combined pressure and volume overload on the left ventricle.

12
The magnitude of the regurgitant volume depends on : (1) the time available for the regurgitant flow to occur, which is determined by the heart rate (2) the pressure gradient across the aortic valve, which is dependent on the systemic vascular resistance.
 the time available for the regurgitant flow to occur, which is determined by the heart rate (2) the pressure gradient across the aortic valve, which is dependent on the systemic vascular resistance.")
13
The magnitude of aortic regurgitation is decreased by tachycardia and peripheral vasodilation.

14
The left ventricle compensates by developing hypertrophy and enlarging to accommodate the volume overload. Because of the increased oxygen requirements necessitated by left ventricular hypertrophy and the decrease in aortic diastolic pressure, which decreases coronary blood flow, angina pectoris may occur in the absence of coronary artery disease.

15
The left ventricle can usually tolerate the chronic volume overload. However, if left ventricular failure occurs, left ventricular end-diastolic volume increases dramatically and pulmonary edema develops.

16
A helpful indicator of left ventricular function in the presence of aortic regurgitation is the echocardiographic determination of end- systolic volume and ejection fraction, both of which remain normal until left ventricular function becomes impaired.

17
Indeed, surgery is recommended before : 1-the ejection fraction decreases to less than 55% 2- left ventricular end-systolic volume increases to more than 55 mL.

18
Compared to patients with chronic aortic regurgitation, patients with acute aortic regurgitation experience severe volume overload in a ventricle that has had no time to compensate. This typically results in coronary ischemia, rapid deterioration in left ventricular function, and heart failure.

20
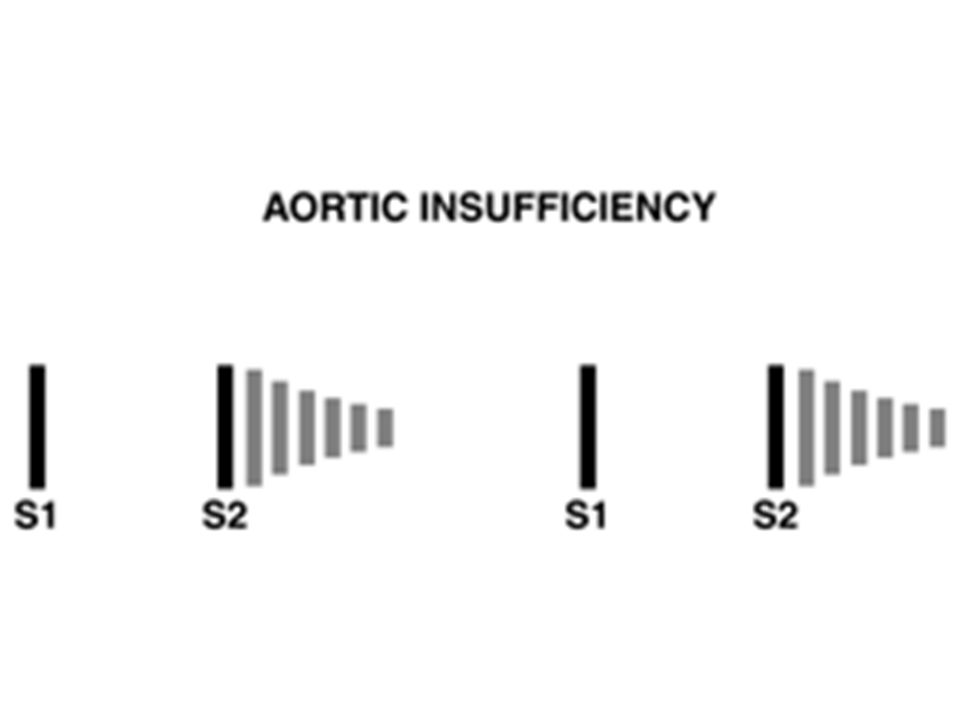
Aortic regurgitation is recognized clinically by its characteristic diastolic murmur heard best along the left sternal border and peripheral signs of a hyperdynamic circulation including a widened pulse pressure, decreased diastolic blood pressure, and bounding pulses.

22
In addition to the typical murmur of aortic regurgitation, there may be a low-pitched diastolic rumble (Austin-Flint murmur) that results from the regurgitant jet causing fluttering of the mitral valve.
 that results from the regurgitant jet causing fluttering of the mitral valve.")
23
symptoms of aortic regurgitation may not appear until left ventricular dysfunction is present. Symptoms at this stage are manifestations of left ventricular failure (dyspnea, orthopnea, fatigue) and coronary ischemia.
 and coronary ischemia..")
24
With chronic aortic regurgitation, evidence of left ventricular enlargement and left ventricular hypertrophy may be seen on the chest radiograph and ECG.

25
Echocardiography will identify any anatomic abnormalities of the aortic valve including leaflet perforation or prolapse and will identify any abnormalities in the aortic root and aortic annulus. Left ventricle size, volume, and ejection fraction can be measured, and Doppler examination can be used to identify the presence and severity of aortic regurgitation.

26
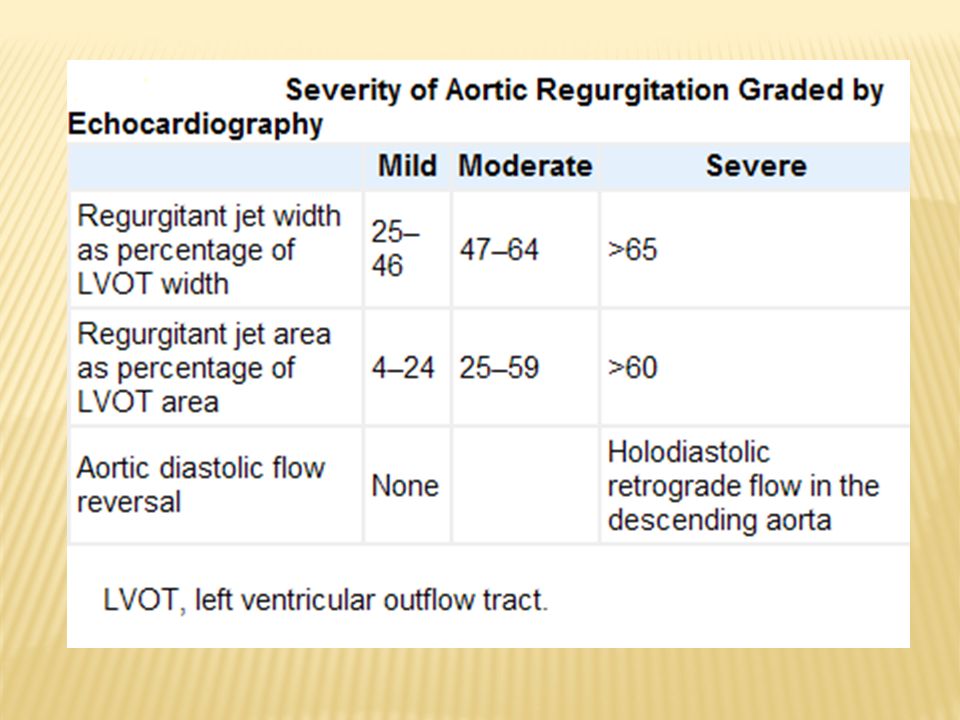
Many methods exist to quantify aortic regurgitation.These include regurgitant jet width as a percentage of overall left ventricular outflow tract width, pressure half-time, and.diastolic flow reversal in the descending aorta ( Table in next slide ) Cardiac catheterization and cardiac magnetic resonance imaging may be useful for grading aortic regurgitation if echocardiography is insufficient.
 Cardiac catheterization and cardiac magnetic resonance imaging may be useful for grading aortic regurgitation if echocardiography is insufficient.")
28
Surgical replacement of a diseased aortic valve is recommended before the onset of permanent left ventricular dysfunction, even if patients are asymptomatic.

29
The operative mortality for isolated aortic valve replacement is approximately 4%. It is higher if there is concomitant aortic root replacement or coronary artery bypass grafting or if there are substantial comorbidities. The mortality rate of asymptomatic patients with normal left ventricular size and function is less than 0.2% per year.

30
In contrast, symptomatic patients have a mortality rate greater than 10% per year. In acute aortic regurgitation, immediate surgical intervention is necessary because the acute volume overload results in heart failure. Alternatives to aortic valve replacement with a prosthetic valve include a pulmonic valve autograft (Ross procedure) and aortic valve reconstruction.
 and aortic valve reconstruction..")
31
Medical therapy of aortic regurgitation is designed to decrease systolic hypertension and ventricular wall stress and improve left ventricular function.

32
Intravenous infusion of a vasodilator such as nitroprusside and an inotropic drug such as dobutamine may be useful for improving forward left ventricular stroke volume and reducing regurgitant volume. Long-term therapy with nifedipine or hydralazine can be beneficial and may delay the need for surgery in asymptomatic patients with good left ventricular function.

33
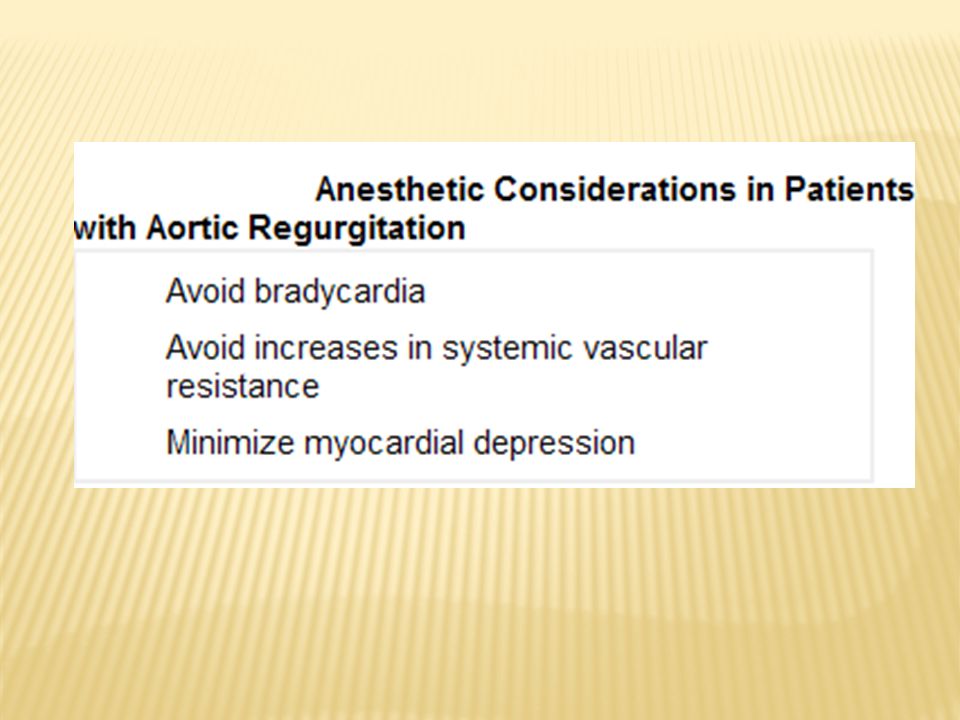
Management of anesthesia for noncardiac surgery in patients with aortic regurgitation is designed to maintain the forward left ventricular stroke volume. The heart rate must be kept at more than 80 bpm because bradycardia, by increasing the duration of diastole and thereby the degree of regurgitation, produces acute left ventricular volume overload. An abrupt increase in systemic vascular resistance can also precipitate left ventricular failure.

34
The compensations for aortic regurgitation may be tenuous, and anesthetic-induced myocardial depression may upset this delicate balance. If left ventricular failure occurs, it is treated with a vasodilator for afterload reduction and an inotrope to increase contractility. Overall, modest increases in heart rate and modest decreases in systemic vascular resistance are reasonable hemodynamic goals during anesthesia. General anesthesia is the usual choice for patients with aortic regurgitation.

36
Induction of anesthesia in the presence of aortic regurgitation can be achieved with inhalation anesthesia an intravenous induction drug. The ideal induction drug should not decrease the heart rate or increase systemic vascular resistance.

37
In the absence of severe left ventricular dysfunction, maintenance of anesthesia is often provided with nitrous oxide plus a volatile anesthetic and/or opioid. The increase in heart rate, decrease in systemic vascular resistance, and minimal myocardial depression of isoflurane, desflurane, and sevoflurane make these drugs excellent choices in patients with aortic regurgitation.

38
In patients with severe left ventricular dysfunction, high-dose opioid anesthesia may be preferred. Bradycardia and myocardial depression from concomitant use of nitrous oxide or a benzodiazepine are risks of the high- dose narcotic technique. Neuromuscular blockers with minimal or no effect on blood pressure and heart rate are typically used, although the modest increase in heart rate associated with pancuronium administration could be helpful in patients with aortic regurgitation.

39
Mechanical ventilation should be adjusted to maintain normal oxygenation and carbon dioxide elimination and adequate time for venous return. Intravascular fluid volume should be maintained at normal levels to provide for adequate cardiac preload. Bradycardia and junctional rhythm may require prompt treatment with intravenous atropine.

40
Minor surgery in patients with asymptomatic aortic regurgitation does not require invasive monitoring. Standard monitors should be adequate to detect any rhythm disturbances or myocardial ischemia. In the presence of severe aortic regurgitation, monitoring with a pulmonary artery catheter or transesophageal echocardiography is helpful for detection of myocardial depression, for facilitating intravascular volume replacement, and for measuring the response to administration of a vasodilating drug.

41
Have a good day

Similar presentations












 CPP = aortic diastolic.>")






