Download presentation
Presentation is loading. Please wait.

1
Inner Ear Disorders Lecture 14 Adults

2
Most common occurring causes of SNHL
Noise Presbycusis Meniere’s disease Immune Disease Ototoxicity Diabetes

3
Noise Induced HL Most common form of preventable HL
Result from exposure to intense noise levels Permanent threshold shift (PTS) Temporary threshold shift (TTS) – recovers within hours Acoustic Trauma: impulsive sound
 Temporary threshold shift (TTS) – recovers within hours. Acoustic Trauma: impulsive sound.")
4
Noise Induced Hearing Loss
More common in men with histories of noise exposure Increasing incidence among children Site of pathology: basal end hair cells- primarily OHC

5
http://www. neurophys. wisc

6
Symptoms of NIHL Tinnitus Difficulty understanding in noise
Difficulty understanding speech

7
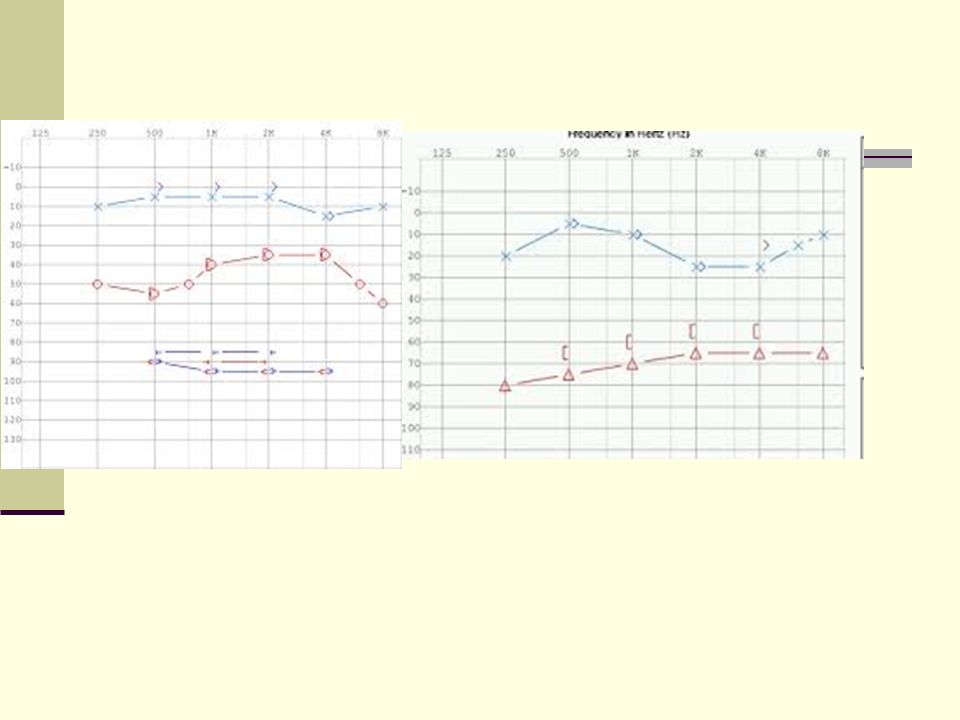
Audiometric Results Otoscopy: Tympanometry: Pure tone Air and Bone OAE
Maximal HL between Hz – “Noise Notch” OAE ABR Lowest Level for wave V IWI

8
Safe vs. Unsafe Sound Levels
Noise levels measured in dB SPL Any loud noise over 85dB is considered loud enough to cause NIHL. 80 dB ….shouting. 110 dB….concert or sporting event. 111 dB…. iPod on full volume. 130 dB …an airplane taking off 100m away. 140 dB ….level at which noise causes pain for most people

9
iPods Percent of Maximum Volume <= 40% 50% 60% 70% 80% 90% 100%
Equivalent Volume dB <= 73dB 81dB 87dB 92dB 98dB 106dB 111dB Time you can use before Hearing Loss WILL Occur Unlimited 8 hours 4.5 hours 1.6 hours 23 minutes 4 minutes 1 minute

10
Metrics for Noise Max sound level is the highest sound level recorded over a period of time Average sound level is the average sound measured over a period of time Noise dose is a percentage of the daily maximum permissible exposure. 100% dose is equivalent to an 85 dBA time-weighted average for 8 hours. Noise Dose: 100%

11
Prevention of HL Walk Away Turn it down Use earplugs
Duration per Day, hours Sound Level dBA 8 90 6 92 4.2 95 3 97 2 100 1.5 102 1 105 .5 110 .25 115 Walk Away Turn it down Use earplugs Educate students about NIHL OSHA NOISE guidelines

12
Education about Prevention of HL
13
Presbycusis The most common cause of SNHL associated w/ aging
Site of pathology: hair cell damage in cochlea By years, pure tone thresholds show drop in hearing in the high frequencies By years of age, the lower frequencies become affected

14
6 Types of Presbycusis Schuknecht and Gacek 1993
Sensory Neural Strial Cochlear Conductive Mixed Presbycusis Intermediate Presbycusis

15
Sensory Presbycusis (*Otle, Schukneckt & Kerr, 1978)
*Loss of inner and outer hair cells Loss of supporting cell structure; degeneration of the Organ of Corti Differential diagnosis is difficult Aging vs acoustic trauma SNHL begins in high frequency range Possible mechanisms for intervention Susceptibility of hair cells to aminoglycosides Genetics

16
Neural Presbycusis (*Otto, Schukneckt & Kerr 1978)
Loose 2,000 neurons per decade – S. Ganglion less than 20,000 in adults years of age *Loss of 50% of cochlear neurons, greater in the elderly over 80 years of age = 15,000 from 30,000 as a young adult Most consistent pathological change in older ear Associated with poorer than expected word recognition

17
Stria Presbycusis Atrophy of the stria vascularis
Function also dependent on capillary beds Stria Presbycusis Atrophy of the stria vascularis Affects production of endolymph – important to maintaining the electrochemical balance of inner ear fluids (ion transport mechanism ) Variable audiometric findings Stria Vascularis
 Variable audiometric findings. Stria. Vascularis.")
18
Summary of Presbycusis
2 major age related structural changes - Inner Ear - Auditory Nerve 6 Classifications of Presbycusis affecting any or a combination of: - hair cells, supporting structures - stria vascularis - spiral ganglia, neurons - nerve fibers of the 8th cranial nerve

19
Audiometric Results Otoscopy: Tympanometry: Pure tone Air and Bone OAE
ABR Lowest Level for wave V IWI

20
Endolymphatic Hydrops/Meniere’s Disease
1/1000 persons suffers MD Symptoms Sudden attacks of vertigo, tinnitus, vomiting and Unilateral SNHL Onset y/o

21
Endolymphatic Hydrops/Meniere’s Disease
Site of Pathology: Vestibular system Malfunction of ES - overproduction of endolymph in the inner ear causes increased pressure on hair cells Etiology: unknown, ES blockage, constriction in blood vessels, migraine, autoimmune reaction, genetic connection, viral infection etc.

22
Endolymphatic Sac ES – important for keeping fluid levels constant
Research ongoing to ID mechanisms that regulate endolymph production

23
Endolymph Hydrops/ Meniere’s Disease
2 parts to the labyrinth: the bony and membranous labyrinth. Membranous labyrinth is filled endolymph Increased production of endolymph alters chemical balance of inner ear The release of endolymph results in a major disturbance of the normal chemical composition of the perilymph in scala vestibuli. As scala vestibuli has a wide communication with perilymph of the vestibule, the chemical disturbance will spread into the vestibular system. The high-potassium endolymph is highly toxic to cells not specialized to deal with it. Cells become depolarized (activating transmitter release and afferent nerve fiber activity) and swell in a high-potassium environment, resulting in auditory and vestibular dysfunction. Perilymph (Na) Endolymph (K+)
 and swell in a high-potassium environment, resulting in auditory and vestibular dysfunction. Perilymph (Na) Endolymph (K+)")
24
Endolymph Hydrops/ Meniere’s
If head moves> endolymph moves and sends vestibular sensory info to the brain Increase in endolymph > the membranous labyrinth dilates> vertigo > “endolymphatic hydrops”

25
Meniere’s Disease Ménière's disease thought to be more than E. Hydrops. Possible rupture of the membranous labyrinth> endolymph mixes with perilymph. The mix of perilymph and endolymph is thought to cause symptoms of Ménière's disease

26
Treatment for Meniere’s
No known cure > management of symptoms Acute Vasodialators, Corticosteroids – improve blood flow to cochlea, anti-inflammatory effect Anti vertigo medications Phenergen, dramamine ,antivert,valium Maintenance Diuretics limit sodium in diet Amplification Vestibular rehabilitation Tx

27
Surgical Treatment Endolymphatic Sac Surgery – decompress the sac/shunt insertion (not common today) Aggressive Tx approaches Labyrinthectomy – removal of vestibular organ- causes total deafness in affected ear Vestibular Neurectomy – partially sever the affected nerve Current approach: Infusion of TM with corticosteroids

28
Audiometric Findings Onset starts with unilateral LF SNHL
Fluctuations in hearing and “Flattening” of shape of audiogram as disease progresses n

29
Audiometric Results Otoscopy: Tympanometry: Pure tone Air and Bone OAE
ABR Lowest Level for wave V IWI

30
Tests to assist with Differential Diagnosis
Auditory Brainstem Response (ABR) test Electronystagmography: ENG VEMPs MRI
 test. Electronystagmography: ENG. VEMPs. MRI.")
31
Autoimmune inner ear disease (AIED)
Inflammatory condition of the inner ear Inner ear proteins are recognized as foreign Primary process Secondary to trauma or inflammation Occurs when the body's immune system attacks cells in the inner ear that are mistaken for a virus or bacteria

32
Symptoms & Incidence Incidence:
<1% of the 28 million Americans with a HL 2/3 females, middle aged Sudden SNHL in one ear but becomes bilat progressing rapidly to second ear (<3 mos) Aural fullness Dizziness/vertigo
 Aural fullness. Dizziness/vertigo.")
33
Theory and Symptoms of AIED
Cochlea is devoid of immune cells Antibodies/ rogue T-cells (type of white blood cell) that circulate around body to look for cell abnormalities and infections T-cells essential for immunity Rogue T-cells cause inner ear damage
 that circulate around body to look for cell abnormalities and infections. T-cells essential for immunity. Rogue T-cells cause inner ear damage.")
34
Treatment Drug therapy: steroids, prednisone and methotrexate – (used in chemotherapy) If received early in disease, very helpful Often results in severe to profound bilateral SNHL Amplification Cochlear implant

36
Differential Testing ABR ENG Blood Tests Immunofluorescence
labeling of antibodies with fluorescent dyes Audiometric Evaluations

37
Audiometric Results Otoscopy: Tympanometry: Pure tone Air and Bone OAE
ABR Lowest Level for wave V IWI

38
Ototoxicity Consider Toxicity is related to
Sometimes the medicine is worse than the disease Sometimes there is no choice when presented with life threatening conditions Toxicity is related to Dosage Duration of administration

40
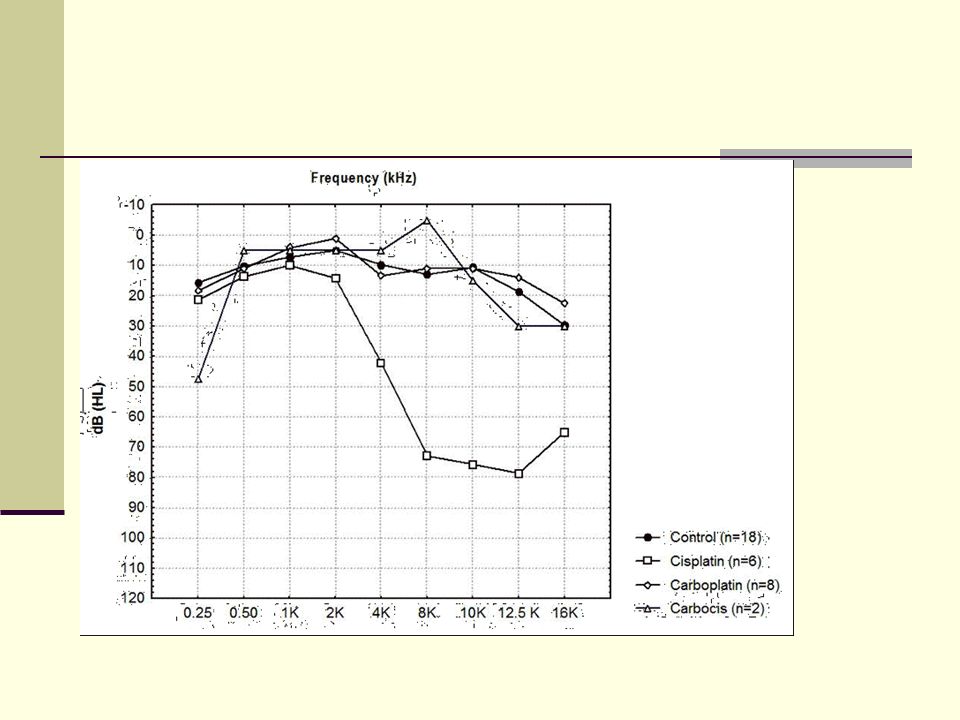
Common ototoxic drugs Aminoglycosides antibiotics Antineoplastic drugs
Treat infections Gentamicin, kanamycin, neomycin, streptomycin, tobramycin Antineoplastic drugs Treatment of cancer and tumors Cisplatin,carboplatin, nitorgen mustard

41
Common ototoxic drugs Diuretics and loop diruetics Salicylates Quinine
Treatment of congestive heart failure, pulmonary edema Lasix, bumetanide Salicylates Treatment of arthritis, rheumatic fever, connective tissue disorders Aspirin Quinine Uncommon- Tx malaria

42
Common ototoxic drugs Environmental chemicals Arsenic Mercury Tin Lead

43
Common Symptoms Impaired renal function
Permanent SNHL – bilateral and mostly high frequencies Tinnitus Can occur suddenly Speech recognition reduced

44
Main mechanism Free radicals form and anti-oxidant inhibition result in HL Damages cells in cochlea Apoptosis – cell death

45
Audiometric Results Otoscopy: Tympanometry: Pure tone Air and Bone OAE
ABR Lowest Level for wave V IWI

46
Treatments Avoid or reduce doses of ototoxic agents as possible
Monitor hearing Substitute with a different agent SNHL – HA

47
Diabetes Elevated blood glucose levels affect inner ear hair cells
Progressive bilateral SNHL Often affects visual acuity Dual Sensory loss

48
Treatment Audiologic Monitoring
Pure tone audiometry – esp in high freq Speech audiometry – discrim may be very poor when compared to pure tone thresholds Otoacoustic emissions – most sensitive and earliest detector of cochlear damage

49
Audiometric Results Otoscopy: Tympanometry: Pure tone Air and Bone OAE
ABR Lowest Level for wave V IWI

50
AMA Criteria for Medical Referral
visible congenital, traumatic deformity history active drainage/bleeding from the ear sudden, rapidly progressive loss (90 days) acute/chronic dizziness unilateral loss of sudden, recent onset (90 days) ABG ≥ , 1000, 2000 Hz significant cerumen accumulation, foreign body Ear pain or discomfort
 acute/chronic dizziness. unilateral loss of sudden, recent onset (90 days) ABG ≥ , 1000, 2000 Hz. significant cerumen accumulation, foreign body. Ear pain or discomfort.")
Similar presentations