Download presentation
Presentation is loading. Please wait.

1
Spinal Cord lesions

2
DEFINITION Insult to spinal cord resulting in a change, in the normal motor, sensory or autonomic function. This change is either temporary or permanent.

3
Anatomy Spinal cord lies within protective covering of vertebral column. Begins just below foramen magnum of the skull. Ends opposite 2nd lumbar vertebra. Below L2 continue as a leash of nerve roots known as cauda equina. Prolongation of the pia matter forms filum terminale

4
Hence: 31 pairs of spinal nerves:
8 cervical 12 thoracic 5 lumbar 5 sacral 1 coccygeal

5
Spinal cord structure

6
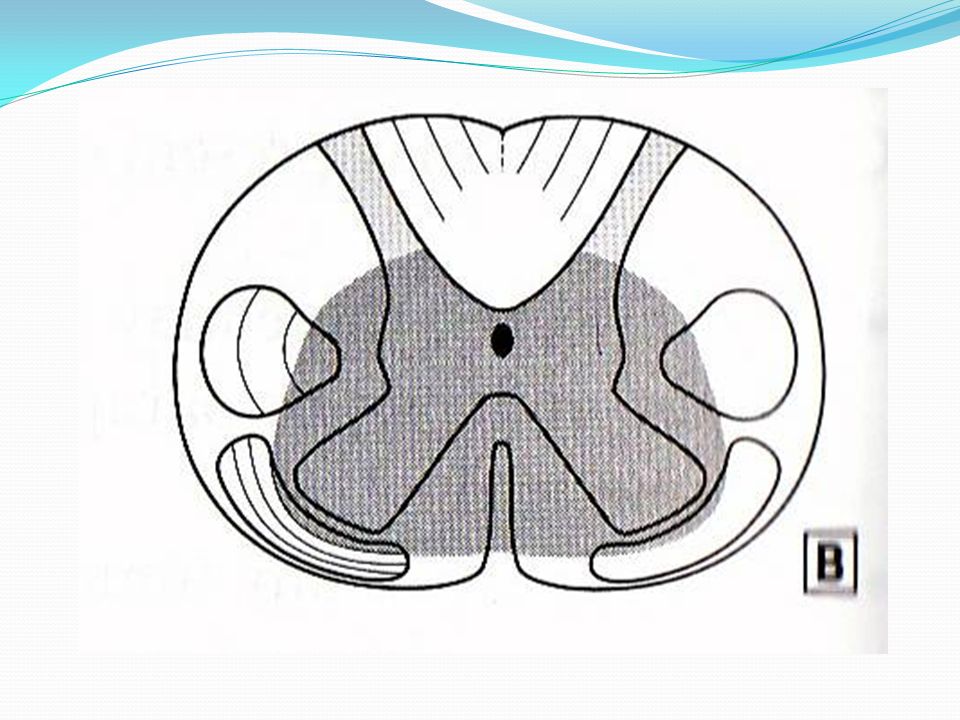
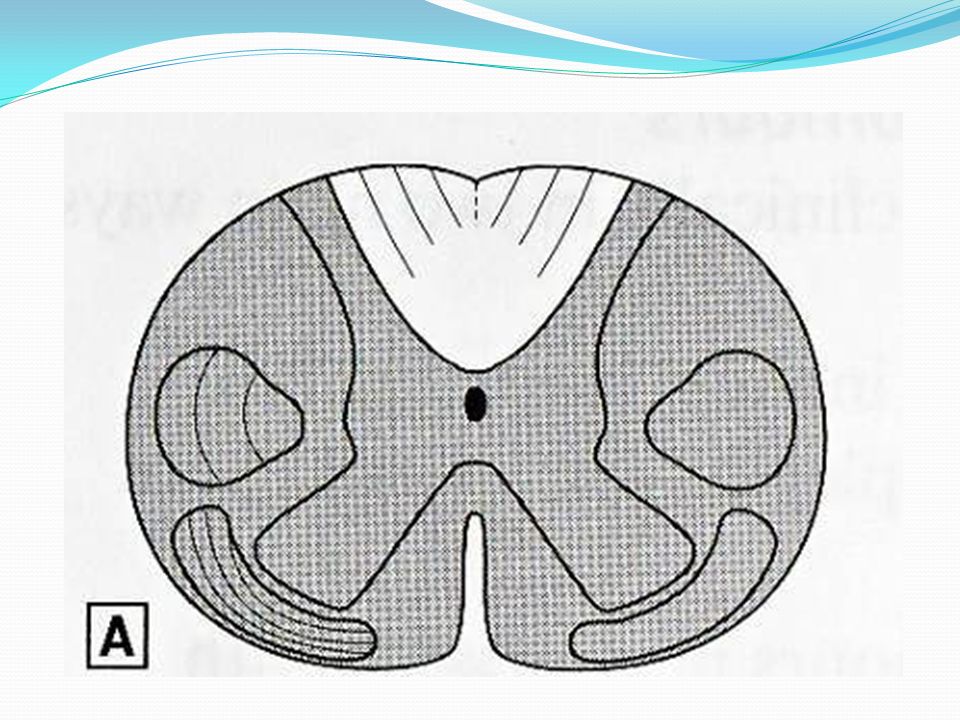
Spinal cord structure The spinal cord consists of central core of grey matter containing nerve cell bodies, and outer layer of white matter of nerve fibers. Within the grey matter, the dorsal horn contains sensory neurons, the ventral horn contains motor neurons and the lateral horn contains preganglionic sympathetic neurons. Within the white matter run ascending and descending nerve fiber tracts, which link the spinal cord to the brain.

7
The principle ascending tracts are the spinothalamic tracts, spinocerebellar tracts and dorsal columns. The coticospinal tracts is an important descending tract. The spinal cord receives information from, and controls the trunk and limbs. This is achieved through 31 pairs of spinal nerves which join the cord at intervals along its length and contain afferent and efferent nerve fibers connecting with the structures at the periphery.

8
Spinal cord compression

9
Statistics National Spinal Cord Injury Database { USA Stats }
MVA % Falls % Violence % Sports % 55% cases occur in 16 – 30yrs of age 81.6% are male!

10
Physiology and function
Grey matter – sensory and motor nerve cells White matter – ascending and descending tracts Divided into - dorsal - lateral - ventral

11
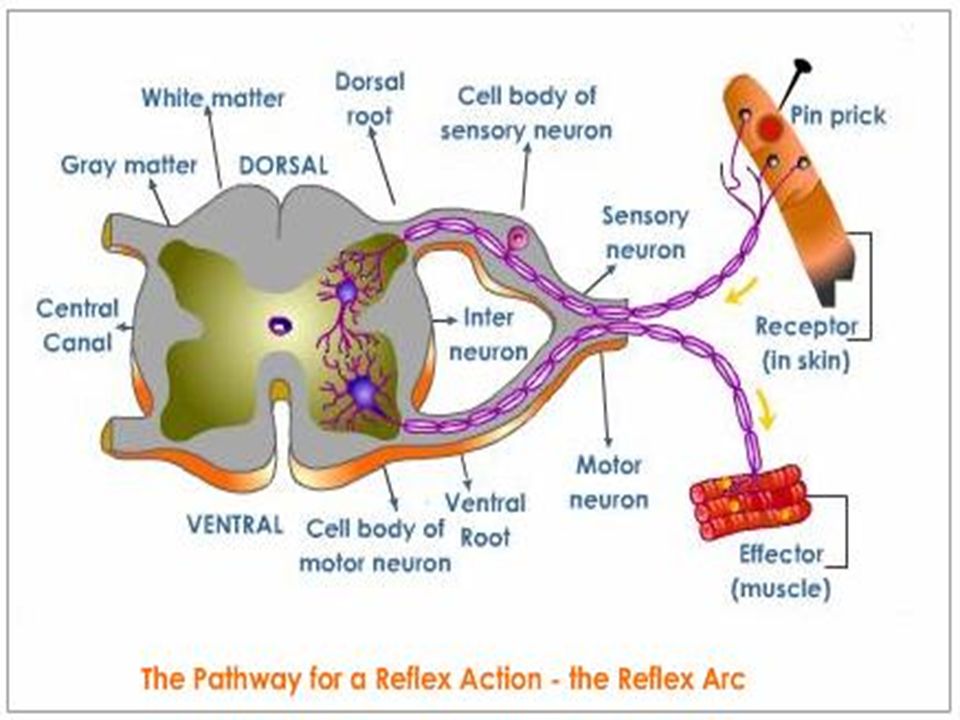
Normal Spinal Cord Reflex Arc Involuntary response to a stimulus
Where sensory and motor nerves arise from cord Sensory fibers enter posterior Synapse in the grey matter Motor fibers leave anterior Once outside cord join form spinal nerve

13
Spinal Cord Protection
Bones- vertebral column 7 Cervical 12 Thoracic 5- Lumbar 5- Sacral Discs- between vertebra

14
Tracts : 1) Posterior column: Fine touch Light press Proprioception
2) Lateral corticospinal tract : Skilled voluntary movement 3) Lateral spinothalamic tract : Pain & temperature sensation
 Lateral corticospinal tract : Skilled voluntary movement. 3) Lateral spinothalamic tract : Pain & temperature sensation.")
15
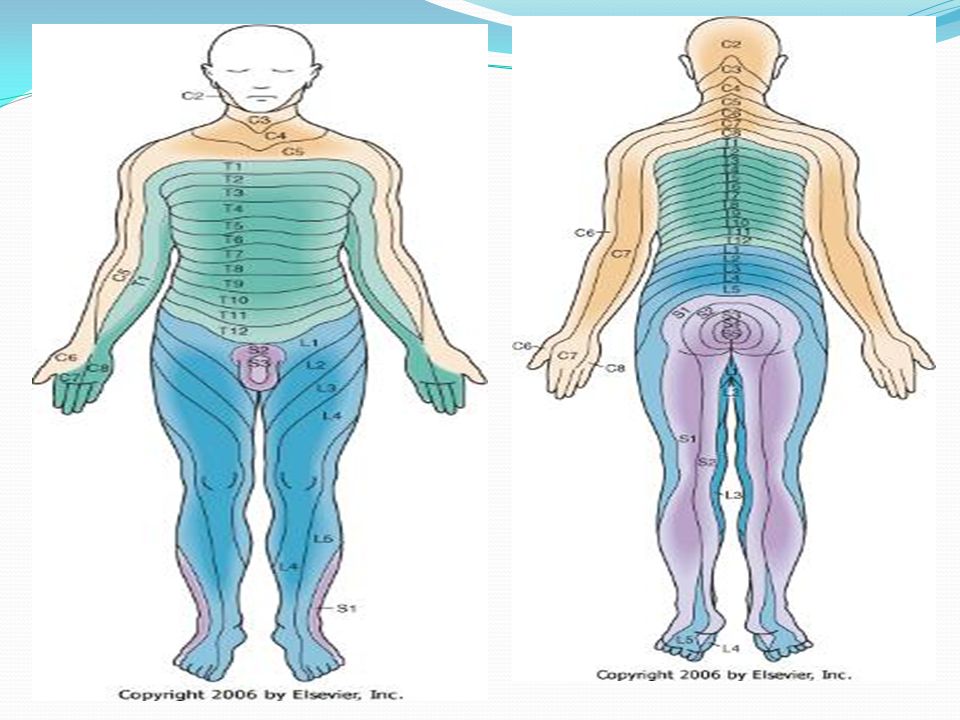
Dermatomes Area of skin innervated by sensory axons within a particular segmental nerve root Knowledge is essential in determining level of injury Useful in assessing improvement or deterioration

17
Myotomes Segmental nerve root innervating a muscle
Again important in determining level of injury Upper limbs: C5 - Deltoid C 6 - Wrist extensors C 7 - Elbow extensors C Long finger flexors T Small hand muscles Lower Limbs : L Hip flexors L3,4 - Knee extensors L4,5 – S1 - Knee flexion L5 - Ankle dorsiflexion S1 - Ankle plantar flexion

18
Spinal Cord Injury Primary Secondary Ischemia Hypoxia Microhemorrhage
Initial mechanism of injury Secondary Ongoing progressive damage Ischemia Hypoxia Microhemorrhage Edema

19
Mechanism of Injury Flexion Hyperextension Compression
Flexion /Rotation

20
Flexion (hyper flexion)
Most common because of natural protection position. Generally cause neck to be unstable because stretching of ligaments

21
Hyperextension Caused by chin hitting a surface area, such as dashboard or bathtub Usually causes central cord syndrome symptom

22
Hyperextension

23
Compression Caused by force from above, as hit on head
Or from below as landing on butt Usually affects the lumbar region

24
Flexion/Rotation Most unstable
Results in tearing of ligamentous structures that normally stabilize the spine Usually results in serious neurologic deficits

25
Classifications of SCI Completeness (Degree) of Injury
Incomplete Central cord syndrome Anterior Cord syndrome Brown-Sequard Syndrome Posterior Cord Syndrome Cauda Equina and Conus Medullaris

26
Complete Motor deficits- Sensory- Autonomic deficits-
Loss of voluntary movement of parts innervated by segment, this is irreversible Loss of sensation Spinal shock Motor deficits- spastic paralysis below level of injury Sensory- loss of all sensation perception Autonomic deficits- vasomotor failure and spastic bladder

27
Incomplete: Some function is present below site of injury
More favourable prognosis overall Are recognizable patterns of injury, although they are rarely pure and variations occur

28
Central cord syndrome Injury to the center of the cord by edema and hemorrhage Motor weakness and sensory loss in all extremities Upper extremities affected more

30
Anterior cord Syndrome:
Injury to anterior cord Loss of voluntary motor, pain and temperature perception below injury Retains posterior column function (sensations of touch, position, vibration, motion)
")
32
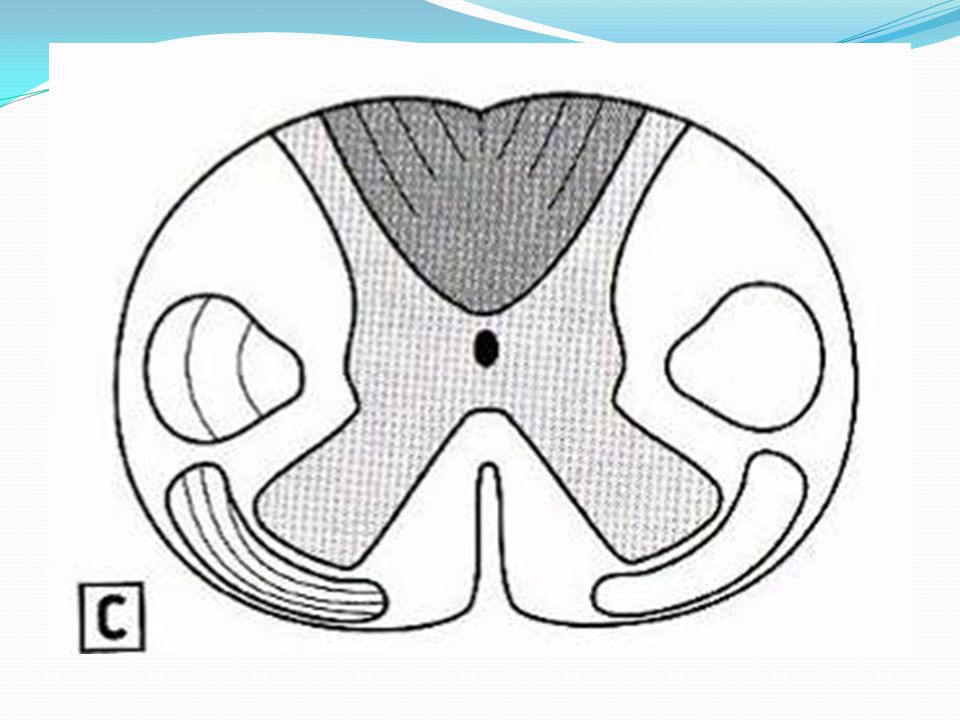
Posterior Cord Syndrome
Least frequent syndrome Injury to the posterior (dorsal) columns Loss of proprioception Pain, temperature, sensation and motor function below the level of the lesion remain intact Proprioception affected – ataxia and faltering gait Usually good power and sensation
 columns. Loss of proprioception. Pain, temperature, sensation and motor function below the level of the lesion remain intact. Proprioception affected – ataxia and faltering gait. Usually good power and sensation.")
34
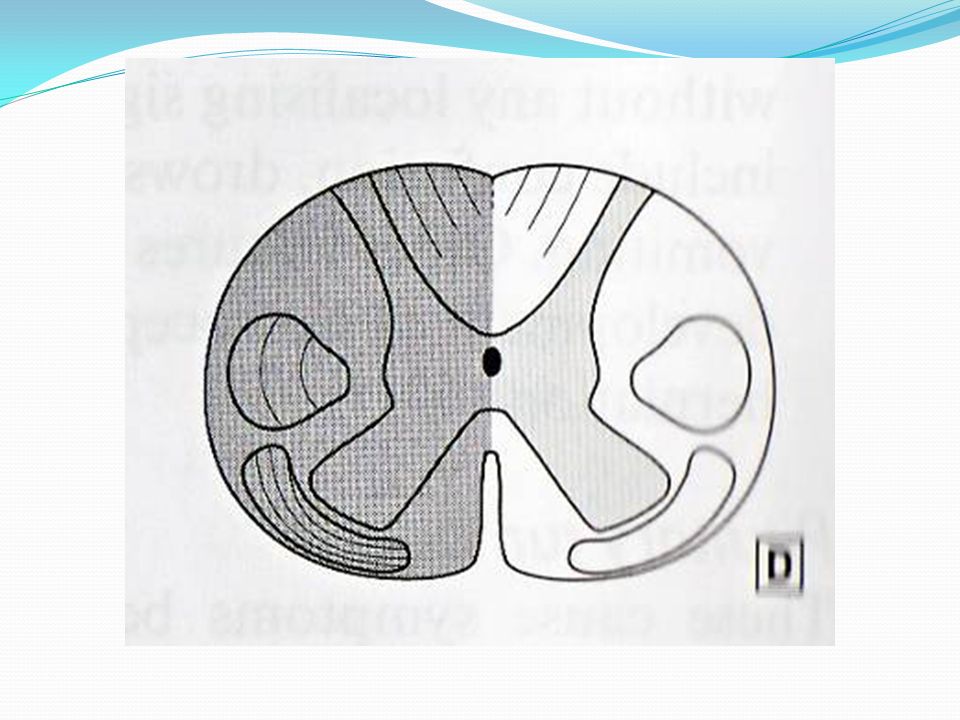
Brown – Sequard Syndrome:
Hemisection of cord Ipsilateral paralysis Ipsilateral superficial sensation, vibration and proprioception loss Contralateral loss of pain and temperature perception

36
Cauda Equina and Conus Medullaris
Injury to the sacral cord (conus) and lumbar nerve roots Cauda Equina Injury to the lumbosacral nerve roots Result- areflexic (flaccid)bladder and bowel, flaccid lower limbs
 and lumbar nerve roots. Cauda Equina. Injury to the lumbosacral nerve roots. Result- areflexic (flaccid)bladder and bowel, flaccid lower limbs.")
37
Cervical injuries - When spinal cord injuries occur near the neck, symptoms can affect both the arms and the legs: Breathing difficulties (from paralysis of the breathing muscles). Loss of normal bowel and bladder control (may include constipation, incontinence, bladder spasms). Numbness. Sensory changes. Spasticity (increased muscle tone). Pain. Weakness, paralysis.
. Loss of normal bowel and bladder control (may include constipation, incontinence, bladder spasms). Numbness. Sensory changes. Spasticity (increased muscle tone). Pain. Weakness, paralysis.")
38
Thoracic injuries When spinal injuries occur at chest level, symptoms can affect the legs: Breathing difficulties (from paralysis of the breathing muscles) Loss of normal bowel and bladder control (may include constipation, incontinence, bladder spasms). Numbness. Sensory changes. Spasticity (increased muscle tone). Pain. Weakness, paralysis. Injuries to the cervical or high-thoracic spinal cord may also result in blood pressure problems, abnormal sweating, and trouble maintaining normal body temperature
 Loss of normal bowel and bladder control (may include constipation, incontinence, bladder spasms). Numbness. Sensory changes. Spasticity (increased muscle tone). Pain. Weakness, paralysis. Injuries to the cervical or high-thoracic spinal cord may also result in blood pressure problems, abnormal sweating, and trouble maintaining normal body temperature.")
39
Lumbosacral injuries When spinal injuries occur at the lower-back level, varying degrees of symptoms can affect the legs: Loss of normal bowel and bladder control (may include constipation, incontinence, bladder spasms). Numbness. Pain. Sensory changes. Spasticity (increased muscle tone). Weakness and paralysis
. Numbness. Pain. Sensory changes. Spasticity (increased muscle tone). Weakness and paralysis.")
40
Types of Spinal Cord Paralysis
Depending on the location and the extent of the injury different forms of paralysis can occur. Monoplegia- paralysis of one limb Diplegia- paralysis of both upper or lower limbs Paraplegia- paralysis of both lower limbs Hemiplegic- paralysis of upper limb, torso and lower leg on one side of the body Quadriplegia- paralysis of all four limbs

41
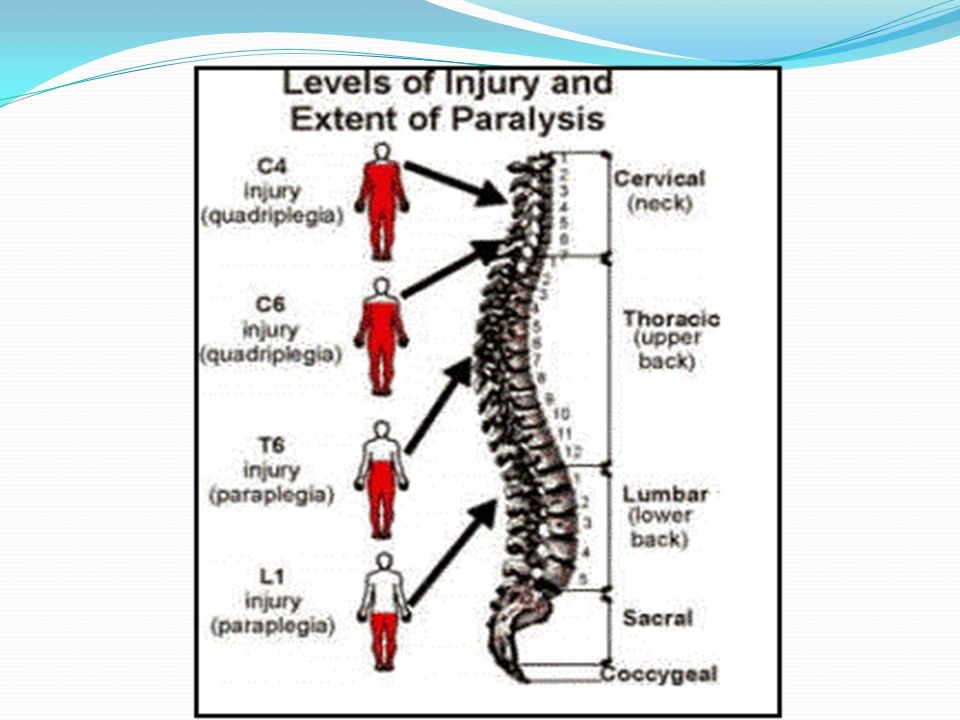
Spinal Cord Paralysis Levels
C1-C3 All daily functions must be totally assisted Breathing is dependant on a ventilator Motorised wheelchair controlled by sip and puff or chin movements is required C4 Same as C1-C3 except breathing can be done without a ventilator C5 Good head, neck, shoulder movements, as well as elbow flexion Electric wheelchair, or manual for short distances

43
C6 Wrist extension movements are good Assistance needed for dressing, and transitions from bed to chair and car may also need assistance C7-C8 All hand movements Ability to dress, eat, drive, do transfers, and do upper body washes

44
T1-T4 (paraplegia) Normal communication skills Help may only be needed for heavy household work or loading wheelchair into car T5-T9 Manual wheelchair for everyday living Independent for personal care T10-L1 Partial paralysis of lower body L2-S5 Some knee, hip and foot movements with possible slow difficult walking with assistance or aids Only heavy home maintenance and hard cleaning will need assistance

46
Injury defined by ASIA Impairment Scale
ASIA – American Spinal Injury Association : A – Complete: no sensory or motor function preserved in sacral segments S4 – S5 B – Incomplete: sensory, but no motor function in sacral segments

47
ASIA – American Spinal Injury Association
C – Incomplete: motor function preserved below level and power graded < 3 D – Incomplete: motor function preserved below level and power graded 3 or more E – Normal: sensory and motor function normal

48
Investigation X ray. CT scan. MRI. Myelogram. Biopsy. Bone scan.
Blood and spinal fluid studies.

49
Muscle Strength Grading:
5 – Normal strength 4 – Full range of motion, but less than normal strength against resistance 3 – Full range of motion against gravity 2 – Movement with gravity eliminated 1 – Flicker of movement 0 – Total paralysis

50
Therapeutic Interventions
Stabilization/ Immobilization Traction- Gardner-wells tongs Halo Casts Splints Collars Braces

51
Management of Spinal Cord Injuries
Immediate management at the scene is critical. Improper handling can cause further damage and loss of functioning Always assume there is a spinal cord injury until it is ruled out Immobilize Prevent flexion, rotation or extension of neck Avoid twisting patient If conscious, patients will usually mention acute pain in back or neck which may radiate along the involved nerve

52
Management of Spinal Cord Injuries
Consists of emergency treatment following an A-B-C-D-E sequence. Airway Management Use bag-valve-mask devise initially for airway compromise and if necessary to prepare for intubation. Breathing Circulation Disability Exposure

53
Breathing Lesions above C5 level will cause partial to complete diaphragmatic paralysis (recall the diaphragm is innervated at C3-5 levels). Any lesion above T12 may cause some airway compromise. Lesions at C5 and below will allow full diaphragmatic movement, but intercostal muscles (innervated at T1) and abdominal muscles (innervated at T12) are affected
 and abdominal muscles (innervated at T12) are affected.")
54
Circulation Cardiac output is affected by external or internal hemorrhage. To determine external bleeding, turn the patient in log-roll fashion and quickly note the site of injury. Two signs of internal bleeding from abdominal trauma are abdominal pain and muscular rigidity. However, these signs may be masked in a patient with sensory and motor deficits.

55
Exposure Patients with SCI become poikilothermic, meaning that their body temperature will increase and decrease with the temperature of the environment. Because they lose the ability to regulate core body temperature through vasodilatation and vasoconstriction, they can become dangerously hyperthermic or hypothermic.

56
Neurological/Orthopedic Management
Reduction Fixation Fusion Fixation involves stabilizing vertebral fractures with wires, plates, and other types of hardware.

57
Rehab and Long-Term Issues
Mobility - initially may require a brace or halo. Needs to bear weight as soon as possible because it helps decrease disuse atrophy, decrease the opportunity for osteoporosis, decrease the possibility of renal calculi, and enhances metabolic processes self-care Skin Integrity - needs to be taught the importance of being responsible for own skin integrity Exercise - to strengthen unaffected parts and promote

58
Bed mobility Pressure relief Wheel chair transfer
Prevent and Manage Complications Spastic Muscles - maximum spastic activity is usually 2 years out and then minimizes some. May require long-term use of anti-spasmodic drugs such as valium, baclofen or dantrium. Contractures - Needs to understand the importance of exercise and maintaining function Bed mobility Pressure relief Wheel chair transfer

Similar presentations













 and Nerves. NERVOUS SYSTEM 1.Collect sensory input 2.Integrate sensory input 3.Motor output Functions of Nervous System.>")






