Download presentation
Presentation is loading. Please wait.

3
Associate Professor, Department of Emergency Medicine Senior Scientist, Ottawa Hospital Research Institute Research Chair in Emergency Cardiac Resuscitation, University of Ottawa Associate Medical Director, Regional Paramedic Program for Eastern Ontario

4
None financial Received peer-reviewed funding No promotion of off-label use of drugs or devices

5
C-Spine immobilization for all...time to reconsider! OBHG 2013

6
Objectives To review current immobilization practices To review current immobilization practices To describe the derivation and validation of the Canadian C-Spine Rule To describe the derivation and validation of the Canadian C-Spine Rule To illustrate its application by paramedics in the field To illustrate its application by paramedics in the field

7
Who Should Be Immobilised?

8
Current Medical Directive Potential C-Spine injury if: Neck pain with any mechanism of injury No neck pain, but some visible injury above the clavicles, and/or Neither neck pain nor visible injury, but significant mechanism of injury as determined by the paramedic

9
Some Numbers… 185,000 ED visits per year in Canada (enough for 3 large EDs, full time) Only 1% have bony c-spine injury Less than 0.5% spinal cord injury
 Only 1% have bony c-spine injury Less than 0.5% spinal cord injury")
10
C-Spine Immobilisation

12
Transportation…no difference -US EMS VS Kuala Lumpur Malaysia N=454 AEM, 1998 -Cochrane review by Kwan, 2009 VS

13
The Damage is Done Initially! Current immobilization practice is mostly opinion based, with no real scientific background.

14
Goals of Management 1. Restore and maintain of alignment 2. Protect the spinal cord and transport safely 3. Establish permanent stability

15
What are YOUR goals? Identify all with a C-Spine injury Identify all with a C-Spine injury Save time and resources Save time and resources Minimise discomfort Minimise discomfort

16
What the Back Board does to You… Progressive pain in head, neck, and back Progressive pain in head, neck, and back Claustrophobia / Agitation Claustrophobia / Agitation Risk of aspiration Risk of aspiration Time and resource utilisation Time and resource utilisation Decubitus ulcer formation Decubitus ulcer formation Process can start within 30 min, and lead to systemic infections

17
The Canadian C-Spine Rule Radiography in Alert & Stable Trauma Patients

18
Clinically Unimportant Injuries Require neither specialized treatment nor follow-up: Isolated avulsion fracture of osteophyte Isolated fracture of transverse process not involving body or facet joint Isolated fracture of spinous process not involving the lamina Isolated simple compression fracture < 25% of body height

20
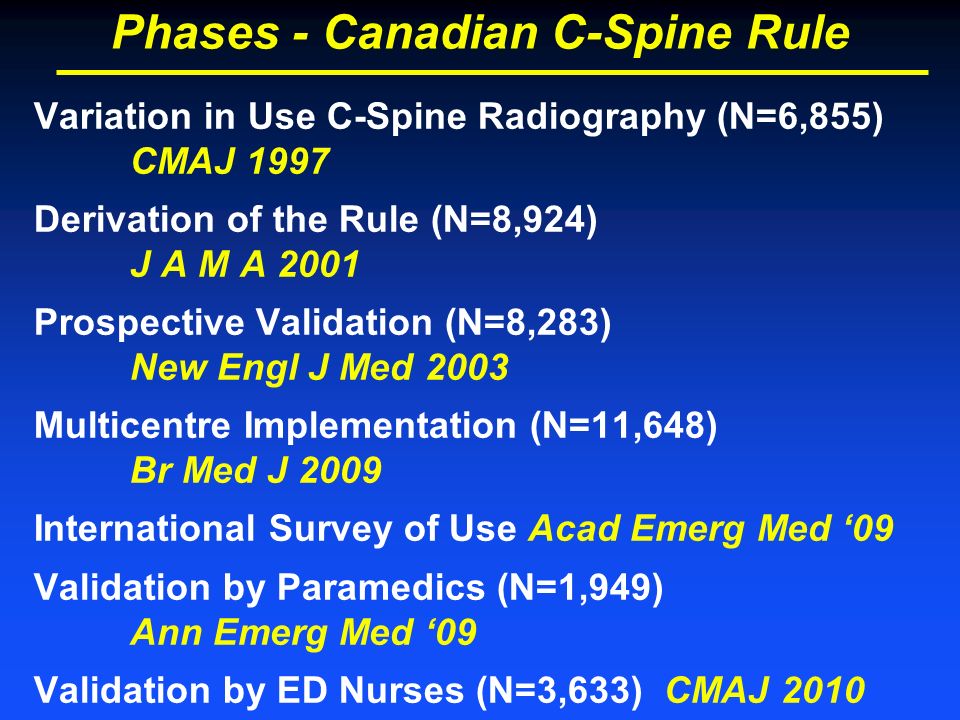
Phases - Canadian C-Spine Rule Variation in Use C-Spine Radiography (N=6,855) CMAJ 1997 Derivation of the Rule (N=8,924) J A M A 2001 Prospective Validation (N=8,283) New Engl J Med 2003 Multicentre Implementation (N=11,648) Br Med J 2009 International Survey of Use Acad Emerg Med ‘09 Validation by Paramedics (N=1,949) Ann Emerg Med ‘09 Validation by ED Nurses (N=3,633) CMAJ 2010
 CMAJ 1997 Derivation of the Rule (N=8,924) J A M A 2001 Prospective Validation (N=8,283) New Engl J Med 2003 Multicentre Implementation (N=11,648) Br Med J 2009 International Survey of Use Acad Emerg Med ‘09 Validation by Paramedics (N=1,949) Ann Emerg Med ‘09 Validation by ED Nurses (N=3,633) CMAJ 2010")
21
Classification Performance for 151 ‘Clinically Important’ Injury Cases C-Spine Injury YesNo Rule Positive Yes1515041 No 03732 Sensitivity100% (98-100) Specificity42.5% (42-44) NPV 100% X-ray Rate 58.2%
 Specificity42.5% (42-44) NPV 100% X-ray Rate 58.2%")
22
Classification Performance for 162 ‘Clinically Important’ Injury Cases* C-Spine Injury YesNo Rule Positive Yes1613995 No 13281 Sensitivity99.4% (96-100) Specificity45.1% (44-46) NPV 100% *845 cases were indeterminate (no neck rotation)
 Specificity45.1% (44-46) NPV 100% *845 cases were indeterminate (no neck rotation)")
23
After evaluation of 313 ‘clinically important’ injuries in 16,362 patients… Only one was ever missed: 18 year old involved in MVC Ambulatory at the scene Normal Xray during initial ED visit He returned one week later… Type II odontoid fracture found on CT Discharged home with a hard collar and no complication

24
Phase II Prospective Validation of the use of the Canadian C-Spine Rule by Triage Nurses

27
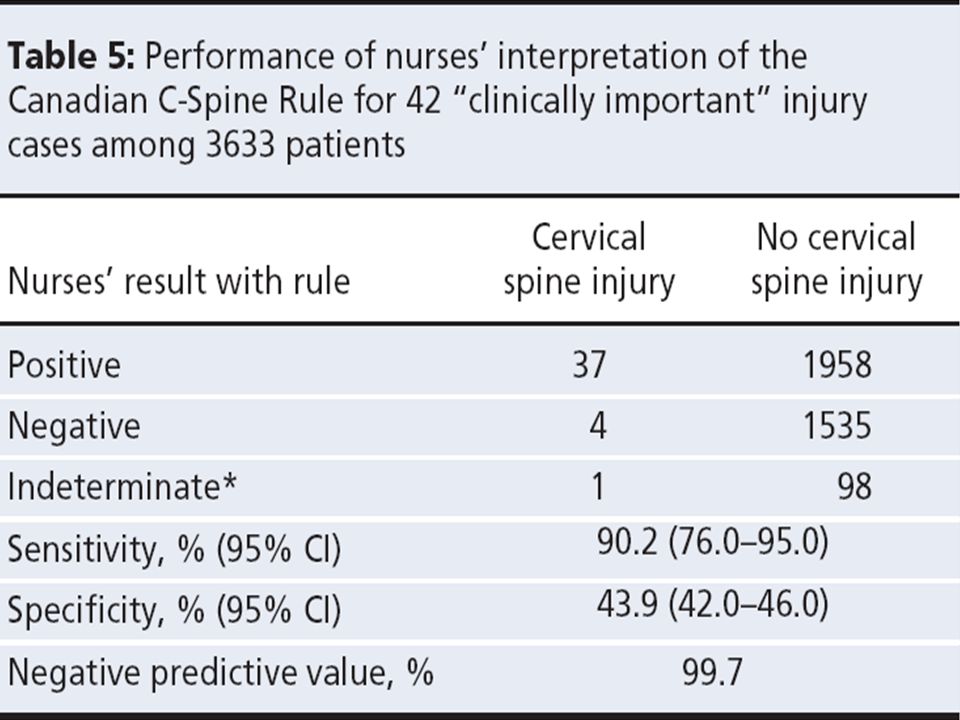
After evaluation of 42 ‘clinically important’ injuries in 3,633 patients… None were misses by “the rule” Four would have been missed by nurses, all involved overlooking a dangerous mechanism: Age 65 Fell down many stairs Ejected from car during MVC Numbness in extremities None on the 4 had in a spinal cord injury

28
Phase II Prospective Pre-Hospital Validation of the Canadian C-Spine Rule Took place between 2002 - 2006 Tested on 1,947 patients with 12 clinically important c-spine injuries

29
Published in Annals of Emergency Medicine, 2009 Voted top 10 paper for 2009 by National Association of EMS Physicians Top 25 downloads from Journal website for more than 6 months in a row

30
Recruitment by Center

31
Patient Characteristics (N= 1,947) Age (median)39 Male Gender49% Mechanism MVC63% Falls20% Pedestrian struck 2% Bicycle struck 2% Admitted to Hospital11% C-Spine Fracture (n=12)0.6%
 Age (median)39 Male Gender49% Mechanism MVC63% Falls20% Pedestrian struck 2% Bicycle struck 2% Admitted to Hospital11% C-Spine Fracture (n=12)0.6%")
32
Patient Outcomes (N = 1,947) Cervical spine injury (n, %) 18 0.9% Fracture 14 0.7% Clinically important injury 12 0.6% Ligamentous instability 7 0.4% Dislocation 3 0.2% Stabilizing treatments (n, %) 6 0.3% Internal fixation 5 0.3% Rigid collar 3 0.2% Brace 2 0.1% Halo 1 0.1%
 Cervical spine injury (n, %) % Fracture % Clinically important injury % Ligamentous instability 7 0.4% Dislocation 3 0.2% Stabilizing treatments (n, %) 6 0.3% Internal fixation 5 0.3% Rigid collar 3 0.2% Brace 2 0.1% Halo 1 0.1%")
33
Classification Performance for 12 ‘Clinically Important’ Injury Cases C-Spine Injury YesNo Paramedic Pos. Yes 121,204 No 0 731 Sensitivity 100% (74-100) Specificity37.7% (36-40) NPV 100%
 Specificity37.7% (36-40) NPV 100%.")
34
Excellent Agreement Among Paramedics N = 155 Kappa = 0.93 (0.87 – 0.99) Conservatively misinterpreted the rule N = 320 (16%) Dangerous mechanism overcalled N = 154 (8%) Did not rotate the neck when indicated N = 166 (9%)
 Conservatively misinterpreted the rule N = 320 (16%) Dangerous mechanism overcalled N = 154 (8%) Did not rotate the neck when indicated N = 166 (9%)")
35
How Comfortable… N= 1,947

36
Phase III …Started 1/11 th /2011! Evaluation of the Safety of C-Spine Clearance by Paramedics

38
Why not implement this province wide right away?? We could not convince people this was a safe thing to do…yet!

39
Others are doing it! NEXUS rule used in USA Domeier, Ann Arbor MI Missed 33 of 415 injuries (8%) Stroh, Fresno CA Missed 5 of 504 injuries (1%) 2 were clinically important 1 resulted in adverse outcome Canadian C-Spine rule is used in few cities in Canada, but miss rate is not reported Canadian C-Spine rule is better than NEXUS
 Stroh, Fresno CA Missed 5 of 504 injuries (1%) 2 were clinically important 1 resulted in adverse outcome Canadian C-Spine rule is used in few cities in Canada, but miss rate is not reported Canadian C-Spine rule is better than NEXUS.")
40
2003

41
Sensitivity 100% (95% CI 74% to 100%) Percentage of Eligible Trauma Victims Enrolled per Month Over a One Year Period (N=1,236)
 Percentage of Eligible Trauma Victims Enrolled per Month Over a One Year Period (N=1,236)")
42
We need to evaluate more patients in this ongoing study such that we can decrease this margin of error down to a level acceptable to all partners

43
First, answer the questions on top… Easy if not for spine injury

44
The Canadian C-Spine Rule

46
High-Risk Factors Age 65

47
High-Risk Factors Paresthesias in Extremities

48
The Canadian C-Spine Rule

49
High-Risk Factors Dangerous Mechanism

50
The Canadian C-Spine Rule

51
Low-Risk Factors

52
The Canadian C-Spine Rule

53
Simple Rear-end Excludes…

54
The Canadian C-Spine Rule

55
Ability to Rotate the Neck

56
Do not forget the last questions at the bottom…

57
Let’s do this again… 1.Should I use the rule for this patient 2.Is there any of the High-Risk factor 3.Is there at least one of the Low-Risk factor 4.Can the patient rotate 45 degree on own 5.Do I agree with the rule’s recommendation?

58
Should I use the rule in this patient? Recent ( 16 yo Normal GCS Normal neuro exam Normal vitals Normal spine in the past Normal everything!

59
Our overall goal We want to recruit 3,000 patients by the end of this year 20 of those patients are expected to have a clinically important c-spine injury We intend to apply to renew funding this September for a multi-center implementation study

60
Now on to the next topic…

62
Objectives 1. Review current statistics for prehospital cardiac arrest care and survival 2. Illustrate the importance of agonal breathing for prehospital cardiac arrest recognition 3. Demonstrate current efforts to improve bystander CPR rates in the community

63
20,000 victims per year

65
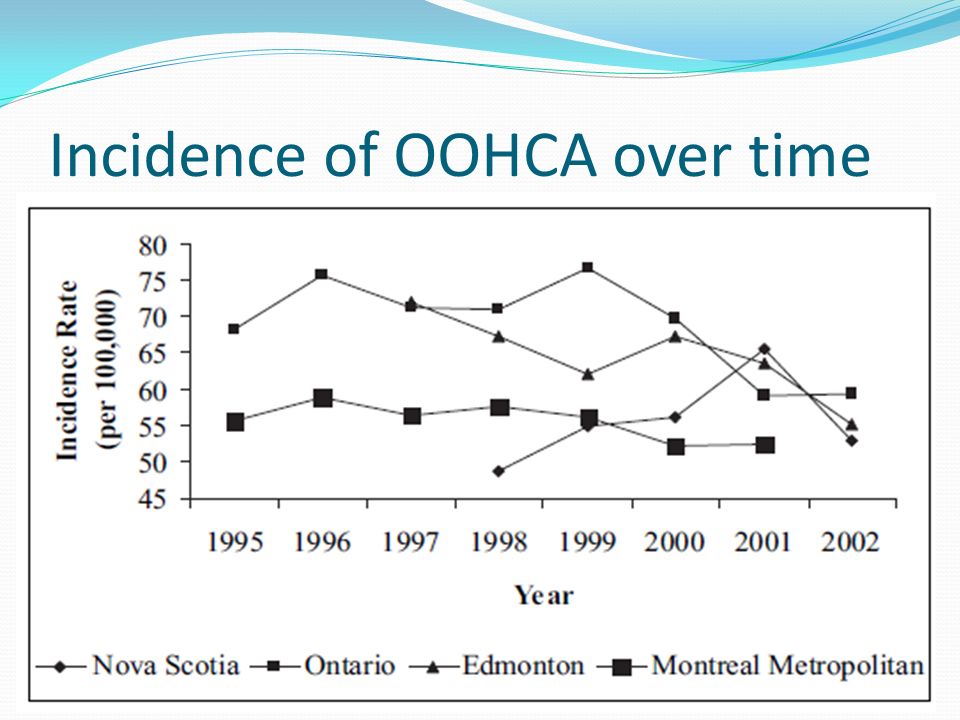
Incidence of OOHCA over time

66
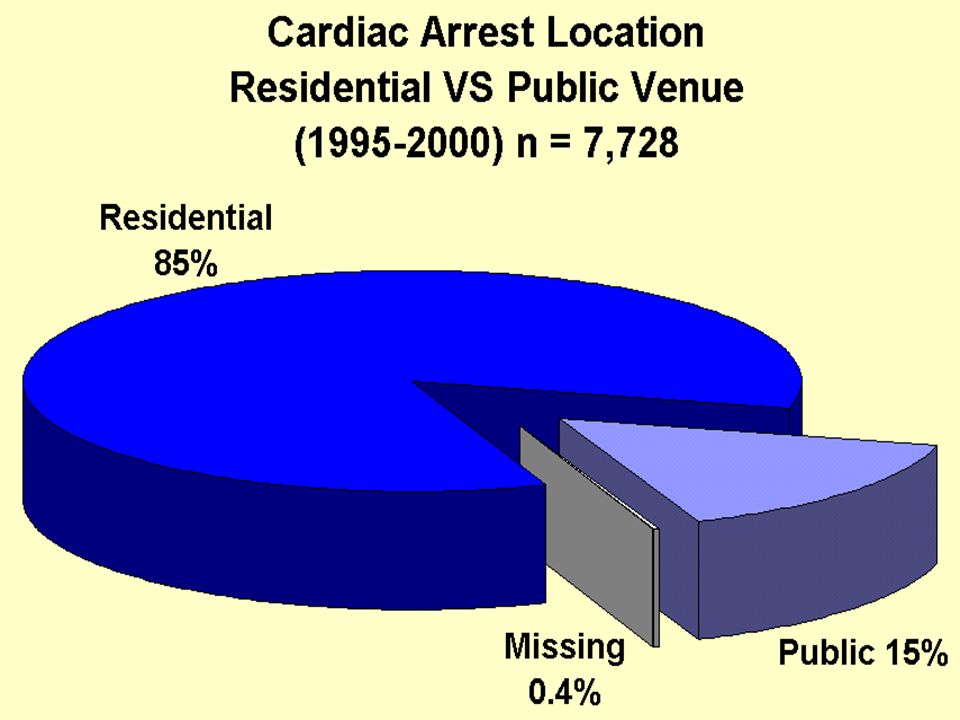
Cardiac arrest statistics… Mean age is 69 67% are men 50% are witnessed 1 st symptom of cardiac disease in 50%

69
What can we do about it?

71
3 -4 times more likely to survive

72
Effect of bystander CPR… 32% 46% 15%

73
Bystander CPR over time…

74
Reviewed 252 publications on CPR CJEM 2008;10(1):51-65
:51-65")
75
Best approaches…

76
Dispatch-assisted CPR instructions Started April, 2004 in Ontario Intervention

77
Bystander CPR rate today

78
Effect on survival rates

79
Current Statistics… Bystander CPR rate between 20% to 30% Overall survival rate between 6% to 9%

80
CAEP 2011, St. John’s

81
Cardiac ArrestNo Cardiac Arrest Diagnosis1,012490 No Diagnosis524234 %95% CI Sensitivity65.963.5 – 68.2 Specificity32.329.0 – 35.9 PPV67.4 NPV30.9

82
Callers (%) Female 60.0 Relationship to the victim Spouse27.8 Child17.5 Nursing home staff 7.1 Stranger 6.9 Friend 6.3 Previously trained in CPR (n = 475)40.6 Reported agonal breathing 22.7
 Female 60.0 Relationship to the victim Spouse27.8 Child17.5 Nursing home staff 7.1 Stranger 6.9 Friend 6.3 Previously trained in CPR (n = 475)40.6 Reported agonal breathing 22.7")
85
Factors Associated With the Successful Recognition of Agonal Breathing and Cardiac Arrest by Ambulance Communications Officers CAEP 2010 and 2011

86
Methods Interview guide: Based on the constructs of the Theory of Planned Behaviour

87
Improving the Cardiac Arrest Diagnostic Accuracy of 9-1-1 Communication Officers Study launched this week!

88
Controlled before-after ; time series analyses Ottawa compared to Windsor (control) 700 cardiac arrest recordings per group over next 3 years
 700 cardiac arrest recordings per group over next 3 years")
89
Increase cardiac arrest recognition by 10%, from 65% to 75% Increase bystander CPR rates from 30% to 40% Save the lives of 100 additional Ontarians/year

90
To review current immobilization practices To describe the derivation and validation of the Canadian C-Spine Rule To illustrate its application by paramedics in the field

91
Review current statistics for prehospital cardiac arrest care and survival Illustrate the importance of agonal breathing for prehospital cardiac arrest recognition Demonstrate current efforts to improve bystander CPR rates in the community

92
Time for Questions!

Similar presentations



>")











 By Primary Care Paramedics Implementation Trial Research by Ontario’s Base Hospitals in Collaboration with the Sunnybrook.>")

>")




