Download presentation
Presentation is loading. Please wait.

1
Care at the end of life in hospital Dr David Oliver Consultant Physician Wisdom Hospice Honorary Reader University of Kent D.J.Oliver@kent.ac.uk

3
Palliative Care An approach that improves the quality of life of patients and their families facing problems associated with life threatening illness, through the prevention and relief of suffering, early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual W.H.O. 2002
4
Palliative care aims Provides relief from pain and other distressing symptoms Affirms life and regards dying as a normal process Intends neither to hasten or postpone death Integrates the psychological and spiritual aspects of patient care

5
Symptom management All aspects of care need to be considered Physical Psychological Social Spiritual

6
Symptoms Weakness87% Pain77% Weight loss76% Anorexia66% Dry mouth58% Dyspnoea57% Constipation46% Nausea37%

7
Which patients? Cancer Palliative chemotherapy COPD Heart failure Neurological disease Dementia ?Elderly frail

8
Who? 45 year old man with carcinoma of lung and brain metastases 65 year old man with COPD 78 year old lady with renal failure – but decision made not to use dialysis 98 year old man in residential home with dementia 44 year old lady post op following breast lump excision – carcinoma found

9
The End of Life Care Pathway Support for carers and families Information for patients and carers Spiritual care services Step 2 Assessment, care planning and review Agreed care plan and regular review of needs and preferences Assessing needs of carers Step 3 Coordination of care Strategic coordination Coordination of individual patient care Step 4 Delivery of high quality services in different settings Requires the individuals to have appropriate knowledge and skills to deliver high quality care Step 5 Care in the last days of life Identification of the dying phase Review of needs and preferences for place of death Support for both patient and carer Recognition of wishes Regarding resuscitation and organ donation Step 6 Care after death Recognition that end of life care does not stop at the point of death. Timely verification and certification of death or referral to coroner Care and support of carer and family, Including emotional and practical bereavement support Discussions as the end of life approaches Open, honest communication Identifying triggers for discussion Step 1

10
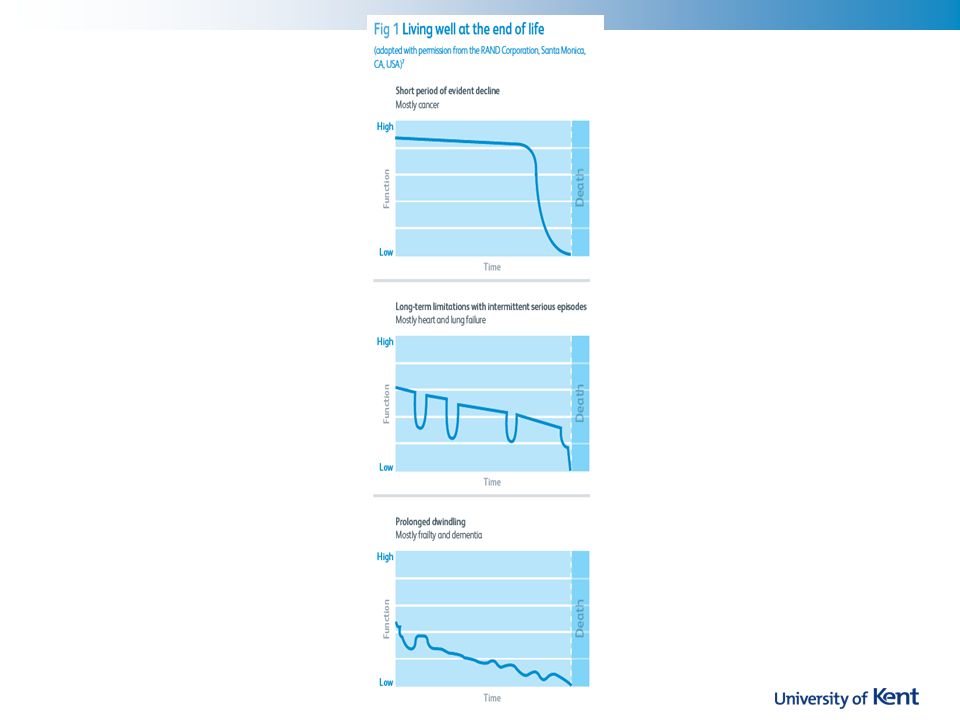
People in the last year of life - RCP report 90% of patients die from a previously diagnosed condition. For patients who are older and frail or have advanced progressive disease, prognostic factors could include: –a ‘No’ answer to the question ‘Would I be surprised if the patient were to die in the next 12 months’ –two or more unplanned admissions in the last 6 months –poor or deteriorating performance status –persistent symptoms despite optimal therapy –secondary organ failure arising from an underlying condition.

12
Identification Surprise question Would you be surprised if this person died in the next 12 months? The gut feeling Triggers Repeated admissions No improvement after admission Decline in mental /physical state Bed bound

13
Which patients? Cancer Palliative chemotherapy COPD Heart failure Neurological disease Dementia ?Elderly frail

14
Aims of care Assess and review Reduce unnecessary medication and interventions Ensure appropriate medication available Symptom management essential Support family and carers Anticipate and prepare

15
General principles in last few days of life Assess symptoms regularly Team approach Assess current medication and discontinue non-essentials Stop statins Medication available if required Pain, vomiting, agitation, chest secretions

16
Overall aim Deterioration in patient’s condition suggests that the patient is dying Multidisciplinary assessment Is there a potentially reversible cause? Could the patient be in the last hours / days of life? Is specialist involvement needed Specialist palliative care advice / involvement

17
“Less complex patients” GP care District nurse Advice from specialist teams Hospice Respiratory team Heart failure team MS / PD nurses Cancer site specific CNS Planning

18
Ensuring appropriate treatment / interventions at end of life Home District nurse GP visit – to ensure death certificate DS1500 DNACPR End of life register (My wishes register) Palliative care practice meetings “Message in the bottle” Preferred place of death Advance care planning
 Palliative care practice meetings Message in the bottle Preferred place of death Advance care planning")
19
Nursing / residential homes Plans DNACPR My Wishes register Discussions / care plans Advance care planning Residential home – district nurse Regular visits – death certification Palliative care practice meetings

20
Palliative care practice meetings GP District nurse Community Palliative Care Team CNS Discuss patients on palliative care register Some under CPCT Many under GP / DN care Advice and support

21
Specialist referral Complex symptoms Complex needs Physical Psychosocial Spiritual

22
Common symptoms in last 24 – 48 hours Pain Nausea and vomiting Dyspnoea Restlessness and agitation Chest secretions

23
Parenteral medication Nausea and vomiting Dysphagia Severe weakness / coma Intestinal obstruction Rarely Pain control Compliance

24
Pain Non-drug management Positioning Support and reassurance Bladder and bowel care Mouth care Drug management Continue medication Route of administration

25
Pain Medication Morphine parenterally Fentanyl transdermally Route Oral Parenteral Injection Infusion subcutaneously

26
Pain Morphine parenterally Oral morphine 20mg = morphine im/sc 10mg Total 24 hour oral morphine 50% as subcutaneous infusion Total 24 hour parenteral morphine Equivalent dose as subcutaneous infusion

27
Breathlessness -Drug Management Drugs to relieve awareness of breathlessness Morphine Drugs to relieve fear and anxiety if patient is breathless Lorazepam –500 micrograms sublingually Midazolam –2.5-10 mg every 4 hours Consider oxygen

28
Agitation - Non-Drug Management Treat reversible causes Urinary retention Constipation Pain Identify and address psychological issues Fear Isolation Spiritual distress

29
Agitation- Drug Management Midazolam –2.5-5mg S/C PRN –20-60mg+ / 24 hours Levomepromazine –12.5 - 25 mg S/C PRN –25-150mg / 24 hours

30
Explanation and reassurance to family/carers Repositioning Suctioning (rarely needed) Chest secretions –non-drug management
 Chest secretions –non-drug management")
31
Chest secretions – drug management Drug treatment is effective for relief of retained secretions in only ~ 50% patients Glycopyrronium bromide 200micrograms every 4 hours 600- 1200 micrograms / 24 hours Hyoscine hydrobomide 400 micrograms every 4 hours 2400-3600micrograms / 24 hours

32
Advance care planning Advance statements Non-specific but shows the person’s views Advance decisions to refuse treatment If specific legally binding Lasting Power of Attorney Health Financial Discussion of place of care and death Allows planning for person and family

33
Who? 55 year old man with lung cancer 65 year old man with MND 77 year old lady with early dementia 66 year old man in residential care with Huntington’s disease 45 year old man who is fit and healthy 22 year old man with Duchenne’s MD and on non-invasive ventilation

34
Conclusions Recognition of dying phase Appropriate care Stopping inappropriate medication / investigations Ensuring medication available Support Patient Family Staff

37
Total pain Physical Psychological Social Spiritual

38
Pain “A passion of the soul”Aristotle “A somatopsychic experience” how we feel affects the pain how we are generally affects the pain other symptoms psychological and social aspects

39
Pain Perception of pain influenced by Mood of patient Morale of patient Meaning of the pain for the patient

40
Assessment of Pain Type of pain Ache, sharp, burning Time Duration of pain When does it come Factors increasing pain Movement? Lying? Standing? Factors decreasing pain Rest? Rubbing? Where? Does it radiate When

41
Pain management Explanation Modification of pathological process Increase the pain tolerance threshold Modify the pattern of living Interruption of pain pathways Modulation of pain transmission

42
Explanation Reduces the psychological impact of the pain Shows interest in the pain and its management Helps to establish trust

43
Modification of pathological process Radiotherapy Chemotherapy Hormone therapy Surgery Hypercalcaemia treatment Antibiotics / antifungals / antivirals

44
Increase pain thresh old Insomnia Anger Depression Boredom Analgesics Anxiety Fear Sadness Social Isolation

45
Modification of pattern of living Avoid pain precipitating activities Immobilization – collar, corset, sling, surgery Walking Aid Wheelchair Hoist Involve Physiotherapy Occupational therapy

46
Interruption of pain pathways Nerve blocks Epidural Sympathetic blocks Neurosurgery cordotomy

47
Modulation of pain pathways Non pharmacological TENS Acupuncture Pharmacological Co-analgesics drugs acting in conjunction with opioids

48
Pain management Analyse the cause Regular analgesia Titrate the dose Adjuvant medication Medication Nerve blocks Radiotherapy Remember other pains Psycho-social, spiritual

49
Strong Opioid +/- adjuvant Weak Opioid +/- adjuvant Non Opioid +/- adjuvant World Health Organization Analgesic Ladder

50
Non-opioids Aspirin Paracetamol Nonsteroidals Ibuprofen REGULAR TITRATED TO PATIENT

51
Weaker opioids Codeine Dihydrocodeine Tramadol

52
Strong Opioid +/- adjuvant Weak Opioid +/- adjuvant Non Opioid +/- adjuvant World Health Organization Analgesic Ladder

53
Opioids Morphine Fentanyl Oxycodone Buprenorphine

54
Morphine Strong opioid of choice Effective Cost effective Safe if used properly Oral MST tablets 12 hourly Morphine elixir 4 hourly Morphine IR tablets 4 hourly

55
Use of morphine Start with low dose 5-10mg 4 hourly 10-20mg 12 hourly Increase dose if pain breaks through Do not decrease interval Night – often no extra dose needed

Similar presentations