Download presentation
Presentation is loading. Please wait.

1
Laparoscopic Adrenalectomy
Michel Gagner Wahjoe Djatisoesanto

2
The incisions used during laparoscopic procedures do not tell the entire story.
The cuts are small on the outside, a great amount of work is done on the inside.

3
Introduction Laparoscopic adrenalectomy was described in 1992 by Gagner et al. Laparoscopic adrenalectomy has become the gold standard for the surgical treatment of most adrenal problem. The benefits: decreased hospital stay, shorter recovery time and improved patient satisfaction (decreased post-op pain and better cosmetic).
.")
4
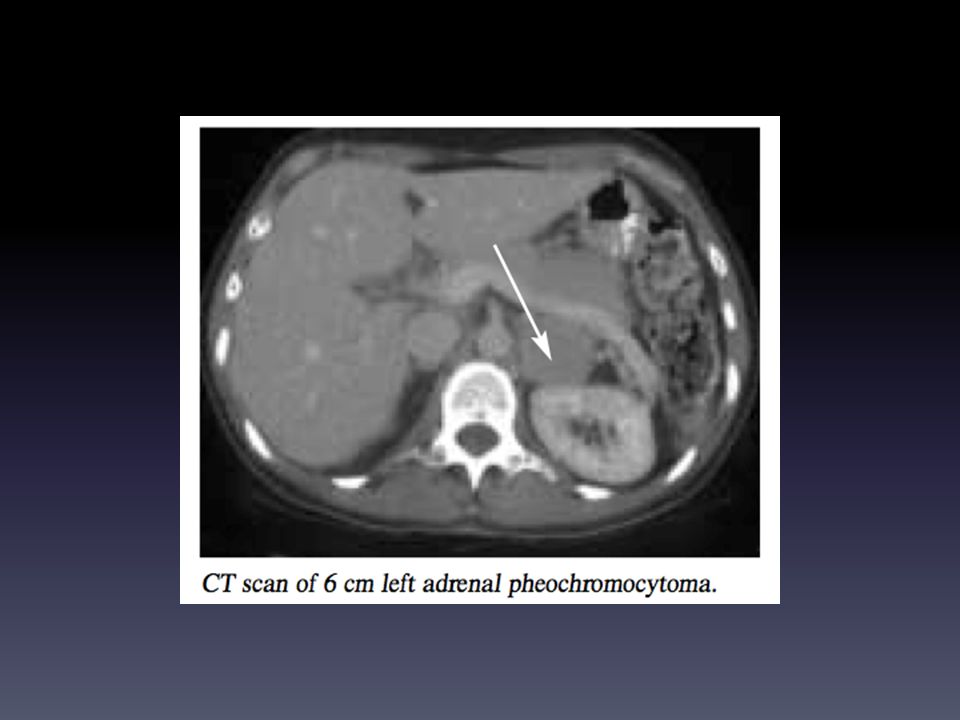
Indications The most common indication is a unilateral benign adrenal lesion: Incidentalomas Pheochromocytomas Aldosteronomas Cushing’s syndrome Less common Adrenal cysts Myelolipomas Androgen-secreting tumors Ganglioneuromas Adrenal hemorrhage

10
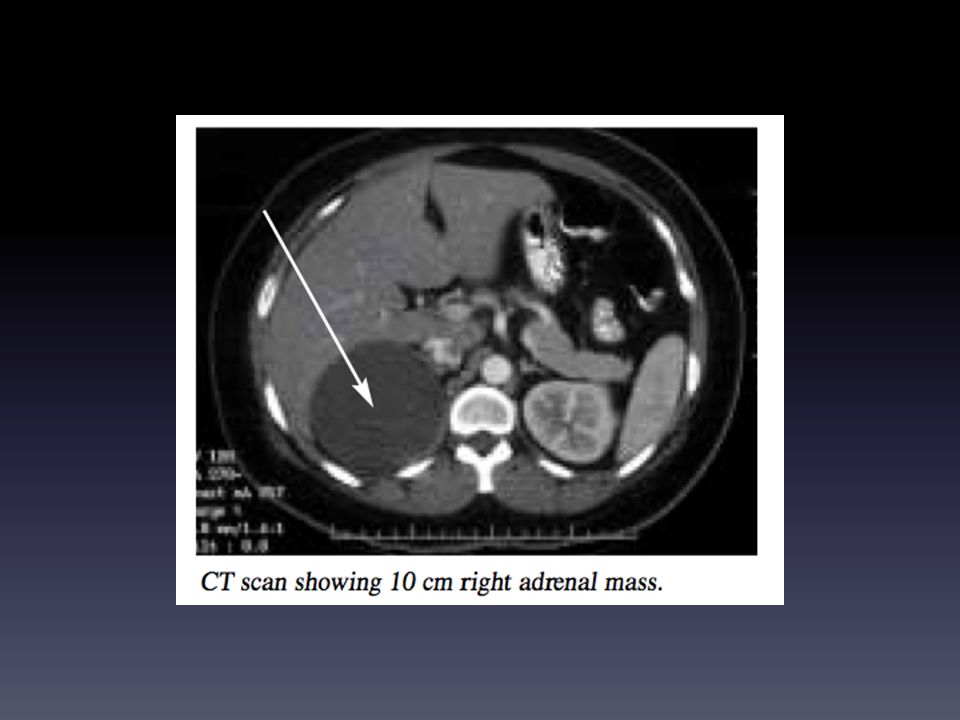
Contraindications Tumors larger than 12 cm likely containing malignancy and local invasion. Metastatic adrenal disease and adrenocortical carcinoma (still debate) Obesity, significant cardiopulmonary disease, coagulopathy (relative contraindications).
 Obesity, significant cardiopulmonary disease, coagulopathy (relative contraindications).")
11
Operative technique The laparoscopic approach to the adrenals
Transperitoneal adrenalectomy anterior (ATA) Lateral transperitoneal adrenalectomy (LTA) Retroperitoneal adrenalectomy (REA) No evidence indicating that one approach is superior to the other. Which approach to use depends on personal preferences
 Lateral transperitoneal adrenalectomy (LTA) Retroperitoneal adrenalectomy (REA) No evidence indicating that one approach is superior to the other. Which approach to use depends on personal preferences.")
12
Transperitoneal Laparoscopic Adrenalectomy

13
Laparoscopic right adrenalectomy

14
The right adrenal gland
Larger than the left one An endocrine organ with a variable shape Located at the medial aspect of the upper pole of the right kidney Retroperitoneal position and not attached to the kidney

15
Operating room set-up

16
Position General anesthesia Full left lateral decubitus position
Both legs slighly flexed to avoid crural neuropathy Cushion placed under left flank Table flexed to widen the space between the anterior iliac spine and inferior costal margin Position

17
Team 1. The Surgeon stands on the abdominal side of the patient.
2 and 3. Two assistants stand on the other side of the patient. Two video monitors are used. Team

18
Equipment Operating table Anesthetic equipment Laparoscopic units
Monitor Electrocautery Instrument table Equipment

19
Pneumoperitoneum A pneumoperitoneum at mmHg is established in a standard fashion according to the operating surgeon’s preference. Only 4 trocars (10mm) are necessary to perform a laparoscopic right adrenalectomy transperitoneal approach. The position of the trocars may vary with the patient’s body habitus.
 are necessary to perform a laparoscopic right adrenalectomy transperitoneal approach. The position of the trocars may vary with the patient’s body habitus.")
20
The first 10 mm optical trocar is inserted in the anterior axillary line, under the costal margin.
The 0° laparoscope is introduced through this trocar. It is preferable to introduce this first trocar under direct vision using the open technique.

21
A second 10 mm trocar is introduced 5 cm from the optical trocar, 2 cm anterior to the anterior axillary line.

22
Two other 10 mm trocars are introduced under direct vision.
Both are placed under the costal margin, 7 cm on either side of the optical trocar. Initially, a grasper is introduced through each trocar and used to expose the operating field to be dessected. The liver retractor will be introduced through the trocar on the left.

23
A 0° laparoscope is commonly used.
A 30° laparoscope may be necessary, especially: In obese patients In case of large tumors

24
Operating devices

25
Other devices

26
Mayor principle Based on complete dissection of the right adrenal gland without specifically identifying the gland itself. The vena cava constitutes the main anatomical landmark in this strategy. It is dissected first because it is easily identified and leads directly to the right adrenal gland.

27
The adrenal gland is located along the upper pole of the internal aspect of the kidney and sometimes covering it. The gland is surrounded by fatty tissue. It is firm yet extremely friable and therefore particularly difficult to manipulate during surgical procedures.

28
The procedure begins with the incision of the subhepatic peritoneum using either a coagulating hook or scissors. Frees the triangular ligament from the liver, resulting in the complete mobilization of the liver The gallbladder, which is situated outside of the operating field, is left untouched.

29
Dissection Mobilization of the liver allows identification of the vena cava. Exposing the renal vein: the vena cava is dissected caudally and then cephalad. The main adrenal vein

30
The main adrenal vein The accessory adrenal vein

31
The main adrenal vein therefore easily dissected for 1 cm and clipped under optimal safety conditions with 2 clips. The vein is then divided and the gland retracted caudally.

32
Captions

33
The middle adrenal artery, which originates from the aorta, is located either posterior or inferior to the main adrenal vein. It’s identified and dissected from the aorta in the fatty tissue, and then clipped and divided.

34
The superior adrenal artery, which originates from an inferior phrenic artery, is identified at the upper pole of the gland below the liver. It is dissected, clipped, and divided.

35
The inferior adrenal artery, which usually originates from the renal artery, is located on the postero-inferior aspect of the gland. Clipping and division of the inferior adrenal artery. The inferior pole and internal aspect of the gland are then completely freed from both the vena cava and the renal vessels.

36
Captions

37
End of the dissection The vascular network of the gland is almost completely divided. The goal is to free the gland completely and proceed to its extraction. The few attachments are carefully dissected using either a monopolar coagulating hook or a bipolar grasper.

38
Conclusion Laparoscopic adrenalectomy is the gold standard for removal of adrenal tumor. There are three kind approach: Anterior transperitoneal, Lateral transperitoneal and Retroperitoneal adrenalectomy. Malignancy is no longer considered an absolute contraindication to the laparoscopic approach, unless invasion of the nearby organs or the vasculature has occurred.

39
Thank you

Similar presentations