Download presentation
Presentation is loading. Please wait.

1
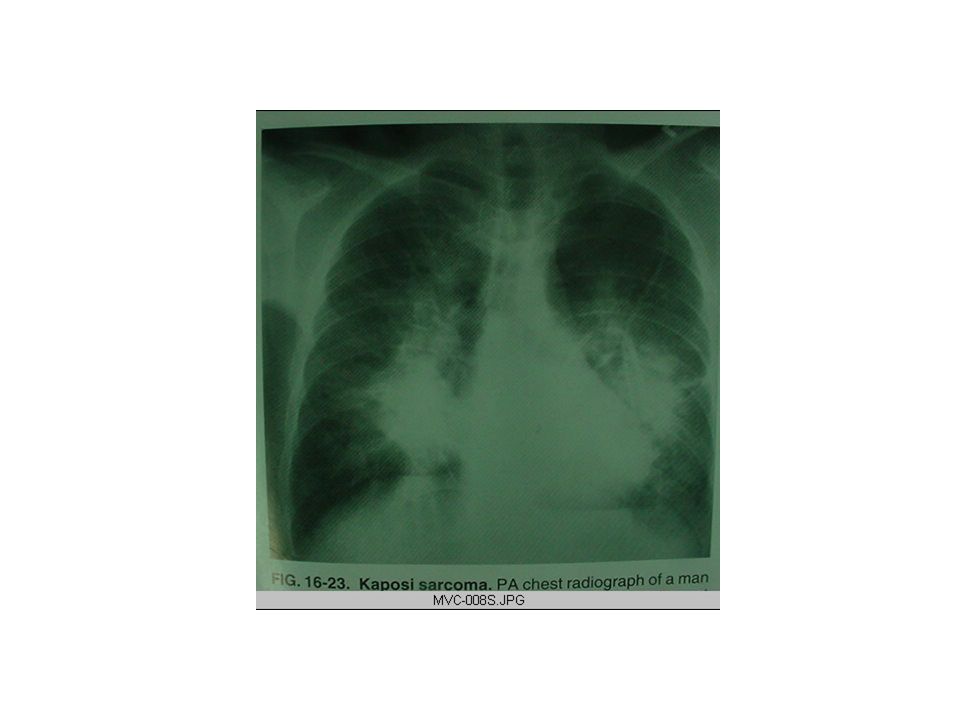
IMAGING PULMONARY MANIFESTATIONS OF HIV/AIDS Part I Dr.Mekashu & Degene, 2006

2
Non-infectious pul. manifestation in HIV/AIDS patients. A Great majority of the pulmonary complications of HIV infection are infectious in origin than non- infectious. Among non-infectious pulmonary complications are: Neoplasm Interstitial pneumonias

3
NEOPLASM PULMONARY COMPLICATION Kaposi’s sarcoma Lymphoma Bronchogenic carcinoma

4
KAPOSI'S SARCOMA: Epidemiology ed frequency in MSM (men who have sex with men) Middle aged to elderly white men Young black patients in Africa Extremely uncommon in women and children Incidence It was more (48%)early in epidemic Now only seen 18% of cases in MSM Pathophysiology It is an endothelial tumor Usually multicentriac Involves the skin &visceral organs KS associated herpes virus (KSHV type 8)
 Middle aged to elderly white men Young black patients in Africa Extremely uncommon in women and children Incidence It was more (48%)early in epidemic Now only seen 18% of cases in MSM Pathophysiology It is an endothelial tumor Usually multicentriac Involves the skin &visceral organs KS associated herpes virus (KSHV type 8)")
5
Very rarely involves the brain Risks More common in those with oral or anal sexual contacts Symptoms Genera:- lesions pruritic Initial:- painless Later:- lesions can be large and painful Signs cutaneous lesions A) Pigmented (violent col.) 1) Red to blue or bluish brown plaques and nodules B) Can involve any area of the skin especially on the soles of the foot affects the palm of the hand
 Pigmented (violent col.) 1) Red to blue or bluish brown plaques and nodules B) Can involve any area of the skin especially on the soles of the foot affects the palm of the hand")
6
C) Biopsy differentiate from 1)Cutaneous Cryptococcus Signs in pul. Involvement Rapidly fatal if not treated (enlarged plaques occlude segmental bronchi) Usually symptomatic: -Non-productive cough -Bronchospasm -Dyspnea -Ple. effusion in 20-50% at D x -Ple. Fluid is –ve for Ks -can be transudate or excaudate
 Usually symptomatic: -Non-productive cough -Bronchospasm -Dyspnea -Ple. effusion in 20-50% at D x -Ple. Fluid is –ve for Ks -can be transudate or excaudate.")
7
Radiological features Radiological features: KS are more specific and the diagnosis may sometimes be suggested in the basis of chest film and CT abnormality as: Poorly defined peribronchiovascular nodular density Typically measures 10-20 mm in diameter Solitary nodular KS may occur Bilateral multiple lesions are typically present Coarse linear opacities are also commonly scattered throughout the lungs, particularly in the perihilar and lower portions

8
Cont’d. Kerly B lines may be present (fig.16.22,23) The bronchovascular nodules can have a flame shaped appearance fig.16.21) Pericardial and pleural effusion and mediastenal lymphadinopaty are present Normal galinium scan Bronchoscopy -characteristic endobronchial lesions -Biopsy usually avoided 2 o to bleeding
 The bronchovascular nodules can have a flame shaped appearance fig.16.21) Pericardial and pleural effusion and mediastenal lymphadinopaty are present Normal galinium scan Bronchoscopy -characteristic endobronchial lesions -Biopsy usually avoided 2 o to bleeding.")
12
CT findings: ill-defined parenchymal nodules, which can be surrounded by small areas of ground-glass density Frequently bilateral perihilar pulmonary infiltrates are seen in majority of pts, which extends into the pulmonary parenchyma along the bronchovascular bundles (fig.5.68) Thickening of the interlobular septa Nodularities of the fissures pleural effusions, pericardial effusion Mediastenal lymphadinopaty Chest wall disease involving the sternum, ribs, thoracic spine and subcutanious tissues are observed
 Thickening of the interlobular septa Nodularities of the fissures pleural effusions, pericardial effusion Mediastenal lymphadinopaty Chest wall disease involving the sternum, ribs, thoracic spine and subcutanious tissues are observed")
14
Lymphoma: Is the 2 nd most frequent intrathoracic malignancy associated with HIV Due to long term stimulation by HIV virus, & EBV virus Lymphoma occurs ed frequency in AIDS pts., as a consequence of B-lymphocyte proliferation Most AIDS associated lymphomas are high grade aggressive B-cell type

15
Pathophysiology of lymphoma oCell neoplasia residing in lymphoid tissue oReticuloendothelial organ infiltration Types: A)Hodgkin’s lymphoma –Localized disease with contiguous nodal spread –Mediastinal involvement –Curability >75% –Systemic symptoms (fever,night sweating, wt.loss)
Hodgkin’s lymphoma –Localized disease with contiguous nodal spread –Mediastinal involvement –Curability >75% –Systemic symptoms (fever,night sweating, wt.loss)")
16
B) Non-Hodgkin’s lymphoma Non –contiguous nodal spread Extra nodal involvement Abdominal and bone marrow involvement Curability < 25% Risk factors Inherited Immunodeficiency syndrome Acquired Immunodeficiency oiatrogenic immunosuperation oAIDS o Acquired hypogammaglobulemia
 Non-Hodgkin’s lymphoma Non –contiguous nodal spread Extra nodal involvement Abdominal and bone marrow involvement Curability < 25% Risk factors Inherited Immunodeficiency syndrome Acquired Immunodeficiency oiatrogenic immunosuperation oAIDS o Acquired hypogammaglobulemia")
17
C)Autoimmune disease SLE Rheumatoid arthritis D) Chemical or drug exposure Phenytoin Radiation therapy Chemotherapy E) Viral association EBV Human T-cell Leukemia virus
Autoimmune disease SLE Rheumatoid arthritis D) Chemical or drug exposure Phenytoin Radiation therapy Chemotherapy E) Viral association EBV Human T-cell Leukemia virus")
19
CT-findings Revels similar findings & more sensitive than CXR Findings of axillary adenopathy with hilar &mediastinal Lns. the raise possibility of lymphoma Multiple nodes with bronchovascular & sub pleural distribution (fig.5.71,72),(16.24,26) Affecting predominantly the mid & lower lung zones.
,(16.24,26) Affecting predominantly the mid & lower lung zones..")
22
Bronchogenic carcinoma: There is 6.5 fold increase incidence of lung ca in HIV-infected and AIDS pts. The immunodepression however, renders the ca. likely to be highly malignant and clinically aggressive Mostly they are histologicaly Adenocarcinoma type It occurs in pts. who are younger than those with out AIDS Unlike KS and lymphoma, no associated mutagenic viral agent has been identified

23
Cont’d One of several neoplasms that arise within the lung Is one of the leading cause of death in USA & most industrialized countries Both in male & female Has subtypes -Adenocarcenoma------------35% -Squamous cell---------------25% -Small cell----------------------25% -Large cell----------------------15% Adenocarcenoma arises from bronchiolar or alveolar epithelium

24
If there is an increase in the prevalence of lung ca it may be 2 0 to deficiencies in immunoregulation In advanced stages (<200CD 4 cells / l) ; bronchoscopic investigation recommended Radiographic features oNo difference to those without HIV infected pts. with ca oHas solitary pul. Nodules(size b/n 2mm& 3cm) o it includes lung masses (>3mm or larger) (fig.16.19) oIt includes hilar mass with or without bronchial obstruction oPleural effusion o Presence of air bronchogram or bubbly lucencies within a nodule or mass is highly suggestive of ca.
 o it includes lung masses (>3mm or larger) (fig.16.19) oIt includes hilar mass with or without bronchial obstruction oPleural effusion o Presence of air bronchogram or bubbly lucencies within a nodule or mass is highly suggestive of ca..")
25
INTERSTITIAL PNEUMONIAS The common pul. disorders associated with HIV infection are: Lymphocytic interstitial pneumonites (LIP) Non-specific interstitial pneumonites (NIP) Others less common pul. disorders associated with HIV infection are: Pulmonary HPN COPA Bronchial hyperreactivity
 Non-specific interstitial pneumonites (NIP) Others less common pul. disorders associated with HIV infection are: Pulmonary HPN COPA Bronchial hyperreactivity.")
26
Cont ’ d. ARDS Alveolar proteinosis Sarcoidosis, Asthma, emphysema (in smokers) Cocaine users (unusual manifestation of pneumothorax or alveolar infiltrate) Drug induced reactions (e.g.. adverse reaction to trimethoprim etc.)
 Cocaine users (unusual manifestation of pneumothorax or alveolar infiltrate) Drug induced reactions (e.g.. adverse reaction to trimethoprim etc.).")
27
Lymphocytic interstitial pneumonites (LIP) Characterized by histological pattern of diffuse infiltration of alveolar walls and peribronchial areas by non-neoplastic mature lymphocyts, plasma cells,lymphoid cells etc. A variety of lympho prolypherative disorders are associated It takes chronic or sub chronic courses Extremely rare in adults (age difference is unknown) Paraneoplastic in some cases Para infective in HIV and EBV viruses
 Paraneoplastic in some cases Para infective in HIV and EBV viruses.")
28
In contrast to PCP, LIP pts. have CD 4 >200/ l A definite D x open-lung biopsy Sensitive to steroid The role play by HAART is unclear Clinical feature Presence of cough, breathlessness or clubbing of fingers With diffuse radiographic abnormality is consistence with PCP But the absence of fever and sever hypoxemia should suggest LIP Marked lymphocytosis in bronchoalveolar lavage is a confirmatory evidence of D x

29
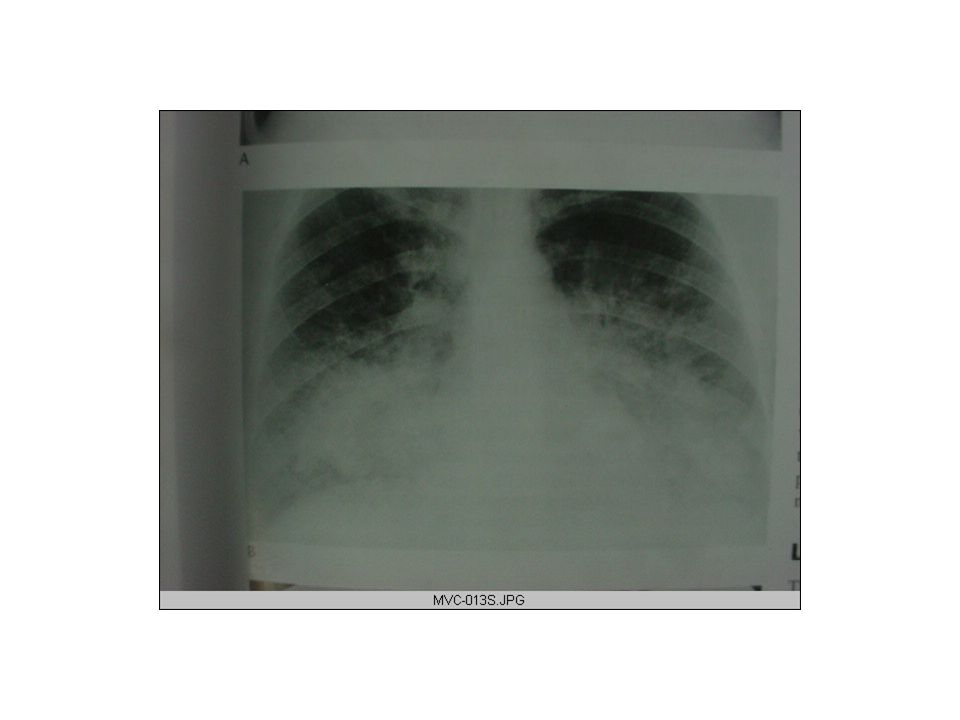
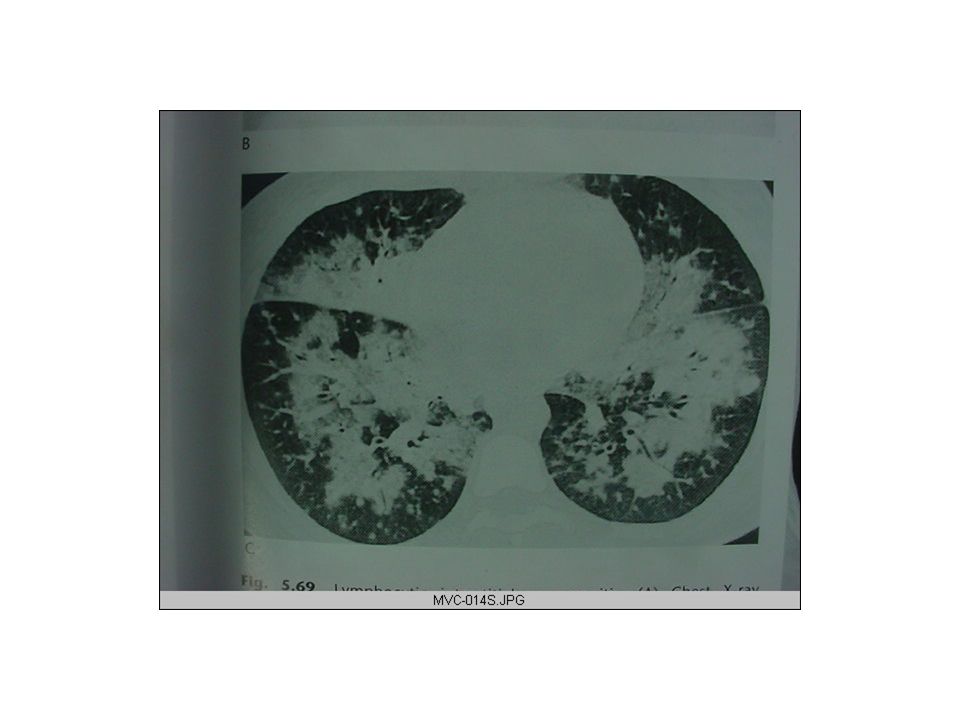
Radiographic feature -Characteristic radiographic of LIP is similar to PCP (fig 5.69). Diffuse bilateral reticulonodular infiltrates Associated hilar lymphadenopaty occasionally predominantly nodular pattern is seen Radionucliode: Similar uptake to PCP CT -findings Diffuse 2-4 mm diameter nodules, generally in a peribronchovascular distribution Bronchiectasis also seen

34
Non-specific interstitial pneumonites (NIP) Poorly defined condition that occurs in immunocompromised pts. with and without AIDS It has been attributed to a variety of causes including: -unidentified viral infection -drug therapy - and irradiation

35
Clinical features Histological pattern of mild to chronic NIP has been found in transbronchial biopsy specimen from both symptomatic and asymptomatic : In 50% of pts. or more are without symptoms It may occur at the time of worsening of HIV infection Failure to respond to R x for infective causes and relatively indolent coarse should raise the possibility of D x

36
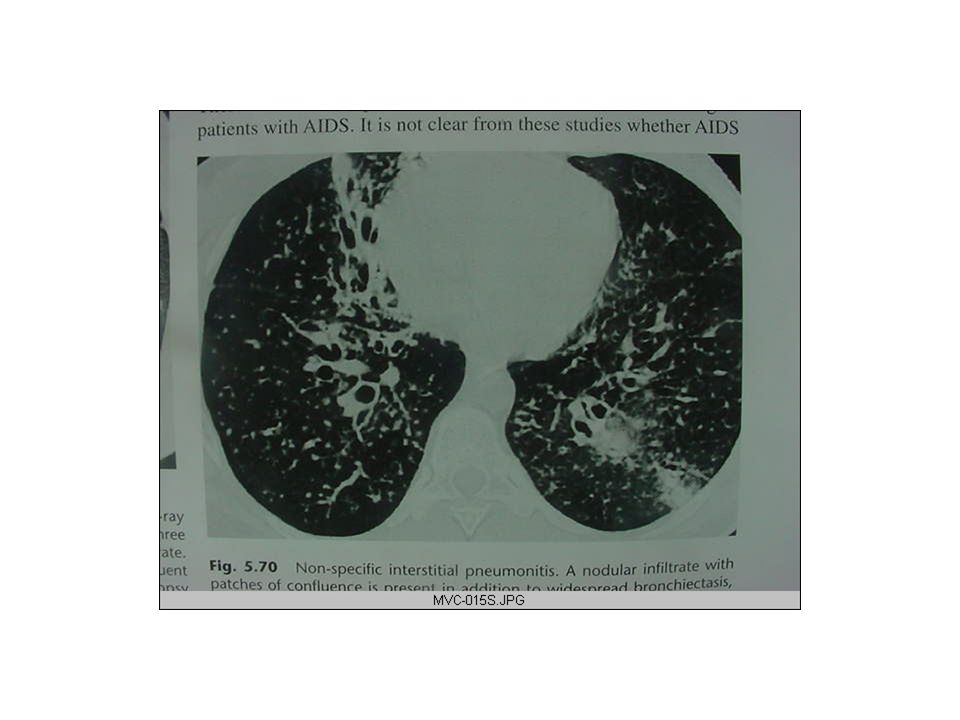
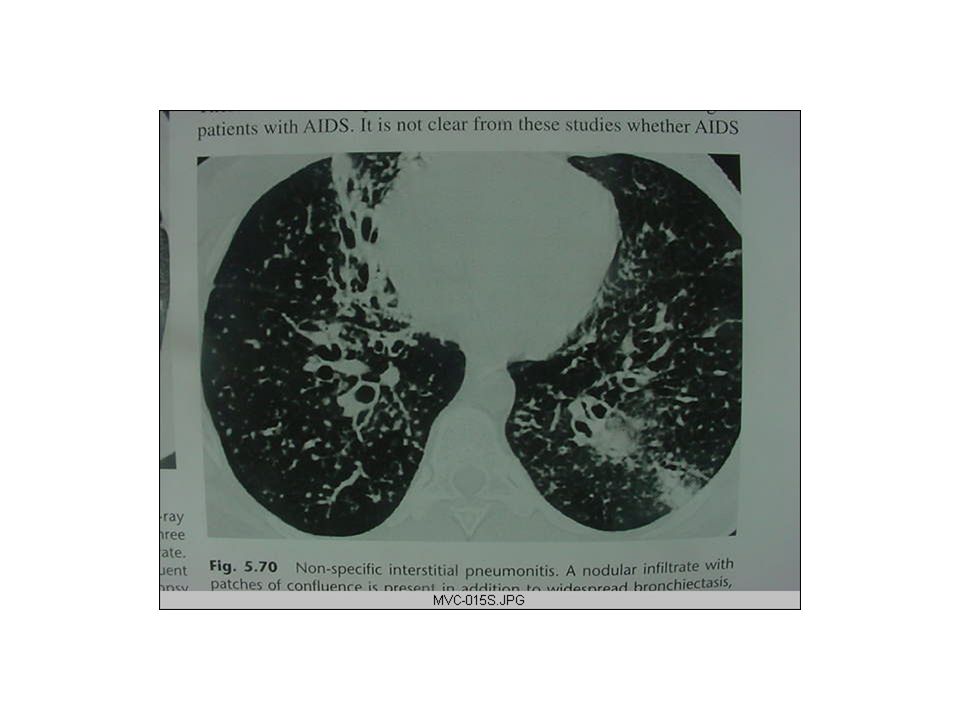
Radiography feature Nearly half of the pts. have normal CXR Others have diffuse or unilateral infiltrates of an interstitial &/or alveolar nature(fig.5.70) THE IMMUNE COMPROMISED CHILD AIDS in children differs from AIDS in Adults: -Has short incubation period - Children are more likely to have sever bacterial infections or CMv - They develop pulmonary lymphoid hyperplasia (PLH) & LIP which are rare in adults - They are less likely to be infected with TOXO, MBT, Cryptococcus & histoplasmosis
 THE IMMUNE COMPROMISED CHILD AIDS in children differs from AIDS in Adults: -Has short incubation period - Children are more likely to have sever bacterial infections or CMv - They develop pulmonary lymphoid hyperplasia (PLH) & LIP which are rare in adults - They are less likely to be infected with TOXO, MBT, Cryptococcus & histoplasmosis.")
38
-There are two patterns of presentation and progression In the 1 st yr. of life with sever infections & encephalopaty- which has poor prognosis Preschool and school age with bacterial and lymphoid tissue hyperplasia---: -survival is longer even to adolescence -Prognostic features are : Sensitivity of the disease in the mother The age of on set and severity at on set

39
Clinical features Failure to thrive, wt.lose, generalized lymphadinopaty, hepatosplenomegaly, recurrent infections, chr. diarrhea Radiologic feature: - In CXR pcp may be localized initially but typically there is rapid progression to generalized lung shadow which is mixed alveolar & interstitial infiltrate (fig.16.28),(6.19) 50% of infections occur at age 3-6 months 2/3 of the infections are the 1 st and only infective in origin
,(6.19) 50% of infections occur at age 3-6 months 2/3 of the infections are the 1 st and only infective in origin.")
41
-LIP/PLH- in 50% of pts. Insidious onset of clinical symptoms CXR is diffuse, symmetrical reticulonodular or nodular pattern (2-3mm) Mostly easily seen at the basis & periphery of the lungs hilar or mediastinal lymphadenopaty The nodules consists of collections of lymphocytes and plasma cells with no organism Children with LIP have increased generalized lymphadenopaty, increased salivary glands & finger clubbing Mediastinal or hilar adenopaty may be 2 0 to PLH,MBT, MAI, CMV, Lymphoma or fungal infection (than other opportunistic infec.)
 Mostly easily seen at the basis & periphery of the lungs hilar or mediastinal lymphadenopaty The nodules consists of collections of lymphocytes and plasma cells with no organism Children with LIP have increased generalized lymphadenopaty, increased salivary glands & finger clubbing Mediastinal or hilar adenopaty may be 2 0 to PLH,MBT, MAI, CMV, Lymphoma or fungal infection (than other opportunistic infec.).")
42
Generally investigating & imaging modalities Beside routine investigations: CXR is a preliminary inspection & is essential in planning the approach to u/s –guided biopsy and for others imaging modalities. U/S (best in viewing masses,nodules,for guidance of biopsy…etc) Fluoroscopy Bronchoscopes (br.alveolar lavage….etc) CT MRI
 Fluoroscopy Bronchoscopes (br.alveolar lavage….etc) CT MRI.")
43
THANK YOU!

Similar presentations
















 SHEN JIN The First Affiliated Hospital of Kunming Medical College.>")






