Download presentation
Presentation is loading. Please wait.

1
ELBOW TRAUMA

2
RADIAL HEAD FRACTURES

3
MASON CLASSIFICATION

4
NON-OP TREATMENT Indications: Tx: Sling for comfort
Mason 1 Mason 2 Tx: Sling for comfort Immobilization no more than 2 weeks to prevent elbow stiffness! Fracture displacement and nonunion is usually asymtomatic and inconsequential (Ring - CORR 2002, Cobb – Orthopedics 1998)
")
5
OPERATIVE INDICATIONS
Traditionally >2 mm displacement >30% of joint involvement Most Importantly: Blocked forearm rotation Mason 3 fracture (displaced comminuted)
")
6
OPERATIVE TX OPTIONS Excision ORIF Arthroplasty

7
RADIAL HEAD EXCISION Isolated radial head fracture
No Essex-Lopresti lesion No terrible triad No MCL injury In older patients with limited functional demands

8
ORIF Mason type 2: 15/15 had satisfactory result
Mason type 3 with 2-3 fragments: 1/12 nonunion Mason type 3 with >3 fragments: 13/14 had unsatisfactory results (Ring JBJS Am 2002) If >3 fragments, consider arthroplasty
 If >3 fragments, consider arthroplasty.")
9
ARTHROPLASTY N=16 80% good or excellent results at 2.8y f/u
Early mobilization important for satisfactory outcome (Bain JBJS Am 2005)
")
16
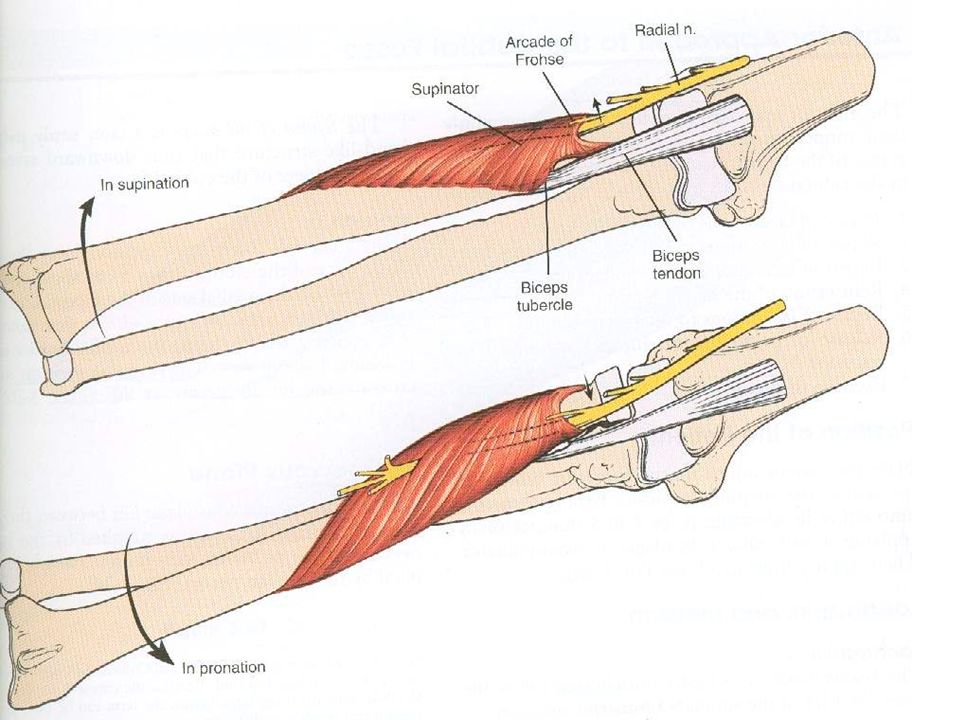
SURGICAL ANATOMY Pronation of forearm translates PIN 1 cm away from operative field Safe zone of lateral radius: Proximal 38 mm Supination decreases safe zone to 22 mm (Diliberti JBJS Am 2000)
")
17
IMPLANT PLACEMENT ON RADIAL HEAD
110° safe zone on lateral aspect to prevent impingement in sigmoid notch Make horizontal marks in forearm in neutral, pronation and supination Limits: Anterior: ½ distance from between mark in neutral and supination Posterior: 2/3 distance from between mark in neutral and pronation (Corresponds to region between Listers tubercle and radial styloid)
")
18
PROXIMAL ULNA FRACTURES

20
PROXIMAL ULNA FRACTURES: Treatment Options
Plating Tension Band

22
TENSION BAND (Macko JBJS Am 1985)
Most common complication: Prominent hardware Indication: Transverse fracture with no comminution

25
PLATING (Bailey JOT 2001) 22/25 good or excellent results
20% requested plate removal

30
CORONOID FRACTURES

31
CORONOID FRACTURE: Morrey and Regan Classification
Type 1: Avulsion of the tip of the process Type 2: 50% of the process Type 3: >50% of the process

32
CORONOID FRACTURES Type 1: Sutures around the fragment
Type 2: Sutures through drill holes in ulna Type 3: Screws Small fragments associated with more challenging injury pattern!

33
CORONOID FRACTURE: O’Driscoll’s Classification

34
ELBOW DISLOCATIONS

35
Lateral collateral ligament Coronoid Radial head
ELBOW STABILIZERS Lateral collateral ligament Coronoid Radial head

36
ELBOW DISLOCATION Non-op or Radial head excision + Cast
Good results if no coronoid fracture Radial head was ultimate determinant of outcome with many radial head resections needed to restore forearm rotation (Broberg & Morrey CORR 1987)
")
37
Elbow dislocation Coronoid fracture Radial head fracture
TERRIBLE TRIAD Elbow dislocation Coronoid fracture Radial head fracture

38
CURRENT MANAGEMENT Radial head ORIF or arthroplasty Coronoid fixation
If still unstable (dislocation with 30° Ext)
 ")
39
LCL + MCL REPAIR

40
CROSS PINS

41
EX-FIX

42
HINDGED BRACE

Similar presentations