Download presentation
Presentation is loading. Please wait.

1
Safeguarding Children Essential Education Group 2

2
Why do we need to safeguard children ? For the purposes of child protection procedures, a child is anyone under the age of 18. All children deserve the opportunity to achieve their full potential. They should be enabled to be as physically and mentally healthy as possible, receive maximum benefit from educational opportunities, live in a safe environment, experience emotional well-being, feel loved and valued, become competent in looking after themselves, have a positive image of themselves and have opportunities to develop interpersonal skills and confidence. If they are denied the opportunity to achieve their potential in this way they are at risk, not only of an impoverished childhood, but of experiencing disadvantage and social exclusion in adulthood.

3
From what we hear in the press, are we as a nation safeguarding our children ? 1945 Dennis O’Neil 1973 Maria Colwell 1984 Jasmine Beckford 1984 Tyra Henry 1984 Heidi Koseda 1986 Kimberly Carlile 1987 Doreen Mason 1992 Leanne White 1994 Rikki Neave 1999 Chelsea Brown 2000 Victoria Climbie 2000 Lauren Wright 2002 Ainlee Labonte 2007 Peter Connelly 2008 Khyra Ishaq

4
How do you decide? Definitions Values Personal experience The law Professional experience With others Gut instincts Social / cultural norms Custom and practice Knowledge Statutory guidance Local procedures

5
Safeguarding Legislation Laming Report 2009 Following death of Baby P, Lord Laming asked to report: Every Child Matters 2003 In response to the Victoria Climbie Inquiry by Lord Laming 2003 Children’s Act 1989 & 2004

6
Focussing on optimal (best possible) outcomes Being healthy Staying safe Enjoying and achieving Making a positive contribution Achieving economic well-being ‘Every Child Matters’
 outcomes Being healthy Staying safe Enjoying and achieving Making a positive contribution Achieving economic well-being ‘Every Child Matters’")
7
All those who come into contact with children and families in their everyday work, including practitioners who do not have a specific role in relation to safeguarding children, have a duty to safeguard and promote the welfare of children. A Duty to Protect… ‘What to do if you’re worried a child is being abused’ HM Government 2006 (p.10) What does all this mean to us?
 What does all this mean to us .")
8
Neglect Physical injury Sexual abuse Emotional abuse Abuse can be inflicted against children, young people and those with learning disabilities. Abuse may take place in the family, the community and institutional settings, by those known to them or more rarely by a stranger. Need to consider: Fabricated illness and domestic violence. Categories of Abuse

9
Physical Abuse ‘Physical abuse may involve hitting, shaking, throwing, poisoning, burning or scalding, drowning, suffocating, or otherwise causing physical harm to a child. Physical harm may also be caused when a parent or carer fabricates the symptoms of, or deliberately induces, illness in a child.’ ‘Working Together’ 2010: 1.33

10
‘Any incident of threatening behaviour, violence or abuse between adults who are or have been intimate partners or family members, regardless of gender or sexuality.’ Can include any form of physical, sexual or emotional abuse between people in a close relationship. Such as: physical assault sexual abuse rape threats & intimidation Domestic Violence / Abuse

11
Sexual abuse ‘…involves forcing or enticing a child or young person to take part in sexual activities, not necessarily involving a high level of violence, whether or not the child is aware of what is happening. The activities may involve physical contact, including assault by penetration (for example, rape or oral sex) or non- penetrative acts such as masturbation, kissing, rubbing and touching outside of clothing.
 or non- penetrative acts such as masturbation, kissing, rubbing and touching outside of clothing..")
12
‘…They may include non-contact activities, such as involving children in looking at, or in the production of sexual images, watching sexual activities, encouraging children to behave in sexually inappropriate ways, or grooming a child in preparation for abuse (including via the internet). Sexual abuse is not solely perpetrated by adult males. Women can also commit acts of sexual abuse, as can other children.’ ‘Working Together’ 2010: 1.35 Sexual abuse ~ continued

13
Emotional Abuse ‘…is the persistent emotional maltreatment of a child such as to cause severe and persistent adverse effects on the child’s emotional development. It may involve conveying to children that they are worthless or unloved, inadequate, or valued only insofar as they meet the needs of another person. It may involve seeing or hearing the ill-treatment of another. It may involve serious bullying (including cyberbullying) causing children frequently to feel frightened or in danger, or the exploitation or corruption of children. Some level of emotional abuse is involved in all types of maltreatment of a child, though it may occur alone.’ ‘Working Together’ 2010: 1.34
 causing children frequently to feel frightened or in danger, or the exploitation or corruption of children. Some level of emotional abuse is involved in all types of maltreatment of a child, though it may occur alone.’ ‘Working Together’ 2010:")
14
Neglect Neglect ‘…is the persistent failure to meet a child’s basic physical and / or psychological needs, likely to result in the serious impairment of the child’s health or development. Neglect may occur during pregnancy as a result of maternal substance abuse.

15
Once a child is born, neglect may involve a parent or carer failing to: provide adequate food and clothing, shelter (including exclusion from home or abandonment)provide adequate food and clothing, shelter (including exclusion from home or abandonment) protect a child from physical and emotional harm or dangerprotect a child from physical and emotional harm or danger ensure adequate supervision (including the use of inadequate care-givers)ensure adequate supervision (including the use of inadequate care-givers) ensure access to appropriate medical care or treatmentensure access to appropriate medical care or treatment It may also include neglect of, or unresponsiveness to, a child’s basic emotional needs. ‘ ‘Working Together’ 2010: 1.36 Neglect ~ continued

16
Fabricated or Induced Illness (FII) Previously referred to as Munchausen’s Syndrome by proxy Is a condition whereby: Illness is fabricated or induced by parent/carer Child presented for medical care/assessment persistently Perpetrator denies aetiology Signs & symptoms cease when child separated from perpetrator
 Previously referred to as Munchausen’s Syndrome by proxy Is a condition whereby: Illness is fabricated or induced by parent/carer Child presented for medical care/assessment persistently Perpetrator denies aetiology Signs & symptoms cease when child separated from perpetrator")
17
Strong suspicions Sometimes you may be concerned about a child’s behaviour, injuries or circumstances you find them in but have nothing more to go on.

18
Child abuse is… ‘…anything which individuals, institutions or processes do, or fail to do, which directly, or indirectly harms children or damages their prospects of safe and healthy development into adulthood…’ From: ‘The Report of the National Commission of Enquiry into the Prevention of Child Abuse’ 1996

19
Child Development

20
Presentation Abuse may present in a variety of ways: Worrying injuries Numerous attendances at hospitals Allegations made by another person Disclosure by a young person / carer Parent/carers capacity to care impaired

21
Listening for child protection If a child discloses abuse, remember that this may be the beginning of a legal process, as well as of a process of recovery for the child. Legal action against a perpetrator can be seriously damaged by any suggestion that the child has been led in any way Rather than directly questioning the child, just listen and be supportive Never stop a child who is freely recalling significant events, but don’t push the child to tell you more than she wishes Write an account of the conversation immediately. Put the date and timings on it, and mention anyone else who was present. Then sign it, and hand your record in to your Line Manager, who should contact the Children’s Social Care District Office where appropriate

22
Pointers to NAI Story of the accident is vague and lacks detail Story is variable and changes with each telling Delay in seeking medical attention History is not compatible with the injury Many previous attendances with injuries or illnesses History of injury due to violence to other family members Child discloses abuse Abnormal appearance of the child and/or abnormal interaction with the carers Injuries in the non-mobile infant – consider the child’s age and development

23
Can we break a patients confidentiality to safeguard a child ?

24
Seven golden rules for information sharing 1.Remember that the Data Protection Act is not a barrier to sharing information but provides a framework to ensure that personal information about living persons is shared appropriately. 2. Be open and honest with the person (and/or their family where appropriate) from the outset about why, what, how and with whom information will, or could be shared, and seek their agreement, unless it is unsafe or inappropriate to do so. 3. Seek advice if you are in any doubt, without disclosing the identity of the person where possible.
 from the outset about why, what, how and with whom information will, or could be shared, and seek their agreement, unless it is unsafe or inappropriate to do so. 3. Seek advice if you are in any doubt, without disclosing the identity of the person where possible..")
25
4. Share with consent where appropriate and, where possible, respect the wishes of those who do not consent to share confidential information. You may still share information without consent if, in your judgement, that lack of consent can be overridden in the public interest. You will need to base your judgement on the facts of the case. 5. Consider safety and well-being: Base your information sharing decisions on considerations of the safety and well-being of the person and others who may be affected by their actions.

26
6. Necessary, proportionate, relevant, accurate, timely and secure: Ensure that the information you share is necessary for the purpose for which you are sharing it, is shared only with those people who need to have it, is accurate and up-to-date, is shared in a timely fashion, and is shared securely. 7. Keep a record of your decision and the reasons for it – whether it is to share information or not. If you decide to share, then record what you have shared, with whom and for what purpose.

27
Barriers to Reporting “The biggest barrier to diagnosis on NAI is the existence of emotional blocks in the minds of the professionals. These can be so powerful that they prevent the diagnosis being considered in even the most obvious cases. All those working with children should be warned that their overwhelming impulse will be to want to cover it up. The most important step in diagnosing NAI is to force yourself to think of it in the first place.” BMJ 1989 vol 298 P 879-881

28
Allegations against staff Keep parents/carers in room If child alone make efforts to contact parent Parental consent/responsibility Female to examine female & vice versa When examining a child ensure crew mate in room if at all possible

29
How should you respond? DO: Remain calm Listen carefully – make factual notes Communicate appropriately Be aware of your non-verbal messages Acknowledge their courage Do not: Show shock / distaste Probe for more information Make promises

30
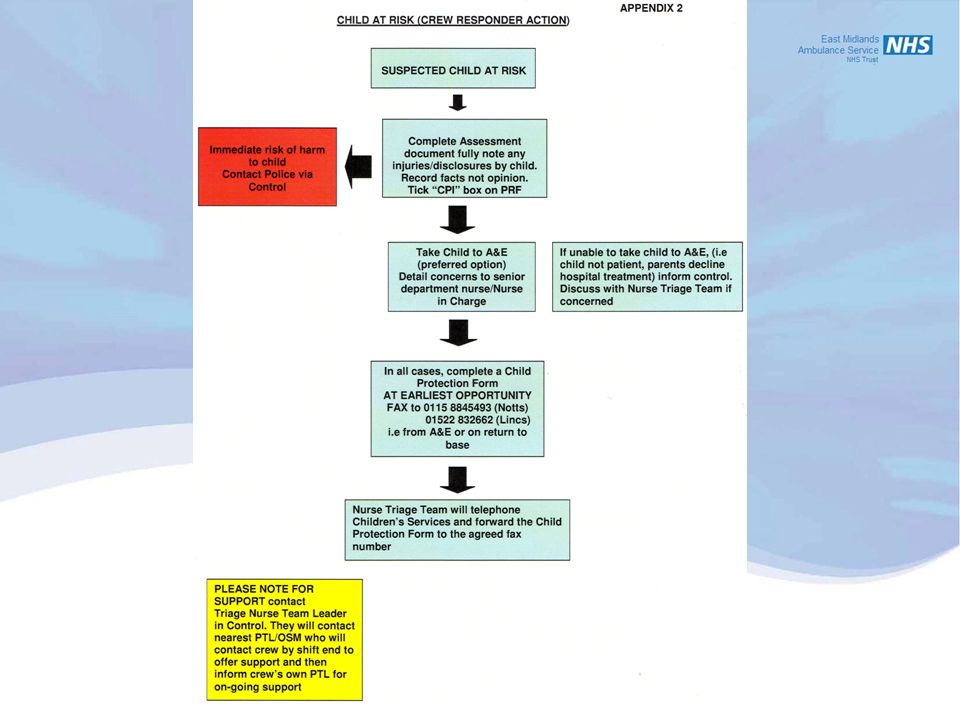
Actions: A B C History taking ? inform parents of your suspicions Convey to hospital if possible – ? Need police or another vehicle Inform triage nurse/discuss with triage nurse Fax completed report form to triage nurse for referral onto CSC Complete PRF Inform nurse at receiving hospital Care of yourself/crew mate

32
What happens next: Social care will investigate if appropriate Contact relevant agencies involved with child / family Medical procedures as required ? Case conference Identified as child / family in need Care package co-ordinated Rare to remove child from extended family

33
When a child or young person’s needs are not being met…

34
Sharing information = putting the whole picture together

Similar presentations


>")



>")






>")





