Download presentation
Presentation is loading. Please wait.

1
Batch 17 2 March 2012 Dr S Gokul Shankar
Anaerobic Infections Batch 17 2 March 2012 Dr S Gokul Shankar

2
Lecture 26: Anaerobic Infections
OBJECTIVES: The objectives of this lecture are to describe the general properties of anaerobic bacteria describe the virulence factors and characteristic clinical features of infections caused by anaerobic bacteria discuss the classification of clostridium. discuss the clinical categorization of clostridium infections. discuss antibiotic induced diarrhoea and Clostridium difficile describe the laboratory identification of anaerobic bacteria, using clostridium infections as example.

3
Learning outcomes At the end of the lecture, students should be able to: describe the general properties of anaerobic bacteria describe the virulence factors and characteristic clinical features of infections caused by anaerobic bacteria describe the morphology of common Clostridium pathogens categorize clostridium infections clinically into the gas gangrene, tetanus, and food poisoning groups. describe the laboratory identification of anaerobic bacteria, using clostridium infections as example.

4
WHAT ARE ANAEROBIC BACTERIA?
Anaerobic bacteria are those that grow in the absence of oxygen, because they cannot tolerate the presence of oxygen

5
Anaerobic infections Common May be serious and life-threatening
Anaerobes are the predominant components of bacterial flora of normal human skin and mucous membranes Difficult to isolate from infectious sites and are often overlooked. Isolation requires appropriate methods of collection, transportation and cultivation of specimens Treatment is complicated by slow growth of these organisms, by the commonly polymicrobial nature of the infection and by the growing resistance of anaerobic bacteria to antimicrobial agents

6
Classification of anaerobes
OBLIGATE ANAEROBE - is any organism that does not require oxygen for growth and die in its presence AERO-TOLERANT ANAEROBES Can survive in presence of oxygen which cannot use oxygen for growth, but tolerate the presence of it FACULTATIVE ANAEROBES - which can grow without oxygen but can utilize oxygen if it is present.

7
Protections of bacteria against oxygen
Bacteria possess protective enzymes, catalase and superoxide dismutase. Catalase breaks down hydrogen peroxide into water and oxygen gas. Superoxide dismutase breaks superoxide down into peroxide and oxygen gas. Anaerobes missing one or both; slow or no growth in the presence of oxygen.

8
WHY ANAEROBIC BACTERIA ARE NOT ABLE TO TOLERATE OXYGEN?

9
Properties of Anaerobic bacteria
die in presence of oxygen due to the absence of the enzymes superoxide dismutase and catalase obligate anaerobes use alternate electron acceptors for cellular respiration such as sulfate, nitrate, iron, carbon monoxide, etc The energy yield of these respiratory processes is less than oxygen respiration. Can be spore forming/non spore forming .

12
Organism Site of infection Gram +ve cocci Peptostreptococcus spp. Respiratory tract, intra-abdominal & soft tissue infections Microaerophilic streptococci (not true anaerobes) Sinusitis, brain abscess Gram +ve non spore-forming bacilli Actinomyces spp. Intracranial abscess, chronic mastoiditis, aspiration pneumonia, head & neck infections Propionibacterium spp. Shunt infections, infections associated with foreign body Bifidobacterium spp. Chronic otitis media, cervical lymphadenitis, intra- abdominal infection Arachnia propionica Eubacterium lentum Gram +ve spore-forming organisms Clostridium perfringens Soft tissue infection, food poisoning Clostridium septicum Neutropaenic enterocolitis Clostridium ramosum Soft tissue infection Clostridium botulinum Botulism Clostridium tetani Tetanus Clostridium difficile Colitis, antibiotic-associated diarrhoea Gram –ve bacilli Bacteroides spp. Intra-abdominal infection, gynaecological infection, neonatal infection Prevotella spp Orofacial infection, aspiration pneumonia, periodontitis, intra-abdominal infection, gynaecological infection Fusobacterium spp. Aspiration pneumonia Porphyromonas spp.
 Sinusitis, brain abscess. Gram +ve non spore-forming bacilli. Actinomyces spp. Intracranial abscess, chronic mastoiditis, aspiration pneumonia, head & neck infections. Propionibacterium spp. Shunt infections, infections associated with foreign body. Bifidobacterium spp. Chronic otitis media, cervical lymphadenitis, intra- abdominal infection. Arachnia propionica. Eubacterium lentum. Gram +ve spore-forming organisms. Clostridium perfringens. Soft tissue infection, food poisoning. Clostridium septicum. Neutropaenic enterocolitis. Clostridium ramosum. Soft tissue infection. Clostridium botulinum. Botulism. Clostridium tetani. Tetanus. Clostridium difficile. Colitis, antibiotic-associated diarrhoea. Gram –ve bacilli. Bacteroides spp. Intra-abdominal infection, gynaecological infection, neonatal infection. Prevotella spp. Orofacial infection, aspiration pneumonia, periodontitis, intra-abdominal infection, gynaecological infection. Fusobacterium spp. Aspiration pneumonia. Porphyromonas spp.")
13
CLOSTRIDIA Gram positive spore forming bacilli ubiquitous
intestines of man and animals animal and human faeces, contaminated soil and water Several species associated with human disease

14
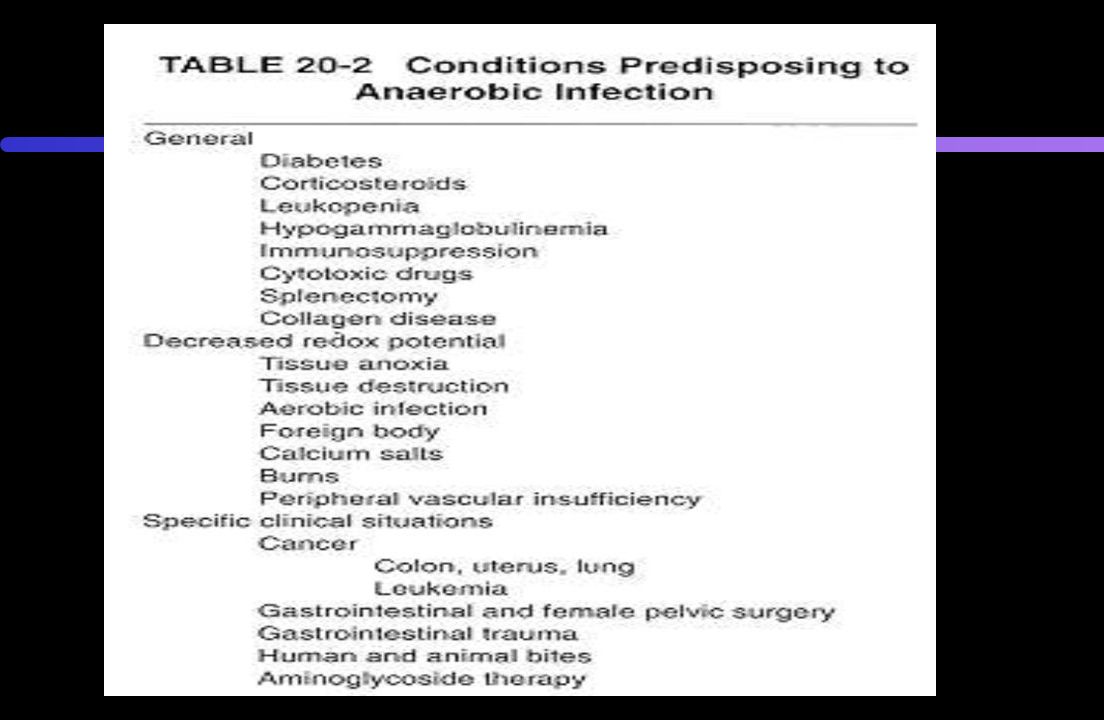
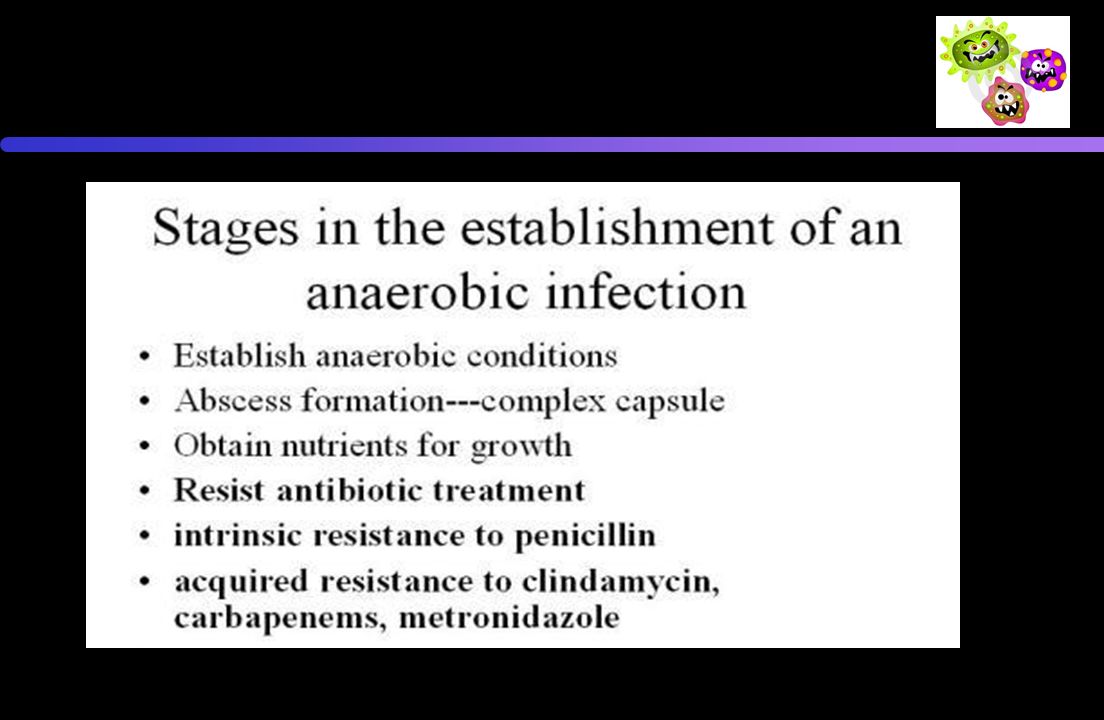
Pathogenesis of anaerobic infections
Contamination of site with spores Factors which promote anaerobiasis ‘crush’ injuries with interruption of blood supply, contaminaton with foreign bodies (dirt), tissue damage Germination of spores Toxin release Binding of toxin to receptor Resulting effect produces symptom(s) of disease
, tissue damage. Germination of spores. Toxin release. Binding of toxin to receptor. Resulting effect produces symptom(s) of disease.")
15
Clostridium perfringens
Morphology Large rectangular rod shaped Gram positive bacillus Spores seldom seen in vivo or in vitro non motile Pathogenesis Produces several toxins alpha (lecithinase), beta, epsilon enterotoxin Causes a spectrum of human diseases Bacteraemia Myonecrosis food poisoning enteritis necrotica (pig bel)
, beta, epsilon enterotoxin. Causes a spectrum of human diseases. Bacteraemia. Myonecrosis. food poisoning. enteritis necrotica (pig bel)")
16
Myonecrosis (Gas gangrene)
Clostridium perfringens is the most common bacterial agent, while C. novyi, C. septicum, and C. histolyticum cause most of the remaining cases Gangrene is necrosis and putrefaction of tissues. Gas production forms bubbles of gas in muscle (crepitus) and smell in decomposing tissue. After rapid and destructive local spread (which can take hours), systemic spread of bacteria and bacterial toxins may result in death. This is a problem in major trauma and in military contexts.
 and smell in decomposing tissue. After rapid and destructive local spread (which can take hours), systemic spread of bacteria and bacterial toxins may result in death. This is a problem in major trauma and in military contexts.")
17
The incubation period - short: almost always <3 days and frequently <24 h.
Typically, begins with the sudden onset of pain in the region of the wound wound must be deep, necrotic, and without communication to the surface. Soon after pain develops, local swelling and oedema—accompanied by a thin, often hemorrhagic exudate—appear. Patients frequently develop marked tachycardia, but elevation in temperature may be only minimal. Gas is usually not obvious/absent at this early stage Frothiness of the wound exudate may be noted. Profuse serous discharge

19
Diagnosis Myonecrosis (Gas gangrene) Food poisoning 3rd common
Gram stain of exudate - typical organisms no pus cells Culture -growth of C perfringens (and/or other clostridia associated with this clinical condition) Food poisoning 3rd common abdominal pain, diarrhoea and vomiting 8-18 hours after a suspect meal. Self limiting
 Food poisoning. 3rd common. abdominal pain, diarrhoea and vomiting 8-18 hours after a suspect meal. Self limiting.")
20
Enteritis necroticans (Clostridial necrotizing enteritis) -Pigbel
Rare, can be fatal severe abdominal pain, bloody diarrhoea (C perfringens type C) Caused by Beta toxin life-threatening sequence of severe abdominal pain, vomiting, bloody stool, ulceration of the small intestine with leakage (perforation) into the peritoneal cavity and possible death
 Caused by Beta toxin. life-threatening sequence of severe abdominal pain, vomiting, bloody stool, ulceration of the small intestine with leakage (perforation) into the peritoneal cavity and possible death.")
21
Treatment and prevention
Myonecrosis Proper wound debridement and ensure adequate blood supply Penicillin antitoxin and hyperbaric oxygen - no proven value Food poisoning Proper preparation and storage of food self limiting disease -antibiotics not indicated Pigbel Proper cooking of food immunization of susceptible population

22
Clostridium tetani Small motile spore forming Gram positive bacillus with round terminal spores (tennis racket appearance) Causes tetanus - a disease characterized by painful muscular spasms that can lead to respiratory failure and in up to 40% of cases, death. C. tetani produces two exotoxins tetanolysin tetanospasmin

23
leads to muscle contraction and spasm
) Pathogenesis: produces tetanospasmin during stationary phase which is released when cell lysis occurs binds to ganglioside on neuronal membranes toxin internalized and moves from peripheral to central nervous system crosses synapse and localized within vesicles acts by blocking release of neurotransmittors (eg GABA, Glycine leads to muscle contraction and spasm Characteristic features are a rigid smile, trismus (lock-jaw"), and opisthotonus (rigid, arched back)
 Pathogenesis: produces tetanospasmin during stationary phase which is released when cell lysis occurs. binds to ganglioside on neuronal membranes. toxin internalized and moves from peripheral to central nervous system. crosses synapse and localized within vesicles. acts by blocking release of neurotransmittors (eg GABA, Glycine. leads to muscle contraction and spasm. Characteristic features are a rigid smile, trismus (lock-jaw ), and opisthotonus (rigid, arched back)")
25
Prevention and treatment
DPT Vaccine (diphtheria-pertussis-tetanus) Active/passive immunization of ‘risk’ injuries management of wound tetanus toxoid Anti-tetanus serum (ARS -horse serum) or Human Tetanus ImmunoGlobulin (HTIG) Penicillin or Metronidazole Management of patient with tetanus respiratory and CVS support
 Active/passive immunization of ‘risk’ injuries. management of wound. tetanus toxoid. Anti-tetanus serum (ARS -horse serum) or Human Tetanus ImmunoGlobulin (HTIG) Penicillin or Metronidazole. Management of patient with tetanus. respiratory and CVS support.")
26
Clostridium difficile
Clostridia are motile bacteria that are ubiquitous in nature and are especially prevalent in soil. appear as long, irregularly (often "drumstick" or "spindle") shaped cells with a bulge at their terminal ends. Gram positive, spore forming
 shaped cells with a bulge at their terminal ends. Gram positive, spore forming.")
27
Clostridium difficile
Associated with human disease in mid-1970’s Found in human GIT in small numbers With antibiotic use, increase in number in GIT Clindamycin, ampicillin, cephalosporins proton pump inhibitors are a risk factor for C. difficile infection Produces 2 entero toxins Toxin A -enterotoxin & Toxin B –cytotoxin responsible for the diarrhoea and inflammation Diagnosis detection of toxins in stools /toxin genes by PCR culture of organism presence of C. Diff in the stool by C. Diff GDH antigen)
")
28
Antibiotic induced diarrhoea
Fluoroquinolones are more strongly associated with C difficile infections Other antibiotics including clindamycin, 3rd generation cephalosporins and beta-lactamase inhibitors Medication to suppress gastric acid production: H2 receptor antagonists and proton pump inhibitors - increased the risk Resistance development to ciprofloxacin and levofloxacin

29
Treatment - omit antibiotic if possible -
Clinical - Pseudomembranous colitis - the generalized inflammation of the colon and the development of pseudomembrane, a viscous collection of inflammatory cells, fibrin and necrotic cells. Treatment - omit antibiotic if possible - metronidazole or oral vancomycin

30
Clostridium botulinum
Fastidious spore forming anaerobic Gram positive bacillus Produces 8 antigenically distinct toxins Human disease described with types A, B, F & E Clinical Food borne botulism (weakness, dizziness, ocular palsy and progressive flaccid paralysis) infant botulism (floppy baby) wound botulism 75 ng of toxin can kill a healthy human being
 infant botulism (floppy baby) wound botulism. 75 ng of toxin can kill a healthy human being.")
31
Other anaerobic G-ve bacilli
Bacteroides, Prevotolla, Porphyromonas and Fusobacterium Present in GI tract -form large component of normal flora >80% of human infections associated with B fragilis virulence factors - capsule, LPS, agglutinins and enzymes Clinical - Endogenous infections Intra-abdominal pyogenic infections pleuro-pulmonary infections genital infection

32
Lab identification of C. botulinum
In laboratory isolated in tryptose sulfite cycloserine (TSC) growth media Always in an anaerobic environment with less than 2% of oxygen. Commercial kits that use a chemical reaction to replace O2 with CO2 (E.J. GasPak System). C. botulinum is lipase negative It grows pH values of 4.8 and 7 Cannot use lacose as a primary carbon.
 growth media. Always in an anaerobic environment with less than 2% of oxygen. Commercial kits that use a chemical reaction to replace O2 with CO2 (E.J. GasPak System). C. botulinum is lipase negative. It grows pH values of 4.8 and 7. Cannot use lacose as a primary carbon.")
33
Clostridium perfringens
Roberson’s cooked meet medium Clostridium perfringens from food/ wound

34
Colitis and C.difficile
Patients with C. difficile colitis often have elevated white blood cell counts Detect toxins produced by C. difficile in a sample of stool Flexible sigmoidoscopy and colonoscopy – look for pseudomembranes in the rectum and the sigmoid colon

Similar presentations







peritrichous.>")





 –Bacteria or their products may migrate to adjacent tissues or bloodstream.>")








