Download presentation
Presentation is loading. Please wait.

1
Principles of Mechanical Ventilation Mazen Kherallah, MD, FCCP

2
Oxygenation Parameters Alveolar P O2 Arterial P O2 Tension-based indices –P (A-a)o2 –P aO2 /P AO2 –P aO2 /F iO2 Respiratory index Pulmonary Shunt
o2 –P aO2 /P AO2 –P aO2 /F iO2 Respiratory index Pulmonary Shunt")
3
Distribution of Normal Ventilation-Perfusion Ratios 1 10 0.10

4
Oxygenation Status Monitoring Alveolar - arterial Oxygen Tension Difference P (A-a)o2 PAo2 = Fio2 (PB-P H2O ) - Pa co2 /R = (Fio2 713) - (Pa co2 /0.8) at sea level = 150 - (Pa co2 /0.8) at sea level on room air A-a Gradient = PAo2 - PaO2 Normal Value: 5-25 mmHg
o2 PAo2 = Fio2 (PB-P H2O ) - Pa co2 /R = (Fio2 713) - (Pa co2 /0.8) at sea level = (Pa co2 /0.8) at sea level on room air A-a Gradient = PAo2 - PaO2 Normal Value: 5-25 mmHg")
5
Oxygenation Status Monitoring A-a Gradient Increased: –Decreased Fio2 –V/Q mismatch –Shunting process –Diffusion abnormalities Decreased –Hyperventilation –Increased Fio2

6
Pa O2 /PA O2 Remains stable when FiO2 changes Can be used to determined FiO2 needed for desired PO2 –FiO2 needed=[(desired PaO2)/(PaO2/PAO2)+Paco2]/(PB-47) Value of less than 0.75 indicates pulmonary dysfunction due to V/Q abnormality, shunt or diffusion abnormality
![Pa O2 /PA O2 Remains stable when FiO2 changes Can be used to determined FiO2 needed for desired PO2 –FiO2 needed=[(desired PaO2)/(PaO2/PAO2)+Paco2]/(PB-47) Value of less than 0.75 indicates pulmonary dysfunction due to V/Q abnormality, shunt or diffusion abnormality](http://images.slideplayer.com/36/10666233/slides/slide_6.jpg "Pa O2 /PA O2 Remains stable when FiO2 changes Can be used to determined FiO2 needed for desired PO2 –FiO2 needed=[(desired PaO2)/(PaO2/PAO2)+Paco2]/(PB-47) Value of less than 0.75 indicates pulmonary dysfunction due to V/Q abnormality, shunt or diffusion abnormality")
7
Pa O2 /FI O2 Oxygenation index Value of less than 200 is associated with severe shunt in patients with acute respiratory failure Easy to calculate

8
Respiratory Index P(A-a) O2 /PaO2 Normal value 0.1 Values higher than 0.1 indicate respiratory abnormality Better indicator of oxygenation dysfuntion
 O2 /PaO2 Normal value 0.1 Values higher than 0.1 indicate respiratory abnormality Better indicator of oxygenation dysfuntion")
9
Pulmonary Shunt Q S /Q T = (CcO2-CaO2)/(CcO2-CvO2) Q S /Q T = (CcO2-CaO2)/(3.5+ CcO2-CaO2) when pulmonary catheter is not in place
/(CcO2-CvO2) Q S /Q T = (CcO2-CaO2)/(3.5+ CcO2-CaO2) when pulmonary catheter is not in place")
10
Oxygenation Status Monitoring Oxygen Delivery Do2 = CI Ca O2 CaO2 = SaO2 1.36 Hgb + (0.0031 PaO2) CI = CO/ BSA Normal Value: 800-1200 mL/min
 CI = CO/ BSA Normal Value: mL/min")
11
Oxygenation Dissociation Curve

12
Oxygenation Status Monitoring Oxygen Consumption Vo2=CI (CaO2-CvO2) CaO2 = SaO2 1.36 Hgb + (0.0031 PaO2) CvO2 = SvO2 1.36 Hgb + (0.0031 PvO2) Normal Value: 225-275 mL/min
 CaO2 = SaO2 1.36 Hgb + ( PaO2) CvO2 = SvO2 1.36 Hgb + ( PvO2) Normal Value: mL/min")
13
Oxygenation Status Monitoring Oxygen Extraction O2 ext = Vo2 / Do2 Normal value: 27%

14
Oxygenation Status Monitoring Relationship between Vo2 and Do2

15
Oxygenation Status Monitoring Oxygen Transport Variables

16
Anatomic and Capillary Shunts

17
Dead Space

18
Ventilation-Perfusion Inequality Acute Exacerbation of COPD 0.01 0.1 1 10 100

19
Ventilation-Perfusion Inequality Asthma 0.01 0.1 1 10 100

20
Ventilation-Perfusion Inequality Pulmonary Embolism 0.01 0.1 1 10 100

21
Shunting Process ARDS 0.01 1 10 100

22
The Effect of Increasing Ventilation- Perfusion Inequality on Arterial Po2 and Pco2

23
The effect of changing the inspired oxygen concentration on arterial Po2 for lung’s shunts of 10 to 50%

24
Assessment of Hypoxia

25
Ventilation Status Monitoring Tidal Volume: Vt Minute ventilation: Vm Respiration Rate: RR CO2 production: Vco2 Dead Space: V DS /V T

26
Dead Space Ventilation V D /V T =(Pa CO2 -PE CO2 )/Pa CO2 Normal is 0.2-0.4 PEco2 is measured by collecting condensate from the water trap on the expiratory limb of the ventilator circuit and the measure PCO2 using blood gas analyzer
/Pa CO2 Normal is PEco2 is measured by collecting condensate from the water trap on the expiratory limb of the ventilator circuit and the measure PCO2 using blood gas analyzer")
27
Causes of Increased Dead Space Ventilation Pulmonary embolism pulmonary hypoperfusion positive pressure ventilation High rate-low tidal volume ventilation

28
Arterial CO2 Pa CO2 = V CO2. 0.863/V E.(1-Vd/Vt)
")
29
High Minute Ventilation Increased CO2 production –Sepsis –Fever –Thyrotoxicosis –High carbohydrate feeding Increased ventilation: –Agitation –Pain –Central hyperventilation –Increased dead space

30
Low Minute Ventilation Decreased CO2 production –Hypothermia –Hypothyroidism –Severe sedation –Low carbohydrate feeding –Paralysis Decreased ventilation: –Sedation –Central hypoventilation –Decreased dead space

31
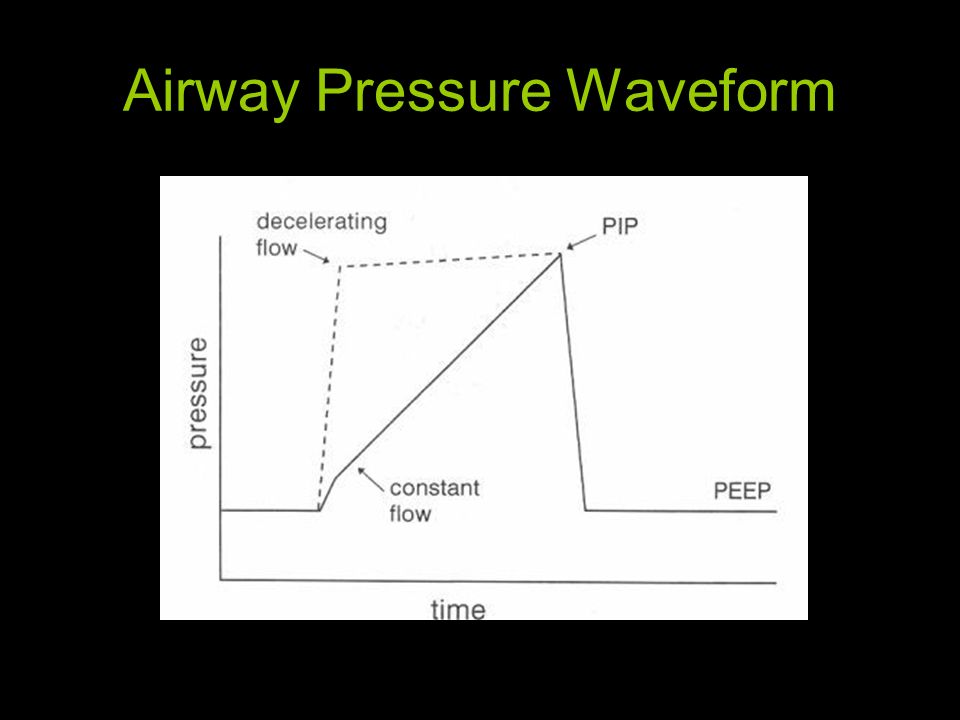
Airway Pressure Waveform

33
Pulmonary Mechanics Peak pressure Plateau pressure I E Airway Resistance

34
Mean Airway Pressure Paw= (PIP-PEEP).(T I /T T )+PEEP.(T E /T T )
.(T I /T T )+PEEP.(T E /T T )")
35
Methods to Increase Mean Airway Pressure Increase in tidal volume Increase in respiratory frequency Reduction in T E Decrease in respiratory flow rate: increase in T I Addition of end-inspiratory pause Addition of PEEP

36
Equation of Motion

37
Work of Breathing Mechanical work is performed when a force moves its point of application through a distance In the case of three dimensional fluid system, work is done when a pressure (P) changes the volume (V) of the system W = P.V: {PIP-(0.5). (Pplat)/100}.v T 0.5 J/L
/100}.v T 0.5 J/L.")
38
Static Pressure-volume curve in ARDS

39
Ventilatory System

40
Control Variables during Inspiration

41
Phase Variables

42
Modes of Ventilation

43
Breath Type during Mechanical Ventilation

44
Pressure Waveforms

45
Flow, Pressure, and Volume Waveforms with Constant Flow, Volume Ventilation

46
Flow, Pressure, and Volume Waveforms with Decelerating Ramp Flow, Volume Ventilation

47
Waveforms for Decelerating and Accelerating Ramp Flows

48
Full and Partial Decelerating Ramp Flow with Volume Ventilation

49
Flow, Pressure, and Volume Waveforms with Pressure Ventilation

50
Full and Modified Sine-flow Waveforms during Volume Ventilation

51
Flow, Pressure, and Volume Waveforms with Pressure Support Ventilation

52
Active Inspiration during Positive Pressure Ventilation

53
Airway Flow Waveform during Mechanical Ventilation

54
Airway Volume Waveform during Mechanical Ventilation

55
Flow-Volume and Pressure-Volume loops with COPD

56
Changes in Flow-Volume and Pressure- Volume loops with Bronchodilators

57
Pressure-Volume Loop Work Performed to Trigger the Ventilator

58
Pressure-Volume Loop Lung/Chest Wall Compliance

59
Dynamic Pressure-Volume LOOP Restrictive Work

60
Inspiratory Work of Breathing

61
Pressure-Volume Loop Deflection Points

62
Modes of Mechanical Ventilation Volume-Cycled Control Mode Ventilation

63
Modes of Mechanical Ventilation Assist-Control Ventilation

64
Indications: – for patients who are awake, moderately sedated or paralyzed and able to initiates ventilation –increase metabolic demands: infection, burns, multisystem organ failure –Respiratory muscle strengthening and weaning Limitations: –patient-ventilator dysynchrony –ventilator assisted hyperventilation in agitated patients with increased inspiratory drive –auto-PEEP in COPD patients

65
Modes of Mechanical Ventilation Intermittent Mandatory Ventilation

66
Modes of Mechanical Ventilation Synchronized Intermittent Mandatory Ventilation

67
Pressure Waveform for SIMV

68
Synchronized Intermittent Mandatory Ventilation Indications: –patients with minimal spontaneous respiratory efforts –respiratory muscle conditioning –ventilator weaning Limitations: –patient-ventilator dysynchrony especially in agitated patients –nonphysiologic way of respiratory muscle conditioning

69
Modes of Mechanical Ventilation Pressure Support Ventilation

70
Indications: –weaning –more physiologic conditioning of respiratory muscles: low pressure-high volume load –improved patient- ventilator dysynchrony Limitations:

71
Modes of Mechanical Ventilation Inverse Ratio Ventilation

72
Auto-PEEP

74
Normal Lung Mechanics and Gas Exchange

75
Severe Airflow Obstruction

76
Acute on Chronic Respiratory Failure

77
Acute Hypoxemic Respiratory Failure

Similar presentations