Download presentation
Presentation is loading. Please wait.

1
Kim Bandelier, MPH, RD, LD Susan Roberts, MS, RDN, LD, CNSC

2
Kim Bandelier: Susan Roberts: Vice-Chair of Academy Council on Future Practice

3
Articulate the current status of order writing privileges for licensed dietitians in Texas in acute care and long term care Describe challenges in obtaining RDN order writing privileges Identify important considerations with order writing and ways to demonstrate positive patient outcomes

4
Texas Licensure: 711.1(13): "Dietetics--The professional discipline of applying and integrating scientific principles of food, nutrition, biochemistry, physiology, management, and behavioral and social sciences under different health, social, cultural, physical, psychological, and economic conditions to the proper nourishment, care, and education of individuals or groups throughout the life cycle to achieve and maintain the health of people. The term includes, without limitation, the development, management, and provision of nutrition services.“ 711((19): "Nutrition assessment--The evaluation of the nutritional needs of individuals and groups based on appropriate biochemical, anthropometric, physical, and dietary data to determine nutrient needs and recommend appropriate nutritional intake including enteral and parenteral nutrition. An important component of medical nutrition therapy.“
: Nutrition assessment--The evaluation of the nutritional needs of individuals and groups based on appropriate biochemical, anthropometric, physical, and dietary data to determine nutrient needs and recommend appropriate nutritional intake including enteral and parenteral nutrition. An important component of medical nutrition therapy. .")
5
711.4(b): (1) "A licensed dietitian, acting within the scope of his or her license and consistent with medical direction or authorization as provided in this section, may accept, transcribe into a patient's medical record or transmit verbal or electronically- transmitted orders, including medication orders, from a physician to other authorized health care professionals relating to the implementation or provision of medical nutrition therapy and related medical protocols for an individual patient or group of patients. In a licensed health facility, the medical direction or authorization shall be provided, as appropriate, through a physician's order, or a standing medical order, or standing delegation order, or medical protocol issued in accordance with Texas Occupations Code, Chapter 157, Subchapter A, and rules adopted by the Board of Medical Examiners implementing the subchapter. In a private practice setting, the medical direction or authorization shall be provided, as appropriate, through the physician's order, standing medical order, or standing delegation order of a referring physician, in accordance with Texas Occupations Code, Chapter 157, Subchapter A, and rules adopted by the Board of Medical Examiners implementing the subchapter.

6
(2) A licensed dietitian, acting within the scope of his or her license and consistent with medical direction or authorization as provided in this section, may order medical laboratory tests relating to the implementation or provision of medical nutrition therapy and related medical protocols for individual patients or groups of patients. In a licensed health facility, the medical direction or authorization shall be provided, as appropriate, through a physician's order, or a standing medical order, or standing delegation order, or medical protocol, issued in accordance with Texas Occupations Code, Chapter 157, Subchapter A, and rules adopted by the Board of Medical Examiners implementing the subchapter. In a private practice setting, the medical direction or authorization shall be provided through the physician's order, standing medical order, or a standing delegation order of the referring physician, in accordance with Texas Occupations Code, Chapter 157, Subchapter A, and rules adopted by the Board of Medical Examiners implementing the subchapter."

7
Allows for order writing via protocols, delegation of order writing by physician to LD Allows for ordering labs Probably a good idea to clean up the language to make consistent with new CoPs, but not prohibitive

8
Hospital Regulations: Rule §133.2(15): "Dietitian--A person who is currently licensed by the Texas State Board of Examiners of Dietitians as a licensed dietitian or provisional licensed dietitian, or who is a registered dietitian with the American Dietetic Association." Rule §133.41(1)(d)(B): "There shall be a qualified dietitian who works full-time, part-time, or on a consultant basis. If by consultation, such services shall occur at least once per month for not less than eight hours. The dietitian shall: (i) be currently licensed under the laws of this state to use the titles of licensed dietitian or provisional licensed dietitian, or be a registered dietitian;... (iii) supervise the nutritional aspects of patient care; (iv) make an assessment of the nutritional status and adequacy of nutritional regimen, as appropriate;... (vi) document nutritional status and pertinent information in patient medical records, as appropriate;" Rule §133.41(3)(A): "Therapeutic diets shall be prescribed by the physician(s) responsible for the care of the patients." Rule §133.41(3)(B): "Nutritional needs shall be met in accordance with recognized dietary practices and in accordance with orders of the physician(s) or appropriately credentialed practitioner(s) responsible for the care of the patients."
 be currently licensed under the laws of this state to use the titles of licensed dietitian or provisional licensed dietitian, or be a registered dietitian;... (iii) supervise the nutritional aspects of patient care; (iv) make an assessment of the nutritional status and adequacy of nutritional regimen, as appropriate;... (vi) document nutritional status and pertinent information in patient medical records, as appropriate; Rule §133.41(3)(A): Therapeutic diets shall be prescribed by the physician(s) responsible for the care of the patients. Rule §133.41(3)(B): Nutritional needs shall be met in accordance with recognized dietary practices and in accordance with orders of the physician(s) or appropriately credentialed practitioner(s) responsible for the care of the patients. .")
9
Texas PPP met with Academy lawyer and Texas Academy Lobbyist to develop plan Licensure could be tweaked but main issue is language in Hospital Licensing regulations. Consumer Protection Coordinator worked with Texas State Board of Examiners of Dietitians (TSBED) TSBED does not see licensure as issue; nor do they feel this is within their scope/jurisdiction
 TSBED does not see licensure as issue; nor do they feel this is within their scope/jurisdiction.")
10
84 th Texas Legislature in Session Consumes state agencies time and resources Sunset Commission and Saving our Licensure Texas PPP meets with DSHS Health Facilities Rule Coordinator

11
Patient by patient order writing delegation Work with stakeholders within your hospital Physicians, nursing, IT, quality director, risk management Draft a policy that clearly spells out what orders you can write Good example located at http://www.nutrition411.com/content/order-writing- privileges-registered-dietitians-medical-nutrition-therapy http://www.nutrition411.com/content/order-writing- privileges-registered-dietitians-medical-nutrition-therapy Get policy approved by appropriate committees Most often P&T and Med Exec

12
How have you been granted Ordering Privileges in your current hospital or critical access hospital? a) Appointed to medical staff through credentialing process and have autonomous ordering privileges b) Appointed to medical staff through other facility process (i.e. HR) and have autonomous ordering privileges c) Delegated orders as written by medical staff to allow RDN to write orders d) Defer and consult with medical staff responsible for patient
 Appointed to medical staff through credentialing process and have autonomous ordering privileges b) Appointed to medical staff through other facility process (i.e. HR) and have autonomous ordering privileges c) Delegated orders as written by medical staff to allow RDN to write orders d) Defer and consult with medical staff responsible for patient.")
13
Assist RDNs in reviewing the Final Rule’s purpose and implementing steps for dietetics practice Practice Tips: Hospital Regulation- Ordering Privileges for the RDN Practice Tips: Implementation Steps- Ordering Privileges for the RDN www.eatrightpro.org/dietorders

14
In states where State law or regulations limits appointments to certain categories of practitioners, privileges may still be granted without appointment to the medical staff as long as such privileges are: Recommended by the medical staff Approved by the governing body Are in accordance with State law The hospital and its medical staff are best qualified and are best situated to exercise oversight, such as credentialing and competency review, of those practitioners to whom it grants privileges, just as it would for those practitioners appointed to its medical staff.

15
Creates savings and reduces burden in many areas. Creates measurable monetary savings for providers and suppliers, while others create savings of time and administrative burden. Proposed regulatory changes allows hospitals to grant appropriate ordering privileges to RDs Hospitals would not be able to effectively realize improved patient outcomes and overall cost savings The economic impact estimate for hospitals is $459 million reoccurring annually.

16
Early nutritional intervention is key to prevention and treatment of malnutrition Only 42% of 865 written RDN recommendations were implemented by MDs in one study 1 Research demonstrates improved outcomes when RDN recommendations are followed 2-5 Timely implementation of Medical Nutrition Therapy is often delayed due to: 5,6 Communication delays between RDN & physician Overlooked recommendations 1)Skipper et al. 1994, JADA 2)Weddel et al. 1995, JADA 3)Braga et al. 2006, JADA 4)Lee et al. 2012, Clin Biochem 5) Moreland et al. 2002, JADA 6) Silver et al. 2003, JADA
Weddel et al. 1995, JADA 3)Braga et al. 2006, JADA 4)Lee et al. 2012, Clin Biochem 5) Moreland et al. 2002, JADA 6) Silver et al. 2003, JADA.")
17
Problems: Patient delayed in receiving care; time constraints of all staff; wasting time of staff; notes get lost or missed; RN forgets to call; MD forgets to write order Independent or Delegated Nutrition Orders by RD from Moreland et al 5

19
Long history of verbal orders- “just write it for me” From first attempts to obtain order writing privileges to implementation took ~4 years

20
Long history of informal privileges writing nutrition-related orders using verbal order process Why change? CMS emphasis that verbal orders are only for emergency situations, not routine use Joint Commission has guidelines for appropriate use of verbal orders consistent with CMS Conditions of Participations Issues arise when physicians and nurses assume all staff are competent to write orders Liability for staff, MD, and hospital

21
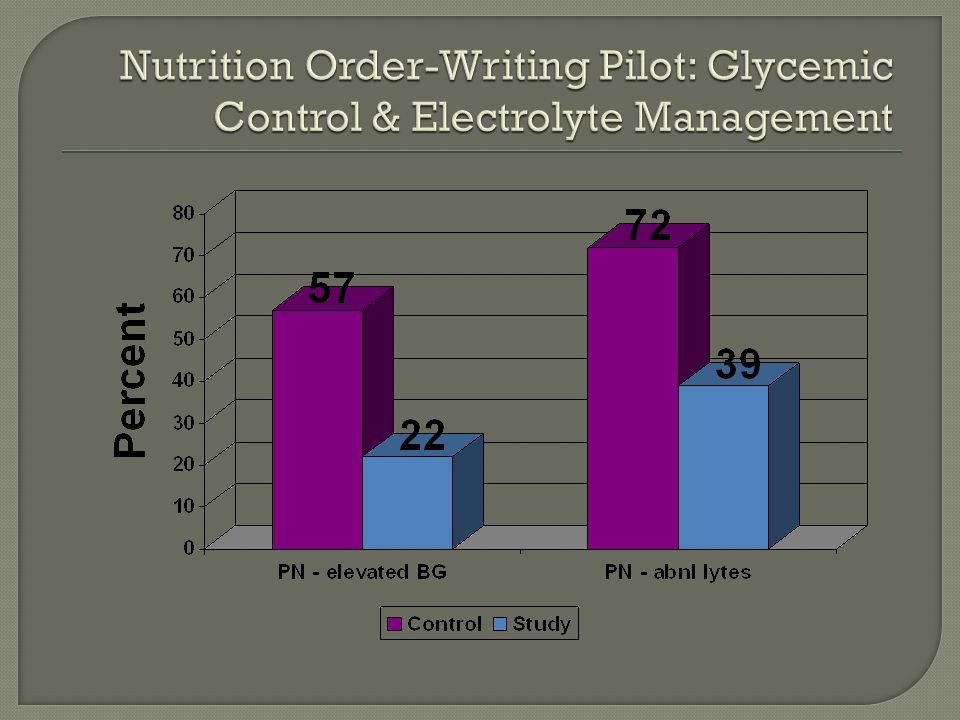
Parenteral Nutrition order-writing audit (2003 & 2004) Sample size= 50 (in 2 years) Average # of days on PN= 12 days ~30% of PN orders had RDN involved with writing orders exclusively or part of the time Results showed RDN involvement with order writing led to improved electrolyte management and glucose control Information presented at Medical Nutrition Committee after both audits, but unable to obtain approval for RDN order writing protocol
 Sample size= 50 (in 2 years) Average # of days on PN= 12 days ~30% of PN orders had RDN involved with writing orders exclusively or part of the time Results showed RDN involvement with order writing led to improved electrolyte management and glucose control Information presented at Medical Nutrition Committee after both audits, but unable to obtain approval for RDN order writing protocol")
22
June 2006: Reintroduced the ideas of RDNs having nutrition order-writing privileges to Medical Nutrition Committee Pilot study on a general medicine and a surgical unit for 2 months First month-usual care Second month- RDN management of nutrition orders Utilized RDNs with ~5 years of experience + CNSD

23
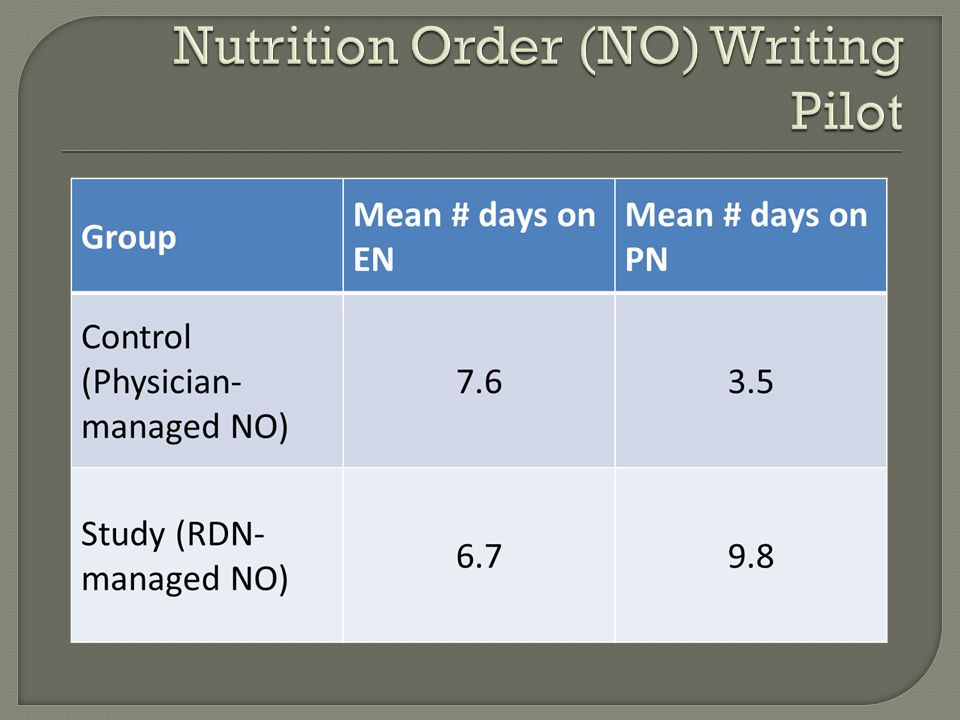
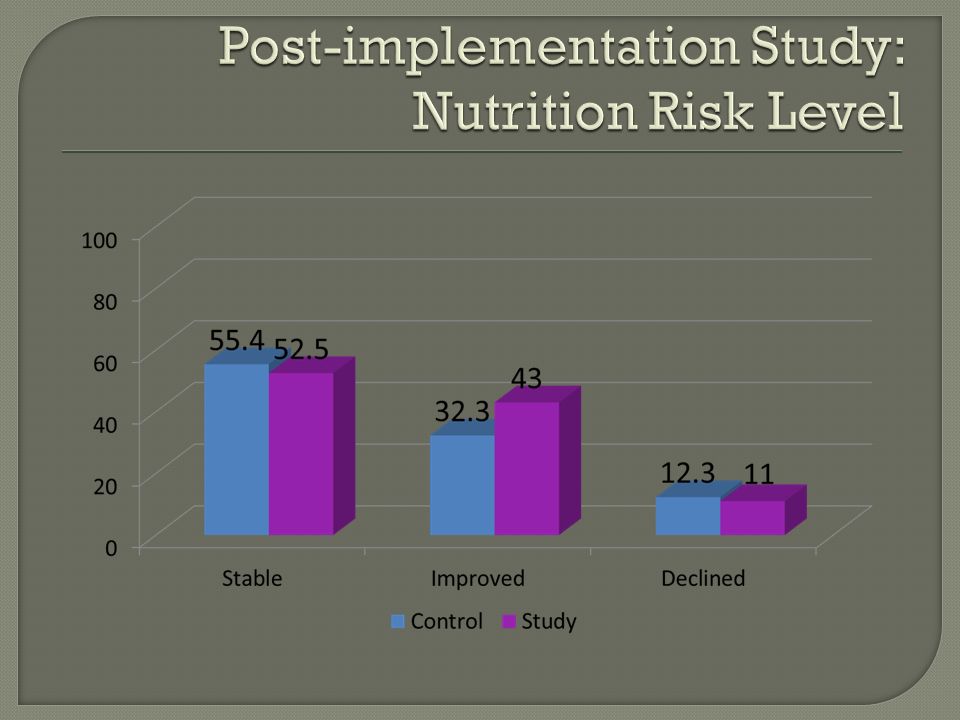
Objective: To demonstrate RDs’ ability to provide safe, effective care through independent nutrition-order (NO) writing privileges Prospective data on total of 190 patients Control group (Physician-managed NO): N=97, RD assessment/recommendations documented and communicated as needed Study group (RD-managed NO): N=93, RD managed nutrition orders with automatic RD assessment
 writing privileges Prospective data on total of 190 patients Control group (Physician-managed NO): N=97, RD assessment/recommendations documented and communicated as needed Study group (RD-managed NO): N=93, RD managed nutrition orders with automatic RD assessment")
24
Procedure for Study Group: MD orders “Nutrition Management Consult” MD still maintains direct control of patient care MD may discontinue RD orders at his/her discretion RD will not independently initiate PN or EN

29
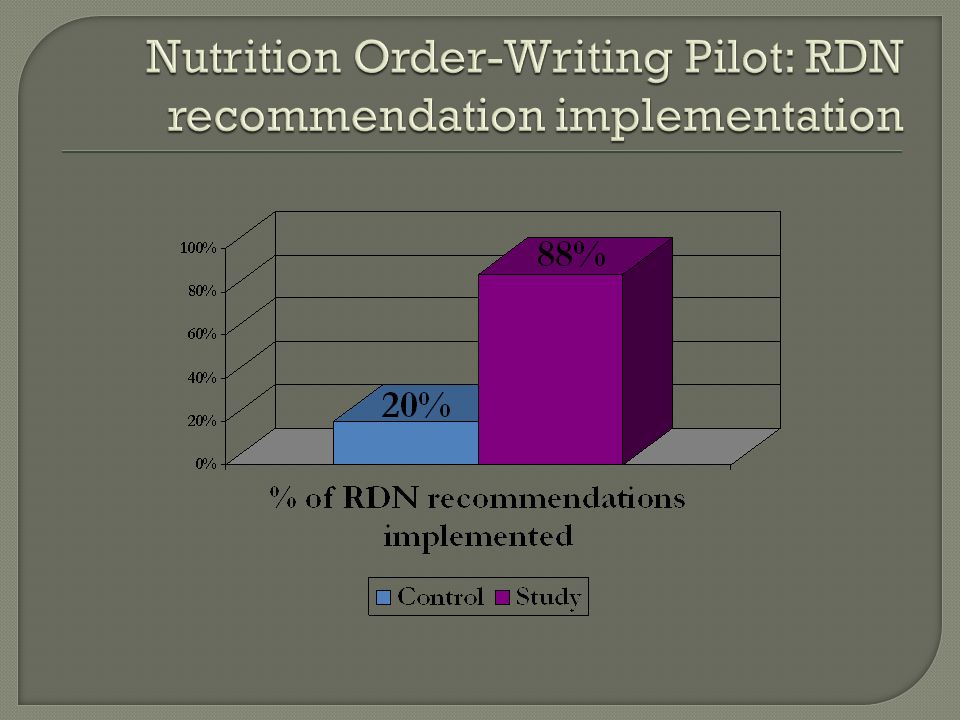
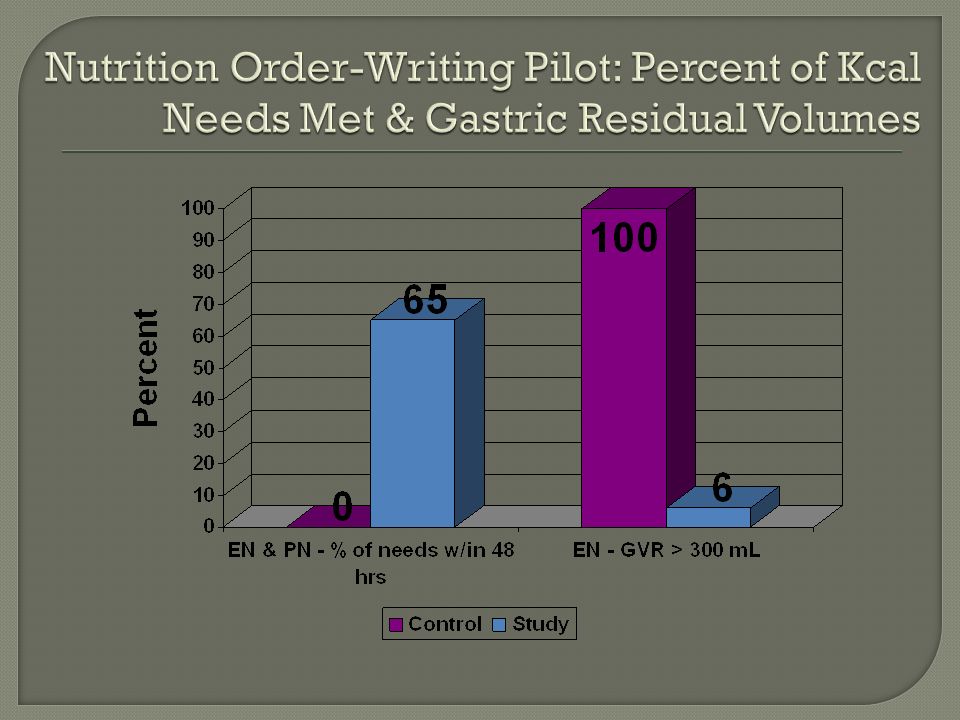
RD nutrition orders did not cause patient harm and were not discontinued by physicians RD nutrition order management: Increases implementation of RD recommendations Improves tolerance to medical nutrition therapy Decreases time to achieve caloric goals This study demonstrates RD independent nutrition order writing provides not only safe, but improved patient care

30
Support for RD writing nutrition-related orders Policy (Nutrition Management Protocol) drafted Final approval by the 3 different governing physician committees obtained Competency of staff (PN vs. other types of orders) Staffing levels to be adjusted (weekends and weekdays) Ongoing data collection and reporting to appropriate committees
 Staffing levels to be adjusted (weekends and weekdays) Ongoing data collection and reporting to appropriate committees.")
31
Parenteral Enteral Monitoring Oral Diets Nutritional Supplements

32
Daily parenteral nutrition orders including Macronutrients, micronutrients, electrolytes, medications including insulin Laboratory monitoring Alter IV fluid infusion rate Enteral nutrition orders including Formula type, rate, hours of infusion, modulars, probiotics, water flushes Laboratory monitoring KUB after tube placement Oral or enteral vitamin/mineral supplements

33
Height and/or weight measurement Add or change serum glucose monitoring Institute the Sliding Scale Insulin Protocol Measure energy expenditure via indirect calorimetry Bedside swallow evaluation Order or discontinue calorie count, as indicated

34
Oral Diets Increase or decrease diet consistency (in collaboration with speech therapist, if needed) Change calorie levels on calorie-restricted diets Modify diet restrictions as needed Nutritional Supplements (oral) Add or delete oral liquid nutritional supplements Add or delete modular supplements (protein, glutamine, fat, banana flakes, fiber, calories) Add or delete oral vitamin/mineral supplements Add probiotic
 Change calorie levels on calorie-restricted diets Modify diet restrictions as needed Nutritional Supplements (oral) Add or delete oral liquid nutritional supplements Add or delete modular supplements (protein, glutamine, fat, banana flakes, fiber, calories) Add or delete oral vitamin/mineral supplements Add probiotic")
35
Assess competency and willingness of staff Implement training if needed Develop a Competency Assessment Program Involve other disciplines for education as needed The Neighborhood by Jerry Van Amerongen

36
Registered & Licensed Dietitian, ≥ 1 year of experience At least 1 year of experience with Nutrition Support Demonstrate competency in writing orders for enteral nutrition, oral diets, oral supplements, and monitoring Earn ≥10 relevant (Enteral & Parenteral Nutrition Support) hours of CE every year RD’s writing PN orders: Certified Nutrition Support Clinician (CNSC) Pass the Baylor Nutrition Support Competency Examination, and demonstrate competency with writing a minimum of 10 parenteral nutrition orders
 hours of CE every year RD’s writing PN orders: Certified Nutrition Support Clinician (CNSC) Pass the Baylor Nutrition Support Competency Examination, and demonstrate competency with writing a minimum of 10 parenteral nutrition orders")
37
Electrolyte replacement guidelines for potassium, phosphorus, magnesium, and calcium Reminder list for the RD’s on medication interactions with tube feedings and PN, insulin, and glucose management and lab reports Physician-let presentation with tips for successful order writing through appropriate and effective interaction with physicians Competency check-off for PN order writing

38
To justify the need for additional full-time RD’s, PRN protocol time and full-time RD overtime was tracked along with the following information: Number of protocol patients Number of PN and EN protocol patients Number of non-protocol patients Time for protocol patient care and data collection Time for non-protocol patient care A “buddy list” for the RD’s who are not a CNSC- A designated CNSD/CNSC manages their PN orders Outcomes reported to appropriate committees

39
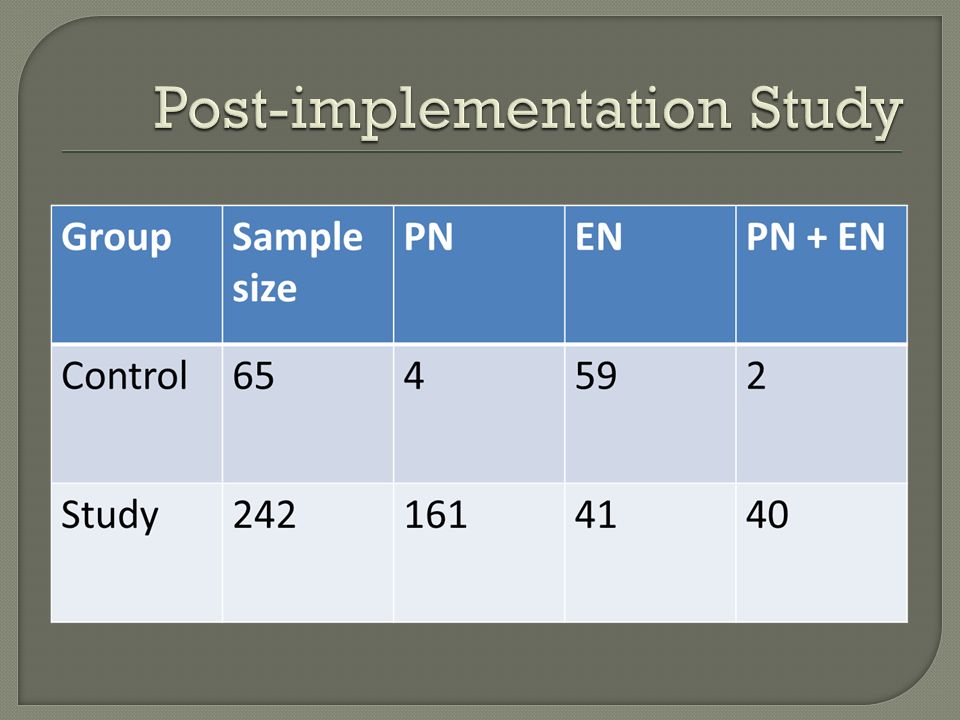
Data collection following implementation in November 2007- February 2008 Observational, non-randomized study Control group- EN/PN order written by MD N=65 Study group- EN/PN order written by RDN N=242

45
p = 0.046

46
p = 0.003

47
Percent of days with abnormal electrolytes

48
Percent of patients with and without nutrition-related complications p = 0.0018

49
14 Hospitals in the North Division- Nutrition Management Protocol (NMP) implemented in all hospitals Time to implement ranged from 6-18 months Steps to implementation included Establishing the need for the service (to enhance quality, cost savings, patient safety)- may require baseline data collection to establish the need Approval from appropriate committees including the medical board Assessment of staffing/training needs, competency check-off
 implemented in all hospitals Time to implement ranged from 6-18 months Steps to implementation included Establishing the need for the service (to enhance quality, cost savings, patient safety)- may require baseline data collection to establish the need Approval from appropriate committees including the medical board Assessment of staffing/training needs, competency check-off")
50
Existing relationship between RDs and physicians and strong physician support Persistence- took ~4 years from concept to implementation Pilot study and ongoing data collection which demonstrate improvements when the RD writes the PN versus the MD Administrative support for additional staffing

51
Lengthy process for approval from committees Physician and nursing education Staffing for weekends and holidays- require CNSC for PN order writing Ensuring ongoing competency of staff, new and existing Monitoring for quality, avoidance of errors

52
Ongoing data collection on glycemic control, electrolyte abnormalities, days on nutrition support, LOS Buddy system- pair a more experienced CNSC with a less experienced CNSC to act as a resource Error/near miss reporting process

53
Preparation and sitting for CNSC examination for many staff members Attending class on PN order writing, which included case studies and practice writing orders Successfully passing the BHCS Nutrition Support Exam 2-3 days of hands-on training and competency check-off: required to write minimum of 10 correct PN orders, including initial and ongoing orders, critically ill patients Annual competency check-off

54
Include NMP consult as option in Admission Order Sets- may be more feasible in smaller hospitals or for specific patient populations Ongoing order for patient’s stay- must keep NMP consult “active” versus completing it in the EHR Incorporate into Enteral and Parenteral Protocols as default RD consult Ensure the RD has the capability to enter orders, including labs and x-rays in the EHR- may have to explain RD SOP to other disciplines

55
Improves quality of care- the patient receives the right care in a more timely manner Maximizes the role of the RD- RD is able to use expertise and have a higher level of job satisfaction Saves time for other disciplines and RD- and team feels more cohesive Cost savings- decreases LOS, avoidance of complications and repeat orders

56
Check state licensure requirements and understand CMS guidelines related to order writing Obtain support from key physicians and other clinicians prior to submitting for approval Evaluate RD staff’s experience level and willingness to accept responsibility associated with order writing privileges Conduct a pilot study to demonstrate effectiveness of the protocol Collect outcomes data and explore/report cost savings with improved patient outcomes Track staffing time to justify need for more staff Establish an effective system for ongoing communication with and amongst RD staff

57
Communication- before implementation and ongoing- stress more collaboration between disciplines is needed, not less!! Understanding the hospital’s culture, key physician and nurse champions and committee structure/process for approval If writing PN orders, most staff will need additional training about electrolyte management Planning carefully for adequate staffing and training RD commitment to a higher level of accountability- “with privilege comes responsibility”

58
BUMC CNSC Dietitians

59
Developing advanced practice skills as a part of order writing is important Chart the course: set specific steps and goals Approval and implementation for performing certain skill or obtaining privileges cannot be accomplished alone Once implemented, RD staff must collaborate even more closely with other team members Collect data and share it!!

60
For further questions email: Susan Roberts: SusanRo@BaylorHealth.edu Kim Bandelier kim.bandelier@gmail.com Thank you

Similar presentations




 Texas Rules for ESRD Facilities What They Mean for the Renal Dietitian.>")





>")



 final rule allows RDNs privilege to: Order patient diets without.>")





