Download presentation
Presentation is loading. Please wait.

1
Endocrine System Diabetes, Thyroid, Parathyroid NUR 171

2
Normal Insulin function

3
Altered Mechanisms in Type 1 and Type 2 Diabetes Fig. 49-2

5
http://coursewareobjects.elsevier.com/objects/pa geburst/index.php?path=rtmp://media.us.elsevierh ealth.com/archieAnimations/836.flv http://coursewareobjects.elsevier.com/objects/pa geburst/index.php?path=rtmp://media.us.elsevierh ealth.com/archieAnimations/836.flv

6
Comparison DM1DM2 Acute S/S onset 3 P’s polydypsia, polyuria, polyphagia Weight loss Weakness Fatigue DKA S/S non specific Fatigue Recurrent infections Prolonged wound healing Visual changes

7
Collaborative assessment Glycosylated Hemoglobin (Hgb A1C ) Fasting Plasma Glucose (FPG) Oral Glucose Tolerance Test (OGTT) Random Blood Glucose (RBG)
 Fasting Plasma Glucose (FPG) Oral Glucose Tolerance Test (OGTT) Random Blood Glucose (RBG)")
8
Collaborative assessment Blood Studies Reference interval: 70-99 mg/dL (3.9-5.5 mmol/L) Reference interval: <100 mg/dL (5.5 mmol/L) baseline, <200 mg/dL (11.1 mmol/L) at 30 and 60 min, <140 mg/dL (7.8 mmol/L) at 120 min. Reference interval: 4.0%-6.0% Fasting blood glucose (FBG) Oral glucose tolerance test (OGTT) Glycosylated hemoglobin (Hb A1C)
 Oral glucose tolerance test (OGTT) Glycosylated hemoglobin (Hb A1C).")
9
Nursing Assessment

10
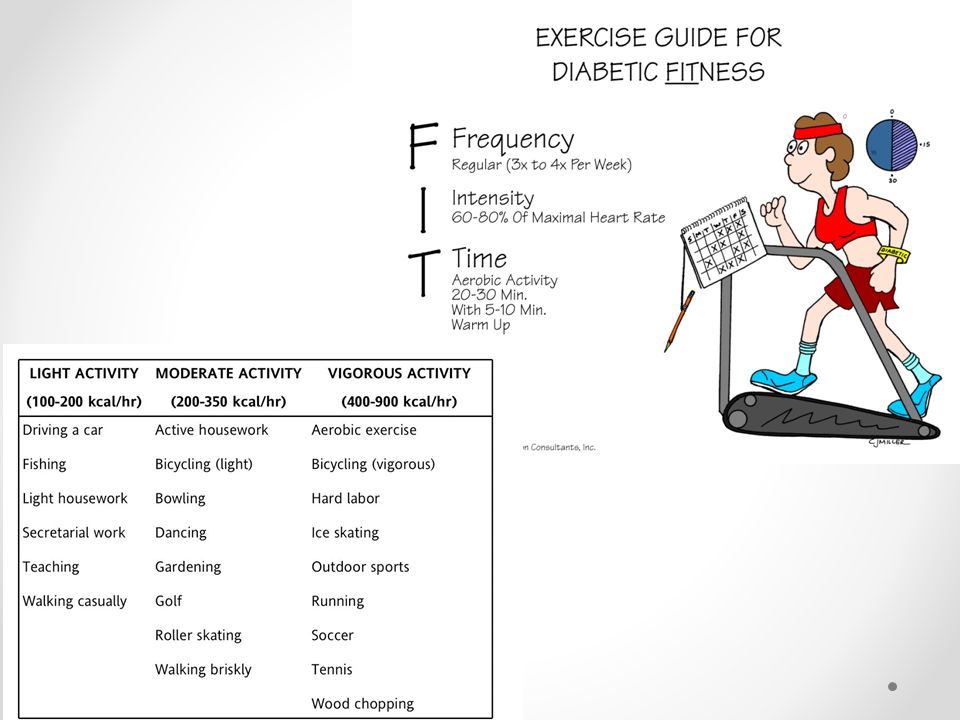
Collaborative Care Patient and caregiver teaching and follow-up programs Nutritional therapy (see Table 49-9) Exercise therapy (see Tables 49-10 and 49-11) Self-monitoring of blood glucose (SMBG) Oral and other agents (see Table 49-7) Enteric-coated aspirin (81-162 mg/day) Angiotensin-converting enzyme (ACE) inhibitors (see Table 33-8) Angiotensin II receptor blockers (ARBs) (see Table 33-8) Antihyperlipidemic drugs (see Table 34-6)
 Exercise therapy (see Tables and 49-11) Self-monitoring of blood glucose (SMBG) Oral and other agents (see Table 49-7) Enteric-coated aspirin ( mg/day) Angiotensin-converting enzyme (ACE) inhibitors (see Table 33-8) Angiotensin II receptor blockers (ARBs) (see Table 33-8) Antihyperlipidemic drugs (see Table 34-6)")
11
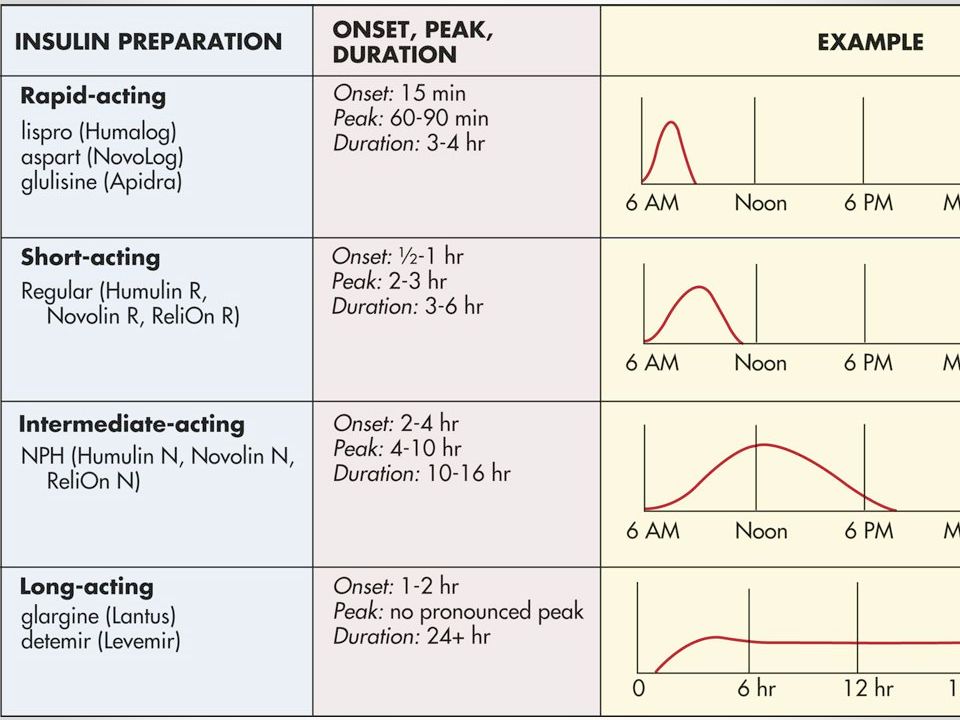
Insulin Rapid-acting synthetic insulin analogs, which include lispro (Humalog), aspart (NovoLog), and glulisine (Apidra Long Acting : Insulin glargine (Lantus) and detemir (Levemir) o Once daily: steady and continuous insulin release, o Do not have a peak of action (Detemir can be given twice daily.). o Glargine and detemir must not be diluted or mixed with any other insulin or solution. accuracy before use. Intermediate: NPH o basal insulin that has a duration of 10 to 16 hours.

13
Insulin devices

14
Oral Antidiabetics [OA] Sulfonylurea: Increase insulin production Meglitinides: rapid/short-lived insulin Biguanide: ↓ Rate of hepatic glucose production; augments glucose uptake by tissues, especially muscles α-Glucosidase Inhibitors: Delay absorption of glucose from GI tract Thiazolidinediones: ↑ Glucose uptake in muscle; ↓ endogenous glucose production Dipeptidyl Peptidase-4 (DPP-4) Inhibitors : Enhances the incretin system, stimulates release of insulin from pancreatic β cells, and ↓ hepatic glucose production
![Oral Antidiabetics [OA] Sulfonylurea: Increase insulin production Meglitinides: rapid/short-lived insulin Biguanide: ↓ Rate of hepatic glucose production; augments glucose uptake by tissues, especially muscles α-Glucosidase Inhibitors: Delay absorption of glucose from GI tract Thiazolidinediones: ↑ Glucose uptake in muscle; ↓ endogenous glucose production Dipeptidyl Peptidase-4 (DPP-4) Inhibitors : Enhances the incretin system, stimulates release of insulin from pancreatic β cells, and ↓ hepatic glucose production](http://images.slideplayer.com/38/10803960/slides/slide_14.jpg "Oral Antidiabetics [OA] Sulfonylurea: Increase insulin production Meglitinides: rapid/short-lived insulin Biguanide: ↓ Rate of hepatic glucose production; augments glucose uptake by tissues, especially muscles α-Glucosidase Inhibitors: Delay absorption of glucose from GI tract Thiazolidinediones: ↑ Glucose uptake in muscle; ↓ endogenous glucose production Dipeptidyl Peptidase-4 (DPP-4) Inhibitors : Enhances the incretin system, stimulates release of insulin from pancreatic β cells, and ↓ hepatic glucose production")
15
Newer Antidiabetic agents Dipeptidyl Peptidase-4 (DPP-4) Inhibitors Incretin Mimetics: Amylin Analog
 Inhibitors Incretin Mimetics: Amylin Analog")
16
Pancreas Transplantation Can be used as a treatment option for patients with type 1 diabetes mellitus. Can improve the quality of life by o eliminating the need for exogenous insulin, f o requent blood glucose measurements, o and many of the dietary restrictions imposed by the disorder.

17
Nutritional Therapy Greatest impact when provided at the onset of the diagnosis of the disease Eat a varied diet according to the current Food Pyramid Maintain exercise habits that will lead to improved metabolic control TABLE 49-9 NUTRITIONAL THERAPY o Recommendations for Patients with Diabetes Mellitus (Lewis 1231) Carbs: 130g/day Protein: 15-20% total calories Fat: <7% total calories Cholesterol <200mg/day Alcohol: < 1/day women, < 2/day men
 Carbs: 130g/day Protein: 15-20% total calories Fat: <7% total calories Cholesterol <200mg/day Alcohol: < 1/day women, < 2/day men")
18
Plate Method verses Food Pyramid

20
Diabetes Mellitus NANDA’s o Ineffective self-health management o Imbalanced nutrition: more than body requirements o Risk for injury o Risk for peripheral neurovascular dysfunction Interventions/Meds/Complications

22
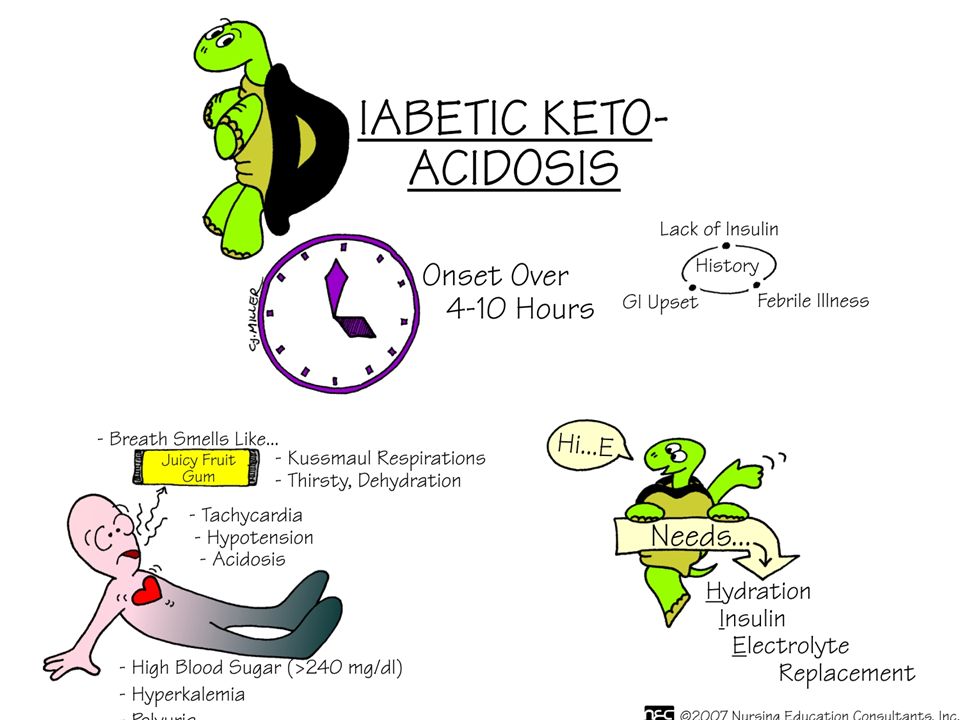
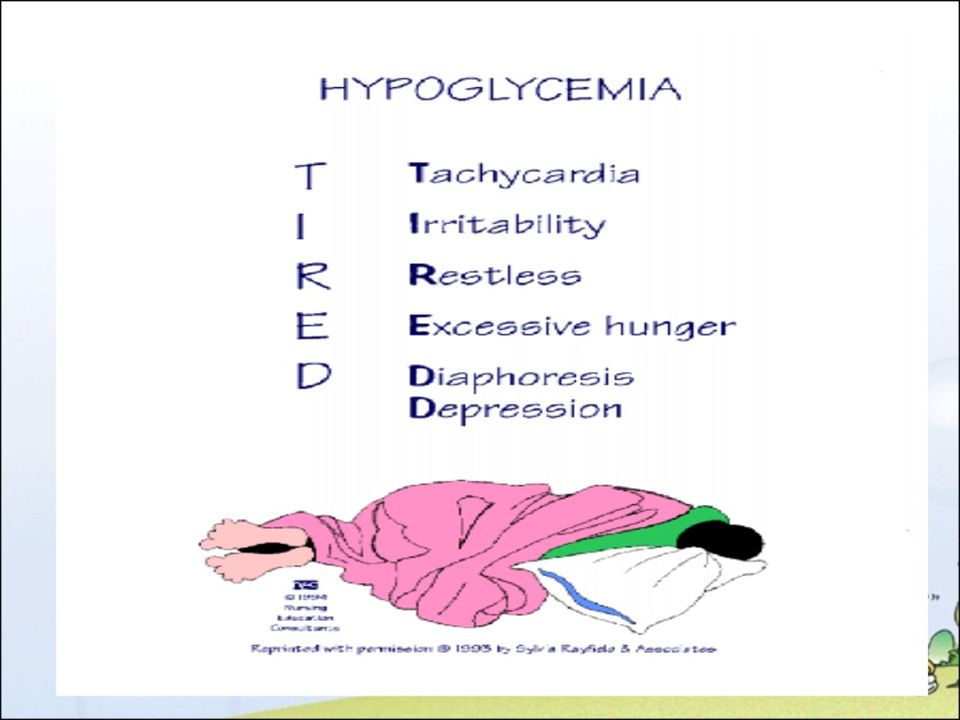
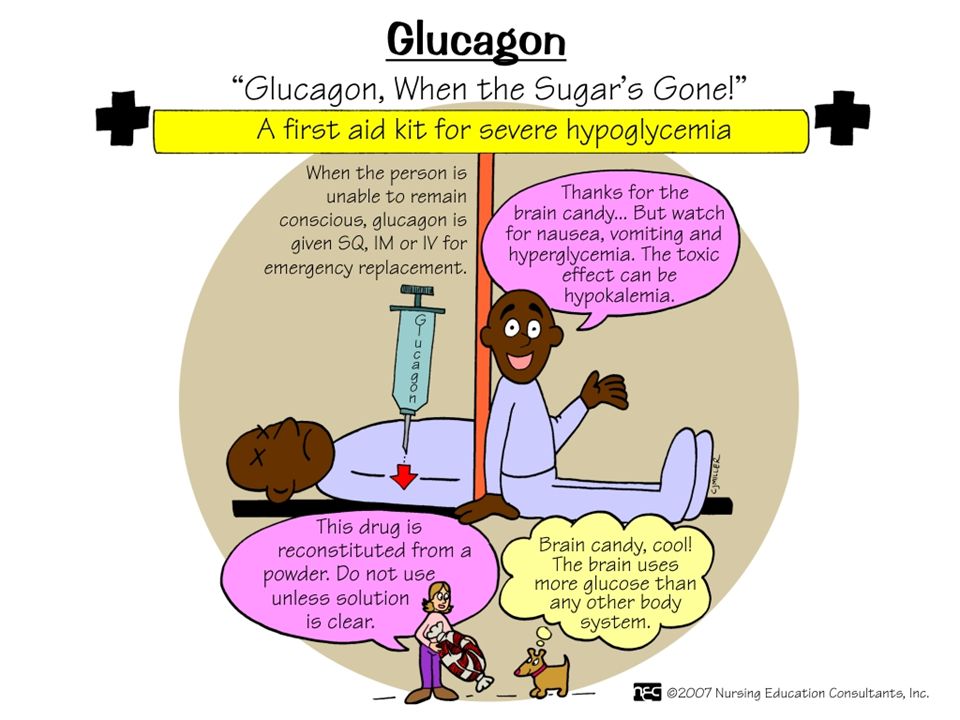
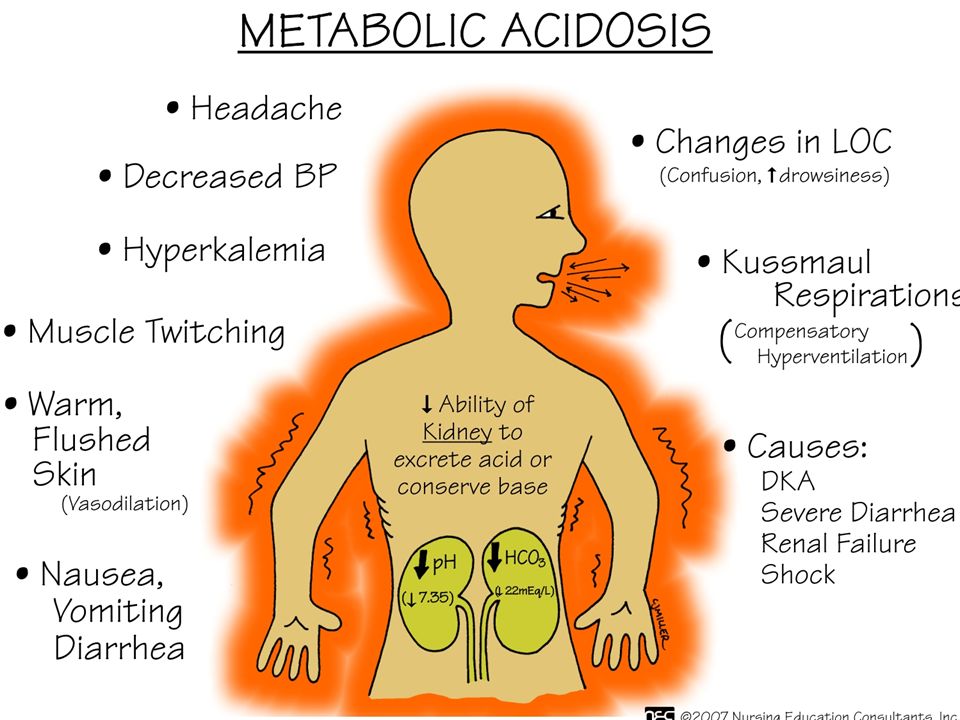
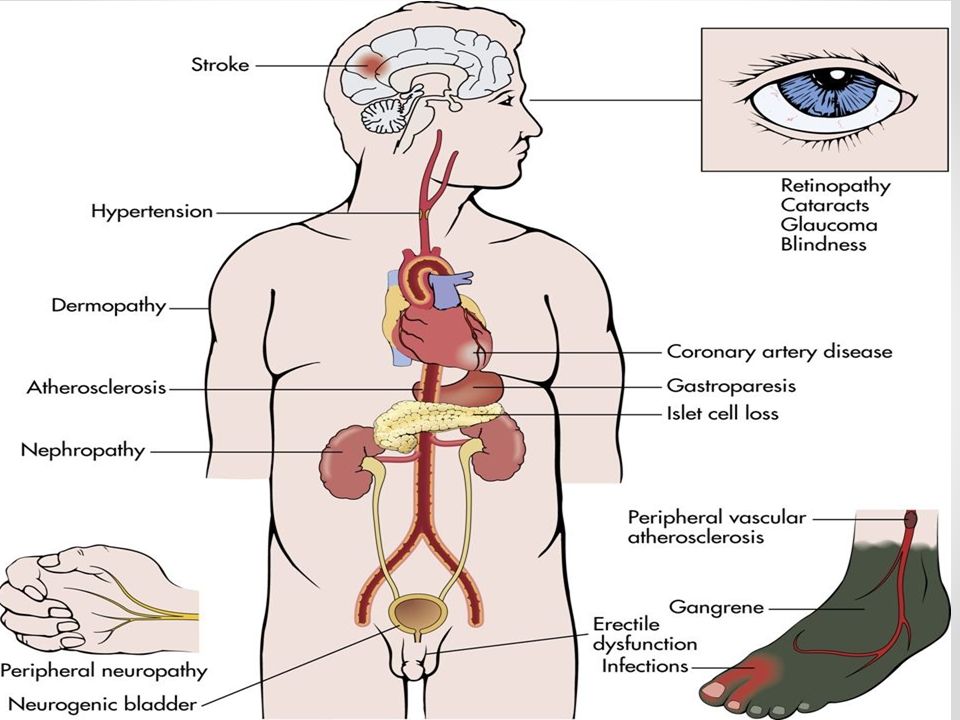
Complications Hyperglycemia o DKA Hypoglycemia Macrovascular o CAD, o CVA o PVD Microvascular o Nephropathy o Neuropathy o Retinopathy

23
Agents that potentiate hyper and hypoglycemia Hyperglycemic potentiators 1.Glucocorticoids 2.Estrogens 3.Diuretics 4.Dilantin 5.B blockers Hypoglycemic potentiators 1.ETOH 2.Salicylates 3. MAO inhibitors Mask s/s of hypoglycemia 1.B blockers

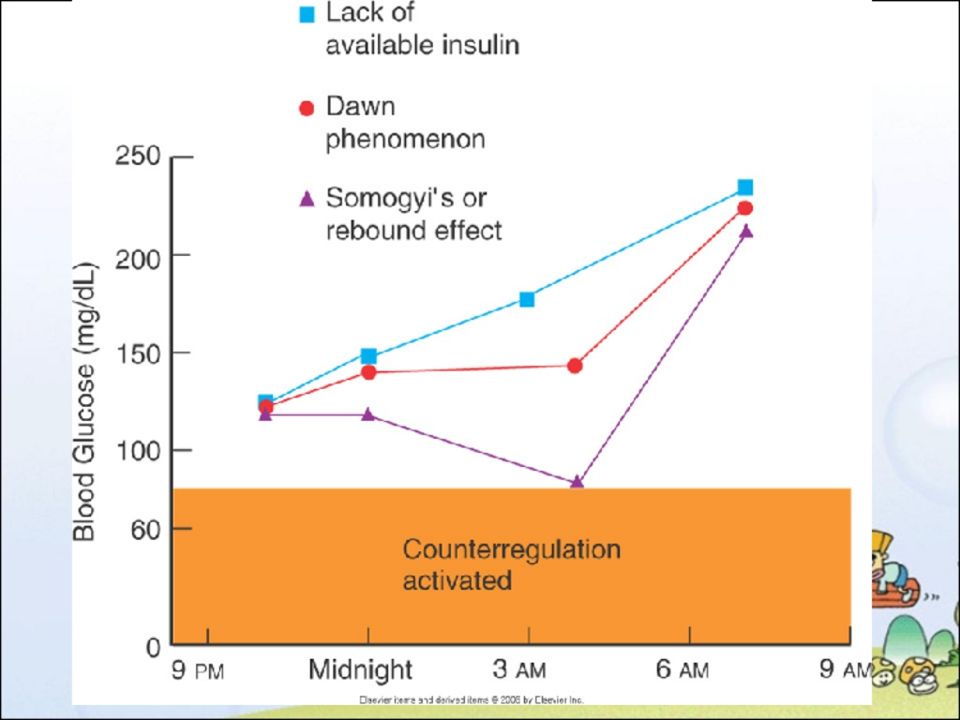
24
Hyperglycemia SomogyiDawn Phenomena Low BS during sleep Counter regulatory effect causes high BS on awakening Check BS 0200-0400 Decrease morning insulin dose Insulin dose decreased High BS on awakening Counter regulatory release in pre dawn hours More severe when growth hormone is at its peak during adolescence and young adulthood. Morning insulin increased

33
Diabetic Nephropathy Diabetic Nephropathy Microvascular complication Leading cause of end-stage renal disease (ESRD) in the United States Risk of nephropathy is about the same in patients with either type 1 or type 2 diabetes Annual Screening albumin-to-creatinine ratio in a random spot urine collection for albumin Serum creatinine Treatment: ACE or ARB
 in the United States Risk of nephropathy is about the same in patients with either type 1 or type 2 diabetes Annual Screening albumin-to-creatinine ratio in a random spot urine collection for albumin Serum creatinine Treatment: ACE or ARB")
34
Diabetic Neuropathy Sensory Neuropathy o Most common o Affects hands and feet bilaterally o “Stocking/glove” neuropathy o Key: Control glucose o RX: TCA [amitriptyline],SSRI [duloxetine], antisezure [gabapentin ] Autonomic Neuropathy o Affects all body systems o Delayed gastric emptying (gastroparesis) o Hypoglycemia d/t delayed gastric emptying o ED o Neurogenic bladder
![Diabetic Neuropathy Sensory Neuropathy o Most common o Affects hands and feet bilaterally o Stocking/glove neuropathy o Key: Control glucose o RX: TCA [amitriptyline],SSRI [duloxetine], antisezure [gabapentin ] Autonomic Neuropathy o Affects all body systems o Delayed gastric emptying (gastroparesis) o Hypoglycemia d/t delayed gastric emptying o ED o Neurogenic bladder](http://images.slideplayer.com/38/10803960/slides/slide_34.jpg "Diabetic Neuropathy Sensory Neuropathy o Most common o Affects hands and feet bilaterally o Stocking/glove neuropathy o Key: Control glucose o RX: TCA [amitriptyline],SSRI [duloxetine], antisezure [gabapentin ] Autonomic Neuropathy o Affects all body systems o Delayed gastric emptying (gastroparesis) o Hypoglycemia d/t delayed gastric emptying o ED o Neurogenic bladder")
35
Diabetic Retinopathy Non proliferative o Most common o Partial occlusion small BV of retina causing capillary microaneurysms Proliferative o Most severe o Affects retina and vitreous Collaborative Care o Annual dilated eye exams o DM 1 within 5 years of diagnosis

Similar presentations









 Diabetes Mellitus.>")







. Type 2 DM 90% of diabetics (in USA) Develops gradually may be without obvious symptoms may be detected by routine screening.>")

