Download presentation
Presentation is loading. Please wait.

1
Adult Immunizations Update 2016
Kenneth McCall, BSPharm, PharmD Associate Professor | UNE

2
Objectives Discuss the gap between current vaccination rates and Healthy People 2020 goals for vaccinations. Categorize each of the CDC recommended flu vaccines based upon live/inactivated, route, preparation, and storage. Discuss the influenza vaccines for 2016 including the new quadrivalent and mammalian cell vaccines. Identify vaccine contraindications and recommend vaccines based upon patient age and medical history. Apply ACIP recommendations and FDA approved indications for the CDC recommended vaccines. Recognize Maine state laws that regulate vaccine administration.

3
Outline Background & Principles of Vaccination Influenza Vaccines
Quadrivalent inactivated Quadrivalent live Mammalian High Dose Intradermal

4
Background & Principles of Vaccination

5
Classification of Vaccines
Live attenuated Weakened form of the “wild” virus or bacteria Inactivated Whole viruses or bacteria Fractions of viruses or bacteria *Epidemiology and Prevention of Vaccine-Preventable Diseases, 12th Edition

6
Classification of Vaccines
Live attenuated: Measles, mumps, rubella, varicella, zoster, intranasal influenza Inactivated: hepatitis A, hepatitis B, influenza, pneumonia, diphtheria, tetanus, pertussis, HPV, meningicoccal *Epidemiology and Prevention of Vaccine-Preventable Diseases, 12th Edition

7
In contrast to other preventive services, adult vaccination rates remain low for most routinely recommended vaccines and well below Healthy People 2020 goals.1 To estimate adult vaccination rates for influenza during the 2010–2011 influenza season, the CDC analyzed data from the Behavioral Risk Factor Surveillance System.2 34.8% of adults aged 18 to 64 years were vaccinated.2 The Healthy People 2020 goal is 80%.3 66.6% of adults aged 65 years and older were vaccinated.2 The Healthy People 2020 goal for this age group is 90%.3 The CDC also analyzed data from the 2010 National Health Interview Survey to further assess adult vaccination rates.1 Pneumococcal vaccination rates were 18.5% for high-risk adults aged 19 to 64 years and 59.7% for adults aged 65 years and older.2 The Healthy People 2020 goals are 60% (persons 18 to 64 years of age) and 90% (adults aged 65 years and older).3 The vaccination rate for herpes zoster vaccination of adults 60 years of age and older was 14.4%.2 The Healthy People 2020 goal is 30%.3 The vaccination rates for hepatitis B vaccination (≥3 doses) of adults aged 19 to 49 years were 42.0% for those at high risk for infection and 33.1% for those not at high risk.2 The Healthy People 2020 goal for hepatitis B vaccination for adults is to increase hepatitis B vaccine coverage among the following high-risk populations: long-term hemodialysis patients, men who have sex with men, health care personnel, and injection drug users. A goal of 90% has been targeted specifically for health care personnel. 1. Centers for Disease Control and Prevention (CDC). MMWR. 2012;61:61–80. 2. CDC. Final state specific influenza vaccination coverage estimates for the 2010–11 season—United States, National Immunization Survey and Behavioral Risk Factor Surveillance System, August 2010 through May Atlanta, GA: US Department of Health and Human Services, CDC; cdc.gov/flu/professionals/vaccination/coverage_1011estimates.htm. Accessed April 13, 2012. 3. US Department of Health and Human Services. healthypeople.gov/2020/topicsobjectives2020/pdfs/HP2020objectives.pdf. Accessed April 13, 2012. 7
 and 90% (adults aged 65 years and older).3. The vaccination rate for herpes zoster vaccination of adults 60 years of age and older was 14.4%.2 The Healthy People 2020 goal is 30%.3. The vaccination rates for hepatitis B vaccination (≥3 doses) of adults aged 19 to 49 years were 42.0% for those at high risk for infection and 33.1% for those not at high risk.2 The Healthy People 2020 goal for hepatitis B vaccination for adults is to increase hepatitis B vaccine coverage among the following high-risk populations: long-term hemodialysis patients, men who have sex with men, health care personnel, and injection drug users. A goal of 90% has been targeted specifically for health care personnel. 1. Centers for Disease Control and Prevention (CDC). MMWR. 2012;61:61– CDC. Final state specific influenza vaccination coverage estimates for the 2010–11 season—United States, National Immunization Survey and Behavioral Risk Factor Surveillance System, August 2010 through May Atlanta, GA: US Department of Health and Human Services, CDC; cdc.gov/flu/professionals/vaccination/coverage_1011estimates.htm. Accessed April 13, US Department of Health and Human Services. healthypeople.gov/2020/topicsobjectives2020/pdfs/HP2020objectives.pdf. Accessed April 13,")
8
Immunization Schedules
US Center for Disease and Prevention (CDC) Advisory Committee on Immunization Practices (ACIP) ACIP is a group of medical and public health experts who meet three times per year to discuss vaccine recommendations Published annually Adult schedule approved by American Academy of Family Physicians (AAFP) American College of Obstetricians and Gynecologists American College of Physicians American College of Nurse-Midwives
 Advisory Committee on Immunization Practices (ACIP) ACIP is a group of medical and public health experts who meet three times per year to discuss vaccine recommendations. Published annually. Adult schedule approved by. American Academy of Family Physicians (AAFP) American College of Obstetricians and Gynecologists. American College of Physicians. American College of Nurse-Midwives.")
9
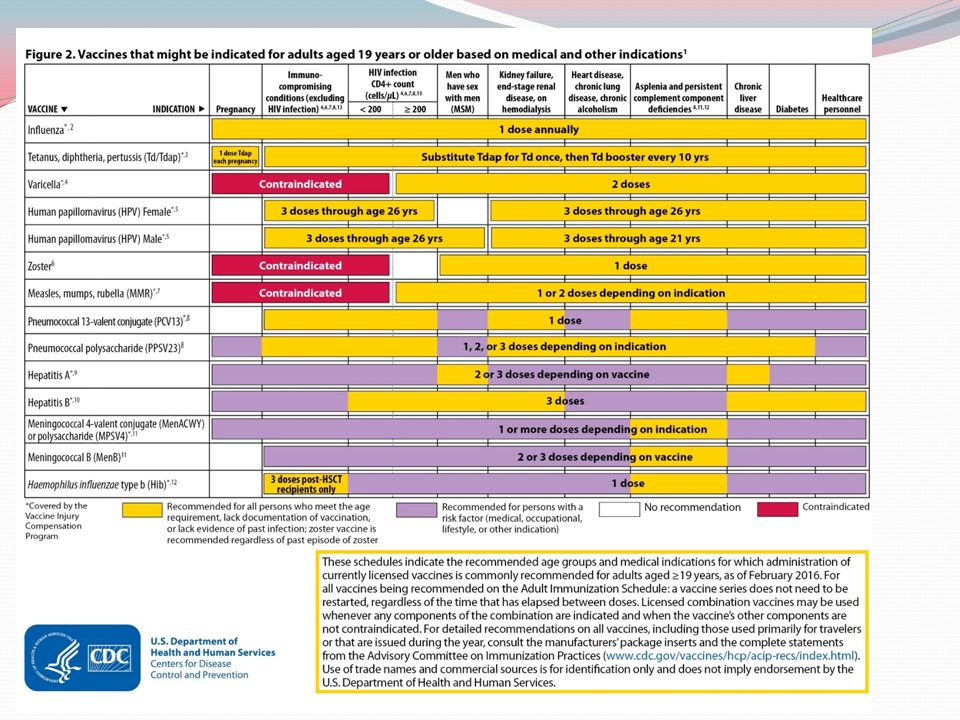
CDC ACIP 2016 Recommended Adult Immunization Schedule

11
State Regulations

13
Maine Pharmacist-Administered Immunization Regulations
No Rx Required Rx Requireda Rx or Protocol Not Permitted Adult (≥18 years) with PCPb Influenza ✓-RPh or Intern Other Vaccinesc Adult (≥18 years) without PCP Child < 18 years ✗ Child 7-17 years ✓-RPh only Child <7 years Sources: Maine H.P L.D and H.P. 836 L.D. 1218 Intern administration permitted as indicated under direct supervision of licensed pharmacist a Verbal/phone authorization acceptable b Primary care physician or existing relationship with a nurse practitioner or an authorized practitioner in Maine c All vaccines licensed by the US FDA recommended by the CDC ACIP
 with PCPb. Influenza. ✓-RPh or Intern. Other Vaccinesc. Adult (≥18 years) without PCP. Child < 18 years. ✗ Child 7-17 years. ✓-RPh only. Child <7 years. Sources: Maine H.P L.D and H.P. 836 L.D Intern administration permitted as indicated under direct supervision of licensed pharmacist. a Verbal/phone authorization acceptable. b Primary care physician or existing relationship with a nurse practitioner or an authorized practitioner in Maine. c All vaccines licensed by the US FDA recommended by the CDC ACIP.")
14
What is the Healthy People 2020 goal for annual flu vaccination for adults 65 and older?
100% 90% 70% 50%

15
Influenza Vaccines

16
Influenza A and B are the two types of influenza viruses that cause epidemic human disease. Since 1977, influenza A (H1N1 and H3N2) viruses and influenza B viruses have circulated globally.1 The influenza A virus is composed of a viral genome covered by a protein shell, the capsid. A lipid bi-layer envelops the capsid, as shown in the figure.2 Influenza A viruses are categorized into subtypes on the basis of two surface antigens: hemagglutinin and neuraminidase.1 Within the envelope is the influenza genome, which is organized into 8 pieces of single-stranded RNA.2 1. Centers for Disease Control and Prevention. MMWR Recomm Rep. 2010;59(RR-8):1–62. 2. Molecular Expressions: Cell Biology and Microscopy Structure and Function of Cells and Viruses. Accessed April 15, 2012. 16
:1– Molecular Expressions: Cell Biology and Microscopy Structure and Function of Cells and Viruses. Accessed April 15,")
17
Influenza versus Common Cold
Signs & Symptoms Influenza Common Cold Onset Sudden Gradual Fever High (>101°F) Less common (low grade) Cough Dry; can be severe Hacking or congested Headache Common Rare Myalgias Usual; severe Slight Fatigue/malaise Can last 2-3 weeks Very mild Extreme exhaustion Early and prominent Rare or never Chest discomfort Mild to moderate Stuffy nose Sometimes Sneezing Usual Sore throat Note - many people also confuse their symptoms of gastrointestinal infections with influenza
 Less common (low grade) Cough. Dry; can be severe. Hacking or congested. Headache. Common. Rare. Myalgias. Usual; severe. Slight. Fatigue/malaise. Can last 2-3 weeks. Very mild. Extreme exhaustion. Early and prominent. Rare or never. Chest discomfort. Mild to moderate. Stuffy nose. Sometimes. Sneezing. Usual. Sore throat. Note - many people also confuse their symptoms of gastrointestinal infections with influenza.")
18
ACIP Recommendations 2015-2016 Influenza Season
All persons aged 6 months and older should receive influenza vaccine annually. Persons who care for severely immunosuppressed persons who require a protective environment should not receive LAIV, or should avoid contact with such persons for 7 days after receipt, given the theoretical risk for transmission of the live attenuated vaccine virus. Persons who report having had reactions to egg involving such symptoms as angioedema, respiratory distress, lightheadedness, or recurrent emesis; or who required epinephrine or another emergency medical intervention, may receive Flublok if they are aged 18 years or older and there are no other contraindications. LAIV: live attenuated influenza vaccine

19
2015-2016 Vaccine Coverage & Age Group Distribution of Influenza Positive Specimens
Trivalent A/California/7/2009 (H1N1)-like virus A/Switzerland/ / (H3N2)-like virus B/Phuket/3073/2013-like virus (Yamagata) Quadrivalent B/Brisbane/60/2008-like virus (Victoria) The flu vaccine's effectiveness may vary depending on age, health, and immune status and how well scientists identity circulating viruses. In , vaccine effectiveness was under 20%.
-like virus. A/Switzerland/ /2013 (H3N2)-like virus. B/Phuket/3073/2013-like virus (Yamagata) Quadrivalent. B/Brisbane/60/2008-like virus (Victoria) The flu vaccine s effectiveness may vary depending on age, health, and immune status and how well scientists identity circulating viruses. In , vaccine effectiveness was under 20%.")
20
A (H1N1) A (H3) B (Yamagata) B (Victoria)

21
Egg Allergy Recommendation
Persons with egg allergy may tolerate egg in baked products (e.g., bread or cake). Tolerance to egg-containing foods does not exclude the possibility of egg allergy. Abbreviations: IIV = inactivated influenza vaccine, trivalent or quadrivalent; RIV3 = recombinant influenza vaccine, trivalent. For the 2015–16 influenza season, ACIP recommends the following: Persons with a history of egg allergy who have experienced only hives after exposure to egg should receive influenza vaccine. Because relatively few data are available for use of LAIV in this setting, IIV or trivalent recombinant influenza vaccine (RIV3) should be used. RIV3 may be used for persons aged ≥18 years who have no other contraindications. However, IIV (egg- or cell culture-based) may also be used, with the following additional safety measures (Figure 2): Vaccine should be administered by a health care provider who is familiar with the potential manifestations of egg allergy; and Vaccine recipients should be observed for ≥30 minutes for signs of a reaction after administration of each vaccine dose. Persons who report having had reactions to egg involving such symptoms as angioedema, respiratory distress, lightheadedness, or recurrent emesis; or who required epinephrine or another emergency medical intervention, may receive RIV3 if they are aged ≥18 years and there are no other contraindications. If RIV3 is not available or the recipient is not within the indicated age range, IIV should be administered by a physician with experience in the recognition and management of severe allergic conditions (Figure 2). Regardless of allergy history, all vaccines should be administered in settings in which personnel and equipment for rapid recognition and treatment of anaphylaxis are available (38). Persons who are able to eat lightly cooked egg (e.g., scrambled egg) without reaction are unlikely to be allergic. Egg-allergic persons might tolerate egg in baked products (e.g., bread or cake). Tolerance to egg-containing foods does not exclude the possibility of egg allergy. Egg allergy can be confirmed by a consistent medical history of adverse reactions to eggs and egg-containing foods, plus skin and/or blood testing for immunoglobulin E directed against egg proteins (39). For persons with no known history of exposure to egg, but who are suspected of being egg-allergic on the basis of previously performed allergy testing, consultation with a physician with expertise in the management of allergic conditions should be obtained before vaccination (Figure 2). Alternatively, RIV3 may be administered if the recipient is aged ≥18 years. A previous severe allergic reaction to influenza vaccine, regardless of the component suspected of being responsible for the reaction, is a contraindication to future receipt of the vaccine. Abbreviations: IIV = inactivated influenza vaccine, trivalent or quadrivalent; RIV3 = recombinant influenza vaccine, trivalent. * Persons with egg allergy may tolerate egg in baked products (e.g., bread or cake). Tolerance to egg-containing foods does not exclude the possibility of egg allergy (Erlewyn-Lajeunesse et al., Recommendations for the administration of influenza vaccine in children allergic to egg. BMJ 2009;339:b3680). † For persons who have no known history of exposure to egg, but who are suspected of being egg-allergic on the basis of previously performed allergy testing, consultation with a physician with expertise in the management of allergic conditions should be obtained prior to vaccination. Alternatively, RIV3 may be administered if the recipient is aged ≥18 years. Alternate Text: The figure above is a flow chart showing recommendations regarding influenza vaccination of persons who report allergy to eggs in the United States for the influenza season.
. Tolerance to egg-containing foods does not exclude the possibility of egg allergy. Abbreviations: IIV = inactivated influenza vaccine, trivalent or quadrivalent; RIV3 = recombinant influenza vaccine, trivalent. For the 2015–16 influenza season, ACIP recommends the following: Persons with a history of egg allergy who have experienced only hives after exposure to egg should receive influenza vaccine. Because relatively few data are available for use of LAIV in this setting, IIV or trivalent recombinant influenza vaccine (RIV3) should be used. RIV3 may be used for persons aged ≥18 years who have no other contraindications. However, IIV (egg- or cell culture-based) may also be used, with the following additional safety measures (Figure 2): Vaccine should be administered by a health care provider who is familiar with the potential manifestations of egg allergy; and. Vaccine recipients should be observed for ≥30 minutes for signs of a reaction after administration of each vaccine dose. Persons who report having had reactions to egg involving such symptoms as angioedema, respiratory distress, lightheadedness, or recurrent emesis; or who required epinephrine or another emergency medical intervention, may receive RIV3 if they are aged ≥18 years and there are no other contraindications. If RIV3 is not available or the recipient is not within the indicated age range, IIV should be administered by a physician with experience in the recognition and management of severe allergic conditions (Figure 2). Regardless of allergy history, all vaccines should be administered in settings in which personnel and equipment for rapid recognition and treatment of anaphylaxis are available (38). Persons who are able to eat lightly cooked egg (e.g., scrambled egg) without reaction are unlikely to be allergic. Egg-allergic persons might tolerate egg in baked products (e.g., bread or cake). Tolerance to egg-containing foods does not exclude the possibility of egg allergy. Egg allergy can be confirmed by a consistent medical history of adverse reactions to eggs and egg-containing foods, plus skin and/or blood testing for immunoglobulin E directed against egg proteins (39). For persons with no known history of exposure to egg, but who are suspected of being egg-allergic on the basis of previously performed allergy testing, consultation with a physician with expertise in the management of allergic conditions should be obtained before vaccination (Figure 2). Alternatively, RIV3 may be administered if the recipient is aged ≥18 years. A previous severe allergic reaction to influenza vaccine, regardless of the component suspected of being responsible for the reaction, is a contraindication to future receipt of the vaccine Abbreviations: IIV = inactivated influenza vaccine, trivalent or quadrivalent; RIV3 = recombinant influenza vaccine, trivalent. * Persons with egg allergy may tolerate egg in baked products (e.g., bread or cake). Tolerance to egg-containing foods does not exclude the possibility of egg allergy (Erlewyn-Lajeunesse et al., Recommendations for the administration of influenza vaccine in children allergic to egg. BMJ 2009;339:b3680). † For persons who have no known history of exposure to egg, but who are suspected of being egg-allergic on the basis of previously performed allergy testing, consultation with a physician with expertise in the management of allergic conditions should be obtained prior to vaccination. Alternatively, RIV3 may be administered if the recipient is aged ≥18 years. Alternate Text: The figure above is a flow chart showing recommendations regarding influenza vaccination of persons who report allergy to eggs in the United States for the influenza season.")
22
Influenza Vaccines – United States, 2015-2016 Influenza Season
Trade name Manufacturer Presentation Mercury (from thimerosal) µg/0.5 mL Ovalbumin µg/0.5 mL Age indications Latex Route Inactivated influenza vaccine, quadrivalent (IIV4), standard dose Contraindications*: Severe allergic reaction to any vaccine component, including egg protein, or after previous dose of any influenza vaccine. Precautions*: Moderate to severe acute illness with or without fever; history of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine. Fluarix Quadrivalent GlaxoSmithKline 0.5 mL single-dose prefilled syringe — ≤0.05 ≥3 yrs No IM† FluLaval Quadrivalent ID Biomedical Corp. 5.0 mL multi-dose vial <25 ≤0.3 Fluzone Quadrivalent Sanofi Pasteur 0.25 mL single-dose prefilled syringe 6 through 35 mos ≥36 mos 0.5 mL single-dose vial 25 ≥6 mos Fluzone Intradermal¶ Quadrivalent 0.1 mL single-dose prefilled microinjection system 18 through 64 yrs ID** Abbreviations: ACIP = Advisory Committee on Immunization Practices; ID = intradermal; IM = intramuscular; IN = intranasal. * Immunization providers should check Food and Drug Administration-approved prescribing information for 2015–16 influenza vaccines for the most complete and updated information, including (but not limited to) indications, contraindications, warnings, and precautions. Package inserts for U.S.-licensed vaccines are available at † For adults and older children, the recommended site for intramuscular influenza vaccination is the deltoid muscle. The preferred site for infants and young children is the anterolateral aspect of the thigh. Specific guidance regarding site and needle length for intramuscular administration may be found in the ACIP General Recommendations on Immunization, available at § Available upon request from Sanofi Pasteur (1–800–822–2463 or ¶ Quadrivalent inactivated influenza vaccine, intradermal: a 0.1-mL dose contains 9 µg of each vaccine antigen (36 µg total). ** The preferred injection site is over the deltoid muscle. Fluzone Intradermal Quadrivalent is administered using the delivery system included with the vaccine. †† Age indication per package insert is ≥5 years; however, ACIP recommends Afluria not be used in children aged 6 months through 8 years because of increased risk of febrile reactions noted in this age group with bioCSL's 2010 Southern Hemisphere IIV3. If no other age-appropriate, licensed inactivated seasonal influenza vaccine is available for a child aged 5 through 8 years who has a medical condition that increases the child's risk for influenza complications, Afluria can be used; however, providers should discuss with the parents or caregivers the benefits and risks of influenza vaccination with Afluria before administering this vaccine. Afluria may be used in persons aged ≥9 years. §§ Syringe tip cap may contain natural rubber latex. ¶¶ Information not included in package insert. Estimated to contain <50 femtograms (5x10-8 µg) of total egg protein (of which ovalbumin is a fraction) per 0.5 mL dose of Flucelvax. *** Trivalent inactivated influenza vaccine, high-dose: a 0.5-mL dose contains 60 µg of each vaccine antigen (180 µg total).
 µg/0.5 mL. Ovalbumin. µg/0.5 mL. Age indications. Latex. Route. Inactivated influenza vaccine, quadrivalent (IIV4), standard dose. Contraindications*: Severe allergic reaction to any vaccine component, including egg protein, or after previous dose of any influenza vaccine. Precautions*: Moderate to severe acute illness with or without fever; history of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine. Fluarix Quadrivalent. GlaxoSmithKline. 0.5 mL single-dose prefilled syringe. — ≤0.05. ≥3 yrs. No. IM† FluLaval Quadrivalent. ID Biomedical Corp. 5.0 mL multi-dose vial. <25. ≤0.3. Fluzone Quadrivalent. Sanofi Pasteur mL single-dose prefilled syringe. 6 through 35 mos. ≥36 mos. 0.5 mL single-dose vial. 25. ≥6 mos. Fluzone Intradermal¶ Quadrivalent. 0.1 mL single-dose prefilled microinjection system. 18 through 64 yrs. ID** Abbreviations: ACIP = Advisory Committee on Immunization Practices; ID = intradermal; IM = intramuscular; IN = intranasal. * Immunization providers should check Food and Drug Administration-approved prescribing information for 2015–16 influenza vaccines for the most complete and updated information, including (but not limited to) indications, contraindications, warnings, and precautions. Package inserts for U.S.-licensed vaccines are available at † For adults and older children, the recommended site for intramuscular influenza vaccination is the deltoid muscle. The preferred site for infants and young children is the anterolateral aspect of the thigh. Specific guidance regarding site and needle length for intramuscular administration may be found in the ACIP General Recommendations on Immunization, available at § Available upon request from Sanofi Pasteur (1–800–822–2463 or ¶ Quadrivalent inactivated influenza vaccine, intradermal: a 0.1-mL dose contains 9 µg of each vaccine antigen (36 µg total). ** The preferred injection site is over the deltoid muscle. Fluzone Intradermal Quadrivalent is administered using the delivery system included with the vaccine. †† Age indication per package insert is ≥5 years; however, ACIP recommends Afluria not be used in children aged 6 months through 8 years because of increased risk of febrile reactions noted in this age group with bioCSL s 2010 Southern Hemisphere IIV3. If no other age-appropriate, licensed inactivated seasonal influenza vaccine is available for a child aged 5 through 8 years who has a medical condition that increases the child s risk for influenza complications, Afluria can be used; however, providers should discuss with the parents or caregivers the benefits and risks of influenza vaccination with Afluria before administering this vaccine. Afluria may be used in persons aged ≥9 years. §§ Syringe tip cap may contain natural rubber latex. ¶¶ Information not included in package insert. Estimated to contain <50 femtograms (5x10-8 µg) of total egg protein (of which ovalbumin is a fraction) per 0.5 mL dose of Flucelvax. *** Trivalent inactivated influenza vaccine, high-dose: a 0.5-mL dose contains 60 µg of each vaccine antigen (180 µg total).")
23
Influenza Vaccines, 2015-2016 Influenza Season cont’d
Trade name Manufacturer Presentation Mercury (from thimerosal) µg/0.5 mL Ovalbumin µg/0.5 mL Age indications Latex Route Inactivated influenza vaccine, trivalent (IIV3), standard dose Contraindications*: Severe allergic reaction to any vaccine component, including egg protein, or after previous dose of any influenza vaccine. Precautions*: Moderate to severe acute illness with or without fever; history of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine. Afluria bioCSL 0.5 mL single-dose prefilled syringe — <1 ≥9 yrs†† No IM† 5.0 mL multi-dose vial 24.5 ≥9 yrs†† via needle;18 through 64 yrs via jet injector Fluvirin Novartis Vaccines and Diagnostics ≤1 ≥4 yrs Yes§§ 25 Fluzone Sanofi Pasteur ≥6 mos Abbreviations: ACIP = Advisory Committee on Immunization Practices; ID = intradermal; IM = intramuscular; IN = intranasal. * Immunization providers should check Food and Drug Administration-approved prescribing information for 2015–16 influenza vaccines for the most complete and updated information, including (but not limited to) indications, contraindications, warnings, and precautions. Package inserts for U.S.-licensed vaccines are available at † For adults and older children, the recommended site for intramuscular influenza vaccination is the deltoid muscle. The preferred site for infants and young children is the anterolateral aspect of the thigh. Specific guidance regarding site and needle length for intramuscular administration may be found in the ACIP General Recommendations on Immunization, available at § Available upon request from Sanofi Pasteur (1–800–822–2463 or ¶ Quadrivalent inactivated influenza vaccine, intradermal: a 0.1-mL dose contains 9 µg of each vaccine antigen (36 µg total). ** The preferred injection site is over the deltoid muscle. Fluzone Intradermal Quadrivalent is administered using the delivery system included with the vaccine. †† Age indication per package insert is ≥5 years; however, ACIP recommends Afluria not be used in children aged 6 months through 8 years because of increased risk of febrile reactions noted in this age group with bioCSL's 2010 Southern Hemisphere IIV3. If no other age-appropriate, licensed inactivated seasonal influenza vaccine is available for a child aged 5 through 8 years who has a medical condition that increases the child's risk for influenza complications, Afluria can be used; however, providers should discuss with the parents or caregivers the benefits and risks of influenza vaccination with Afluria before administering this vaccine. Afluria may be used in persons aged ≥9 years. §§ Syringe tip cap may contain natural rubber latex. ¶¶ Information not included in package insert. Estimated to contain <50 femtograms (5x10-8 µg) of total egg protein (of which ovalbumin is a fraction) per 0.5 mL dose of Flucelvax. *** Trivalent inactivated influenza vaccine, high-dose: a 0.5-mL dose contains 60 µg of each vaccine antigen (180 µg total).
 µg/0.5 mL. Ovalbumin. µg/0.5 mL. Age indications. Latex. Route. Inactivated influenza vaccine, trivalent (IIV3), standard dose. Contraindications*: Severe allergic reaction to any vaccine component, including egg protein, or after previous dose of any influenza vaccine. Precautions*: Moderate to severe acute illness with or without fever; history of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine. Afluria. bioCSL. 0.5 mL single-dose prefilled syringe. — <1. ≥9 yrs†† No. IM† 5.0 mL multi-dose vial ≥9 yrs†† via needle;18 through 64 yrs via jet injector. Fluvirin. Novartis Vaccines and Diagnostics. ≤1. ≥4 yrs. Yes§§ 25. Fluzone. Sanofi Pasteur. ≥6 mos. Abbreviations: ACIP = Advisory Committee on Immunization Practices; ID = intradermal; IM = intramuscular; IN = intranasal. * Immunization providers should check Food and Drug Administration-approved prescribing information for 2015–16 influenza vaccines for the most complete and updated information, including (but not limited to) indications, contraindications, warnings, and precautions. Package inserts for U.S.-licensed vaccines are available at † For adults and older children, the recommended site for intramuscular influenza vaccination is the deltoid muscle. The preferred site for infants and young children is the anterolateral aspect of the thigh. Specific guidance regarding site and needle length for intramuscular administration may be found in the ACIP General Recommendations on Immunization, available at § Available upon request from Sanofi Pasteur (1–800–822–2463 or ¶ Quadrivalent inactivated influenza vaccine, intradermal: a 0.1-mL dose contains 9 µg of each vaccine antigen (36 µg total). ** The preferred injection site is over the deltoid muscle. Fluzone Intradermal Quadrivalent is administered using the delivery system included with the vaccine. †† Age indication per package insert is ≥5 years; however, ACIP recommends Afluria not be used in children aged 6 months through 8 years because of increased risk of febrile reactions noted in this age group with bioCSL s 2010 Southern Hemisphere IIV3. If no other age-appropriate, licensed inactivated seasonal influenza vaccine is available for a child aged 5 through 8 years who has a medical condition that increases the child s risk for influenza complications, Afluria can be used; however, providers should discuss with the parents or caregivers the benefits and risks of influenza vaccination with Afluria before administering this vaccine. Afluria may be used in persons aged ≥9 years. §§ Syringe tip cap may contain natural rubber latex. ¶¶ Information not included in package insert. Estimated to contain <50 femtograms (5x10-8 µg) of total egg protein (of which ovalbumin is a fraction) per 0.5 mL dose of Flucelvax. *** Trivalent inactivated influenza vaccine, high-dose: a 0.5-mL dose contains 60 µg of each vaccine antigen (180 µg total).")
24
Influenza Vaccines, 2015-2016 Influenza Season cont’d
Trade name Manufacturer Presentation Mercury (from thimerosal) µg/0.5 mL Ovalbumin µg/0.5 mL Age indications Latex Route Inactivated influenza vaccine, cell-culture-based (ccIIV3), standard dose Contraindications*: Severe allergic reaction to any vaccine component, including egg protein, or after previous dose of any influenza vaccine. Precautions*: Moderate to severe acute illness with or without fever; history of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine. Flucelvax Novartis Vaccines and Diagnostics 0.5 mL single-dose prefilled syringe — ¶¶ ≥18 yrs Yes§§ IM† Inactivated influenza vaccine, trivalent (IIV3), high dose Fluzone High-Dose*** Sanofi Pasteur ≥65 yrs No Recombinant influenza vaccine, trivalent (RIV3), standard dose Contraindications*: Severe allergic reaction to any vaccine component. Precautions*: Moderate to severe acute illness with or without fever; history of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine. Flublok Protein Sciences 0.5 mL single-dose vial Abbreviations: ACIP = Advisory Committee on Immunization Practices; ID = intradermal; IM = intramuscular; IN = intranasal. * Immunization providers should check Food and Drug Administration-approved prescribing information for 2015–16 influenza vaccines for the most complete and updated information, including (but not limited to) indications, contraindications, warnings, and precautions. Package inserts for U.S.-licensed vaccines are available at † For adults and older children, the recommended site for intramuscular influenza vaccination is the deltoid muscle. The preferred site for infants and young children is the anterolateral aspect of the thigh. Specific guidance regarding site and needle length for intramuscular administration may be found in the ACIP General Recommendations on Immunization, available at § Available upon request from Sanofi Pasteur (1–800–822–2463 or ¶ Quadrivalent inactivated influenza vaccine, intradermal: a 0.1-mL dose contains 9 µg of each vaccine antigen (36 µg total). ** The preferred injection site is over the deltoid muscle. Fluzone Intradermal Quadrivalent is administered using the delivery system included with the vaccine. †† Age indication per package insert is ≥5 years; however, ACIP recommends Afluria not be used in children aged 6 months through 8 years because of increased risk of febrile reactions noted in this age group with bioCSL's 2010 Southern Hemisphere IIV3. If no other age-appropriate, licensed inactivated seasonal influenza vaccine is available for a child aged 5 through 8 years who has a medical condition that increases the child's risk for influenza complications, Afluria can be used; however, providers should discuss with the parents or caregivers the benefits and risks of influenza vaccination with Afluria before administering this vaccine. Afluria may be used in persons aged ≥9 years. §§ Syringe tip cap may contain natural rubber latex. ¶¶ Information not included in package insert. Estimated to contain <50 femtograms (5x10-8 µg) of total egg protein (of which ovalbumin is a fraction) per 0.5 mL dose of Flucelvax. *** Trivalent inactivated influenza vaccine, high-dose: a 0.5-mL dose contains 60 µg of each vaccine antigen (180 µg total).
 µg/0.5 mL. Ovalbumin. µg/0.5 mL. Age indications. Latex. Route. Inactivated influenza vaccine, cell-culture-based (ccIIV3), standard dose. Contraindications*: Severe allergic reaction to any vaccine component, including egg protein, or after previous dose of any influenza vaccine. Precautions*: Moderate to severe acute illness with or without fever; history of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine. Flucelvax. Novartis Vaccines and Diagnostics. 0.5 mL single-dose prefilled syringe. — ¶¶ ≥18 yrs. Yes§§ IM† Inactivated influenza vaccine, trivalent (IIV3), high dose. Fluzone High-Dose*** Sanofi Pasteur. ≥65 yrs. No. Recombinant influenza vaccine, trivalent (RIV3), standard dose. Contraindications*: Severe allergic reaction to any vaccine component. Precautions*: Moderate to severe acute illness with or without fever; history of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine. Flublok. Protein Sciences. 0.5 mL single-dose vial. Abbreviations: ACIP = Advisory Committee on Immunization Practices; ID = intradermal; IM = intramuscular; IN = intranasal. * Immunization providers should check Food and Drug Administration-approved prescribing information for 2015–16 influenza vaccines for the most complete and updated information, including (but not limited to) indications, contraindications, warnings, and precautions. Package inserts for U.S.-licensed vaccines are available at † For adults and older children, the recommended site for intramuscular influenza vaccination is the deltoid muscle. The preferred site for infants and young children is the anterolateral aspect of the thigh. Specific guidance regarding site and needle length for intramuscular administration may be found in the ACIP General Recommendations on Immunization, available at § Available upon request from Sanofi Pasteur (1–800–822–2463 or ¶ Quadrivalent inactivated influenza vaccine, intradermal: a 0.1-mL dose contains 9 µg of each vaccine antigen (36 µg total). ** The preferred injection site is over the deltoid muscle. Fluzone Intradermal Quadrivalent is administered using the delivery system included with the vaccine. †† Age indication per package insert is ≥5 years; however, ACIP recommends Afluria not be used in children aged 6 months through 8 years because of increased risk of febrile reactions noted in this age group with bioCSL s 2010 Southern Hemisphere IIV3. If no other age-appropriate, licensed inactivated seasonal influenza vaccine is available for a child aged 5 through 8 years who has a medical condition that increases the child s risk for influenza complications, Afluria can be used; however, providers should discuss with the parents or caregivers the benefits and risks of influenza vaccination with Afluria before administering this vaccine. Afluria may be used in persons aged ≥9 years. §§ Syringe tip cap may contain natural rubber latex. ¶¶ Information not included in package insert. Estimated to contain <50 femtograms (5x10-8 µg) of total egg protein (of which ovalbumin is a fraction) per 0.5 mL dose of Flucelvax. *** Trivalent inactivated influenza vaccine, high-dose: a 0.5-mL dose contains 60 µg of each vaccine antigen (180 µg total).")
25
Influenza Vaccines, 2015-2016 Influenza Season cont’d
Trade name Manufacturer Presentation Mercury (from thimerosal) µg/0.5 mL Ovalbumin µg/0.5 mL Age indications Latex Route Live attenuated influenza vaccine, quadrivalent (LAIV4) Contraindications*: Severe allergic reaction to any vaccine component, including egg protein, or after previous dose of any influenza vaccine. Concomitant use of aspirin or aspirin-containing medications in children and adolescents. In addition, ACIP recommends LAIV4 not be used for pregnant women, immunosuppressed persons, persons with egg allergy, and children aged 2 through 4 years who have asthma or who have had a wheezing episode noted in the medical record within the past 12 months, or for whom parents report that a health care provider stated that they had wheezing or asthma within the last 12 months. LAIV4 should not be administered to persons who have taken influenza antiviral medications within the previous 48 hours. Persons who care for severely immunosuppressed persons who require a protective environment should not receive LAIV4, or should avoid contact with such persons for 7 days after receipt. Precautions*: Moderate to severe acute illness with or without fever; history of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine; asthma in persons aged 5 years and older; medical conditions which might predispose to higher risk for complications attributable to influenza. FluMist Quadrivalent††† MedImmune 0.2 mL single-dose prefilled intranasal sprayer — <0.24 (per 0.2 mL) 2 through 49 yrs No IN Abbreviations: ACIP = Advisory Committee on Immunization Practices; ID = intradermal; IM = intramuscular; IN = intranasal. * Immunization providers should check Food and Drug Administration-approved prescribing information for 2015–16 influenza vaccines for the most complete and updated information, including (but not limited to) indications, contraindications, warnings, and precautions. Package inserts for U.S.-licensed vaccines are available at † For adults and older children, the recommended site for intramuscular influenza vaccination is the deltoid muscle. The preferred site for infants and young children is the anterolateral aspect of the thigh. Specific guidance regarding site and needle length for intramuscular administration may be found in the ACIP General Recommendations on Immunization, available at § Available upon request from Sanofi Pasteur (1–800–822–2463 or ¶ Quadrivalent inactivated influenza vaccine, intradermal: a 0.1-mL dose contains 9 µg of each vaccine antigen (36 µg total). ** The preferred injection site is over the deltoid muscle. Fluzone Intradermal Quadrivalent is administered using the delivery system included with the vaccine. †† Age indication per package insert is ≥5 years; however, ACIP recommends Afluria not be used in children aged 6 months through 8 years because of increased risk of febrile reactions noted in this age group with bioCSL's 2010 Southern Hemisphere IIV3. If no other age-appropriate, licensed inactivated seasonal influenza vaccine is available for a child aged 5 through 8 years who has a medical condition that increases the child's risk for influenza complications, Afluria can be used; however, providers should discuss with the parents or caregivers the benefits and risks of influenza vaccination with Afluria before administering this vaccine. Afluria may be used in persons aged ≥9 years. §§ Syringe tip cap may contain natural rubber latex. ††† FluMist is shipped refrigerated and stored in the refrigerator at 35°F–46°F (2°C–8°C) after arrival in the vaccination clinic. The dose is 0.2 mL divided equally between each nostril. Health care providers should consult the medical record, when available, to identify children aged 2 through 4 years with asthma or recurrent wheezing that might indicate asthma. In addition, to identify children who might be at greater risk for asthma and possibly at increased risk for wheezing after receiving LAIV, parents or caregivers of children aged 2 through 4 years should be asked: "In the past 12 months, has a health care provider ever told you that your child had wheezing or asthma?" Children whose parents or caregivers answer "yes" to this question and children who have asthma or who had a wheezing episode noted in the medical record within the past 12 months should not receive FluMist.
 µg/0.5 mL. Ovalbumin. µg/0.5 mL. Age indications. Latex. Route. Live attenuated influenza vaccine, quadrivalent (LAIV4) Contraindications*: Severe allergic reaction to any vaccine component, including egg protein, or after previous dose of any influenza vaccine. Concomitant use of aspirin or aspirin-containing medications in children and adolescents. In addition, ACIP recommends LAIV4 not be used for pregnant women, immunosuppressed persons, persons with egg allergy, and children aged 2 through 4 years who have asthma or who have had a wheezing episode noted in the medical record within the past 12 months, or for whom parents report that a health care provider stated that they had wheezing or asthma within the last 12 months. LAIV4 should not be administered to persons who have taken influenza antiviral medications within the previous 48 hours. Persons who care for severely immunosuppressed persons who require a protective environment should not receive LAIV4, or should avoid contact with such persons for 7 days after receipt. Precautions*: Moderate to severe acute illness with or without fever; history of Guillain-Barré syndrome within 6 weeks of receipt of influenza vaccine; asthma in persons aged 5 years and older; medical conditions which might predispose to higher risk for complications attributable to influenza. FluMist Quadrivalent††† MedImmune. 0.2 mL single-dose prefilled intranasal sprayer. — <0.24 (per 0.2 mL) 2 through 49 yrs. No. IN. Abbreviations: ACIP = Advisory Committee on Immunization Practices; ID = intradermal; IM = intramuscular; IN = intranasal. * Immunization providers should check Food and Drug Administration-approved prescribing information for 2015–16 influenza vaccines for the most complete and updated information, including (but not limited to) indications, contraindications, warnings, and precautions. Package inserts for U.S.-licensed vaccines are available at † For adults and older children, the recommended site for intramuscular influenza vaccination is the deltoid muscle. The preferred site for infants and young children is the anterolateral aspect of the thigh. Specific guidance regarding site and needle length for intramuscular administration may be found in the ACIP General Recommendations on Immunization, available at § Available upon request from Sanofi Pasteur (1–800–822–2463 or ¶ Quadrivalent inactivated influenza vaccine, intradermal: a 0.1-mL dose contains 9 µg of each vaccine antigen (36 µg total). ** The preferred injection site is over the deltoid muscle. Fluzone Intradermal Quadrivalent is administered using the delivery system included with the vaccine. †† Age indication per package insert is ≥5 years; however, ACIP recommends Afluria not be used in children aged 6 months through 8 years because of increased risk of febrile reactions noted in this age group with bioCSL s 2010 Southern Hemisphere IIV3. If no other age-appropriate, licensed inactivated seasonal influenza vaccine is available for a child aged 5 through 8 years who has a medical condition that increases the child s risk for influenza complications, Afluria can be used; however, providers should discuss with the parents or caregivers the benefits and risks of influenza vaccination with Afluria before administering this vaccine. Afluria may be used in persons aged ≥9 years. §§ Syringe tip cap may contain natural rubber latex. ††† FluMist is shipped refrigerated and stored in the refrigerator at 35°F–46°F (2°C–8°C) after arrival in the vaccination clinic. The dose is 0.2 mL divided equally between each nostril. Health care providers should consult the medical record, when available, to identify children aged 2 through 4 years with asthma or recurrent wheezing that might indicate asthma. In addition, to identify children who might be at greater risk for asthma and possibly at increased risk for wheezing after receiving LAIV, parents or caregivers of children aged 2 through 4 years should be asked: In the past 12 months, has a health care provider ever told you that your child had wheezing or asthma Children whose parents or caregivers answer yes to this question and children who have asthma or who had a wheezing episode noted in the medical record within the past 12 months should not receive FluMist.")
26
Which of the following is the predominant flu strain of 2015-16?
Type B strain in trivalent vaccine Type B strain not in trivalent vaccine Type A H1N1 strain Type A H3N2 strain

27
Inactivated Influenza Vaccine (IIV) Quadrivalent Fluarix® Fluzone®
 Quadrivalent Fluarix® Fluzone®")
28
New Influenza Vaccines:
Fluarix ® (GlaxoSmithKline) – inactivated, quadrivalent vaccine which contains two type A and two type B strains FDA approved December 2012 People ages 3 years and older Fluzone ® (Sanofi Pasteur) – inactivated, quadrivalent vaccine which contains two type A and two type B strains FDA approved March 2013 People ages 6 months and older
 – inactivated, quadrivalent vaccine which contains two type A and two type B strains. FDA approved December People ages 3 years and older. Fluzone ® (Sanofi Pasteur) – inactivated, quadrivalent vaccine which contains two type A and two type B strains. FDA approved March People ages 6 months and older.")
29
Quadrivalent Flu Vaccines Facts
A quadrivalent (4-strain) flu vaccine helps to provide protection against four flu virus strains (2 Type A and 2 Type B). 4-strain flu vaccines are made in the same way 3-strain flu vaccines are made. Quadrivalent flu vaccines are available as both shots and intranasal spray.
 flu vaccine helps to provide protection against four flu virus strains (2 Type A and 2 Type B). 4-strain flu vaccines are made in the same way 3-strain flu vaccines are made. Quadrivalent flu vaccines are available as both shots and intranasal spray.")
30
Quadrivalent versus Trivalent Influenza Vaccine
Excerpt from FDA Clinical Review: Fluarix Quadrivalent® Unmet Medical Need: “The B strain recommended for use in the yearly [trivalent] vaccine has been matched to the main circulating influenza B strain only in one-half of the influenza season in the last eight years.

31
2015-2016 Vaccine Coverage: Trivalent versus Quadrivalent
A/California/7/2009 (H1N1)-like virus A/Switzerland/ /2013 (H3N2)- like virus B/Phuket/3073/2013-like virus (Yamagata) Quadrivalent B/Brisbane/60/2008-like virus (Victoria) The flu vaccine's effectiveness may vary depending on age, health, and immune status and how well scientists identity circulating viruses. In , vaccine effectiveness was under 20%. Conclusion: quadrivalent does not provide significantly better coverage this flu season
-like virus. A/Switzerland/ /2013 (H3N2)- like virus. B/Phuket/3073/2013-like virus (Yamagata) Quadrivalent. B/Brisbane/60/2008-like virus (Victoria) The flu vaccine s effectiveness may vary depending on age, health, and immune status and how well scientists identity circulating viruses. In , vaccine effectiveness was under 20%. Conclusion: quadrivalent does not provide significantly better coverage this flu season.")
32
Administration Fluarix®: 0.5-mL dose IM - deltoid
1 inch, 25 gauge needle

33
Quadrivalent Influenza Vaccines contain which of the following?
Four type A strains Two type A strains, 1 type B, & 1 type C Two type A strains & 2 type B strains Four type B strains

34
Live Attenuated Influenza Vaccine (LAIV) Quadrivalent Flumist®
 Quadrivalent Flumist®")
35
New Influenza Vaccines:
Flumist® Quadrivalent (MedImmune)– live attenuated vaccine which contains two type A and two type B strains FDA approved March, 2012 People ages 2 through 49 years
– live attenuated vaccine which contains two type A and two type B strains. FDA approved March, People ages 2 through 49 years.")
36
Live Attenuated Influenza Vaccine
Indication Healthy people 2 through 49 years of age Contraindications Pregnant women People who have long-term health problems with: heart disease kidney or liver disease lung disease metabolic disease, such as diabetes asthma anemia, and other blood disorders Anyone with a weakened immune system Severe egg allergy I pick my nose!

37
Administration Flumist®: 0.1-mL dose in each nostril Intranasal

38
Intranasal Administration
Active inhalation (sniffing) by the patient is not required
 by the patient is not required.")
39
45 yo man with severe egg allergy 27 yo healthy woman
Which of the following patients is a candidate for the live influenza vaccine? 45 yo man with severe egg allergy 27 yo healthy woman 38 yo man with diabetes 54 yo healthy man 19 yo pregnant woman

40
Inactivated Influenza Vaccine (IIV) Trivalent Mammalian Flucelvax®
 Trivalent Mammalian Flucelvax®")
41
New Influenza Vaccines:
Flucelvax® (Novartis)– trivalent inactivated vaccine grown in mammalian cells rather than chicken embryo cells. FDA approved November, 2012 Adults 18 years and older May contain a trace amount of egg protein.
– trivalent inactivated vaccine grown in mammalian cells rather than chicken embryo cells. FDA approved November, Adults 18 years and older. May contain a trace amount of egg protein.")
42
Administration Flucelvax®: 0.5-mL dose IM - deltoid
1 inch, 25 gauge needle

43
Inactivated, Trivalent Recombinant Vaccine Flublok®

44
New Influenza Vaccines:
Flublock® (Protein Sciences Corporation)– trivalent inactivated vaccine grown in insect cells rather than chicken embryo cells. FDA approved November, 2013 Adults 18 years and older. Doesn’t list “severe allergic reaction to egg protein” in the contraindications
– trivalent inactivated vaccine grown in insect cells rather than chicken embryo cells. FDA approved November, Adults 18 years and older. Doesn’t list severe allergic reaction to egg protein in the contraindications.")
45
Administration Flucelvax®: 0.5-mL dose IM - deltoid
1 inch, 25 gauge needle

46
ACIP Recommendations for flu vaccination of person who report egg allergy.

47
Select an influenza vaccine for a healthy 37-year-old woman with severe egg allergy.
Flublok Flumist Fluzone Fluarix

48
High-Dose Inactivated Influenza Vaccine (IIV) Trivalent Fluzone HD®
 Trivalent Fluzone HD®")
49
Why a high-dose influenza vaccine?
Clinical Need 31 studies from 1986 to 2002 found that post-vaccination titers in older adults were 2x to 4x less likely to produce sufficient protection against influenza Vaccine efficacy in a matched season: 70% to 90% in younger adults 17% to 53% in adults aged ≥65 years HD Vaccine Efficacy RCTs and retrospective analyses demonstrate superior efficacy compared to IIV-SD Vaccine efficacy in a matched season among younger adults = est at 70-90% In older adults = est at 17-53% Wang J, Vardeny O, Zorek J. High-dose influenza vaccine in older adults. JAPhA. 2016; 56:95-97.

50
Methods: Retrospective cohort study
Lancet Infect Dis 2015;15: Methods: Retrospective cohort study HD vaccine (60 mcg of hemagglutinin per strain): N= 929,730 SD vaccine (15 mcg of hemagglutinin per strain): : N= 1,615,545 US Medicare beneficiaries 65 years and older who received influenza vaccine in a community pharmacy Primary outcome: probable episode of influenza-related illness defined by a community medical encounter with the provision of a rapid influenza test followed by dispensing of oseltamivir within a 2-day period
: N= 929,730. SD vaccine (15 mcg of hemagglutinin per strain): : N= 1,615,545. US Medicare beneficiaries 65 years and older who received influenza vaccine in a community pharmacy. Primary outcome: probable episode of influenza-related illness defined by a community medical encounter with the provision of a rapid influenza test followed by dispensing of oseltamivir within a 2-day period.")
51
Izurieta_2015_Lancet Infect Dis
How well does the study design limit bias? Who was enrolled in the study/who does the study apply to? What is the primary outcome, how was it measured and is the result statistically significant? What can we infer from these findings? Is the result clinically significant?

52
Efficacy of HD Vaccine versus SD Vaccine Against Influenza-Related Illness
Similar results to Diazgranados et al. Those who received IIV-HD 22% less likely to have influenza-associated illness and 22% less likely to be admitted to the hospital for influenza Each plot displays the rate of influenza per person-weeks. Data was smoothed using a weighted average, placing a weight of 0・5 on the current week and a weight of 0・25 on the previous and following weeks. (A) Rapid infl uenza test followed by treatment with oseltamivir. (B) Inpatient hospital admissions or emergency department visits with an infl uenza International Classifi cation of Diseases, ninth revision, Clinical Modifi cation code. RIT=rapid infl uenza diagnostic test. Lancet Infect Dis 2015;15:
 Rapid. infl uenza test followed by treatment with oseltamivir. (B) Inpatient hospital admissions or emergency department. visits with an infl uenza International Classifi cation of Diseases, ninth revision, Clinical Modifi cation code. RIT=rapid. infl uenza diagnostic test. Lancet Infect Dis 2015;15:")
53
Conclusions: IIV-HD versus -SD
Safety Injection site reactions have been reported at higher rates for IIV-HD, though most cases were mild and resolved within several days A 2015 study showed IIV-HD results in fewer serious complications Cost Cost to administer is $19.75 higher than IIV-SD per individual A 2015 cost-utility analysis demonstrated a 587% financial return for the health care system alone (cost savings in the millions of dollars) Implications for Pharmacists ACIP makes no recommendation for one influenza vaccine formulation over another for older adults Regardless of which formulation is recommended, be sure it is received in a timely manner so your patients have the best possible flu protection JAPhA. 2016; 56:95-97.
 Implications for Pharmacists. ACIP makes no recommendation for one influenza vaccine formulation over another for older adults. Regardless of which formulation is recommended, be sure it is received in a timely manner so your patients have the best possible flu protection. JAPhA. 2016; 56:")
54
Administration Fluzone HD®: 0.5-mL dose IM - deltoid
1 inch, 25 gauge needle

55
Intradermal Inactivated Influenza Vaccine (IIV) Fluzone Intradermal®
 Fluzone Intradermal®")
56
Intradermal Influenza Vaccine
Indicated for persons 18 through 64 years of age Contraindications Severe egg allergy Associated with higher rates of injection site reactions (erythema, induration, swelling, and pruritus, but not pain) than the IM inactivated influenza vaccines Erythema (>75%) Induration (>50%) Swelling (>50%) Pain (>50%) Pruritus (>40%)
 than the IM inactivated influenza vaccines. Erythema (>75%) Induration (>50%) Swelling (>50%) Pain (>50%) Pruritus (>40%)")
57
Intradermal vs Traditional IM needle Length

58
30 Gauge Needle and Less Volume

59
Methods: Multicenter, randomized, double-blind controlled study
ID vaccine (9 mcg of hemagglutinin per strain) N=1,803 IM vaccine (15 mcg of hemagglutinin per strain): N=452 in adults 18 to 60 years of age. Human Vaccines. 2010;6:
 N=1,803. IM vaccine (15 mcg of hemagglutinin per strain): N=452. in adults 18 to 60 years of age. Human Vaccines. 2010;6:")
60
Comparison of local side effects to ID and IM influenza vaccine
Percent Human Vaccines. 2010;6:

61
Intradermal Injection Technique
Remove needle cap Hold microinjection system between thumb and middle finger Do not place fingers on the windows Insert needle rapidly perpendicular to the skin Inject using the index finger Remove needle from the skin and activate the needle shield by pushing firmly on the plunger

62
Injection site swelling Malaise
Which side effect is more common with the intradermal influenza vaccine than the IM influenza vaccine? Injection site pain Headache Fever Injection site swelling Malaise

63
Influenza Vaccines: Summary

64
Age Indication for Influenza Vaccines: United States, 2015-2016
0.5-2 years 2 years 3 4-8 9-17 18-49 years 50-64 years 65+ Fluzone / Fluzone Quad ✓ Flumist Quad Fluarix Quad FluLaval Quad Fluvirin Afluria1 Flucelvax Flublok2 Fluzone Intradermal Quad Fluzone High-Dose Age indication per package insert is >5 years; however the ACIP recommends >9 years. FDA labeled age indication expanded in 2015 to 18 years and older (now including adults 65+).
.")
65
Characteristics of Influenza Vaccines: United States, 2015-2016
Live Mercury Egg Protein Latex Fluzone / Fluzone Quad ✓1 ✓ Flumist Quad Fluarix Quad FluLaval Quad Fluvirin ✓3 Afluria Flucelvax ✓2 Flublok Fluzone Intradermal Quad Fluzone High-Dose Multi-dose vials contain mercury. Single-dose prefilled syringes are mercury-free. Estimated to contain <50 femtograms (5x10-8 mcg) of total egg protein per 0.5 ml dose. Syringe tip may contain natural rubber latex.
 of total egg protein per 0.5 ml dose. Syringe tip may contain natural rubber latex.")
66
Inactivated trivalent IM vaccine Inactivated quadrivalent vaccine
Which of the following influenza vaccines is NOT indicated for a 72-year old woman? Inactivated trivalent IM vaccine Inactivated quadrivalent vaccine Inactivated high dose vaccine Inactivated trivalent intradermal vaccine

67
Influenza intradermal vaccine Influenza intramuscular vaccine
A 35-year-old woman requests an annual flu shot. She has ulcerative colitis and is taking Prednisone 40 mg QD. Which flu vaccine(s) is/are appropriate? Influenza intradermal vaccine Influenza intramuscular vaccine Influenza high dose vaccine Flumist nasal spray 0.2 ml nasal Either 1 or 2 Either 2 or 3 Either 2 or 4
 is/are appropriate Influenza intradermal vaccine. Influenza intramuscular vaccine. Influenza high dose vaccine. Flumist nasal spray 0.2 ml nasal. Either 1 or 2. Either 2 or 3. Either 2 or 4.")
68
Pneumococcal Vaccine PPSV23 / Pneumovax® PCV13 / Pnevnar®

69
Pneumococcal Disease Complex immunization recommendation for adults
Pneumococcal disease is caused the bacterium Streptococcus pneumoniae Clinical Features Pneumonia Otitis media Sinus infections Bacteremia Meningitis Risk Factors Asplenia Chronic heart, pulmonary, liver, or renal disease Cigarette smoking Cerebrospinal fluid leak Age less than 2 years, or 65 years and older Complex immunization recommendation for adults There are different types of pneumococcal disease, such as lung infections (pneumococcal pneumonia), blood infections (bacteremia), infections of the covering of the brain and spinal cord (pneumococcal meningitis), and middle ear infections (otitis media). Pneumococcal disease is a leading cause of vaccine-preventable illness and death in the United States. Pneumonia is the most common presentation of pneumococcal disease among adults – incubation of pneumonia is 1-3 days – it is characterized by abrupt onset of fever, rigors, chills, pleuritic chest pain, productive cough, dyspnea, tachypnea, hypoxia and diagnosed by x-ray imaging and symptoms However, calling the pneumococcal vaccine the “pneumonia vaccine” can be misleading – one of the greatest benefits of receiving the pneumococcal vaccine is the protection against invasive pneumococcal disease, or “IPD” such as bacteremia or meningitis. The term “invasive” refers to infection of an area of the body that is normally bacteria free – such as the blood stream or the cerebrospinal fluid
, blood infections (bacteremia), infections of the covering of the brain and spinal cord (pneumococcal meningitis), and middle ear infections (otitis media). Pneumococcal disease is a leading cause of vaccine-preventable illness and death in the United States. Pneumonia is the most common presentation of pneumococcal disease among adults – incubation of pneumonia is 1-3 days – it is characterized by abrupt onset of fever, rigors, chills, pleuritic chest pain, productive cough, dyspnea, tachypnea, hypoxia and diagnosed by x-ray imaging and symptoms. However, calling the pneumococcal vaccine the pneumonia vaccine can be misleading – one of the greatest benefits of receiving the pneumococcal vaccine is the protection against invasive pneumococcal disease, or IPD such as bacteremia or meningitis. The term invasive refers to infection of an area of the body that is normally bacteria free – such as the blood stream or the cerebrospinal fluid.")
70
Streptococcus Pneumoniae
90 serotypes identified The 10 most common serotypes are estimated to account for about 62% of invasive disease worldwide Up to 36% of adult CAP Up to 50% of HAP 13-19% of all cases of meningitis lancet shaped gram-positive, facultative anaerobic bacteria. Observed in pairs, or in short chains. Encapsulated organisms are pathogenic Common inhabitants of the respiratory tract – 5-70% of adults CDC: Vaccines and Immunizations. Pneumococcal Disease. Accessed 30 July 2014.

73
Pneumococcal Vaccines
Pneumovax 23® (PPSV23, pneumococcal polysaccharide vaccine) Prevnar 13® (PCV13, pneumococcal conjugate vaccine) Pneumococcal polysaccharide vaccine is composed of purified preparations of pneumococcal capsular polysaccharide. The first polysaccharide pneumococcal vaccine was licensed in the United States in It contained purified capsular polysaccharide antigen from 14 different types of pneumococcal bacteria. In 1983, a 23-valent polysaccharide vaccine (PPSV23) was licensed and replaced the 14-valent vaccine, which is no longer produced. PPSV23 contains polysaccharide antigen from 23 types of pneumococcal bacteria that cause 88% of bacteremic pneumococcal disease. In addition, cross-reactivity occurs for several capsular types that account for an additional 8% of bacteremic disease. The polysaccharide vaccine currently available in the United States (Pneumovax 23, Merck) contains 25 mcg of each antigen per dose and contains 0.25% phenol as a preservative. The vaccine is available in a single-dose vial or syringe, and in a 5-dose vial. Pneumococcal vaccine is given by injection and may be administered either intramuscularly or subcutaneously. The first pneumococcal conjugate vaccine (PCV7) was licensed in the United States in It includes purified capsular polysaccharide of seven serotypes of S. pneumoniae (4, 9V, 14, 19F, 23F, 18C, and 6B) conjugated to a nontoxic variant of diphtheria toxin known as CRM197. In 2010 a 13-valent pneumococcal conjugate vaccine (PCV13) was licensed in the United States. It contains the 7 serotypes of S pneumonia as PCV7 plus serotypes 1, 3, 5, 6A, 7F and 19A which are also conjugated to CRM197. A 0.5-mL PCV13 dose contains approximately 2.2 µg of polysaccharide from each of 12 serotypes and approximately 4.4 μg of polysaccharide from serotype 6B; the total concentration of CRM197 is approximately 34 µg. The vaccine contains 0.02% polysorbate 80 (P80), mg of aluminum as aluminum phosphate (AlPO4) adjuvant, 5mL of succinate buffer, and no thimerosal preservative. Except for the addition of six serotypes, P80, and succinate buffer, the formulation of PCV13 is the same as that of PCV7. ABCs data indicate that in 2008, a total of 61% of invasive pneumococcal disease cases among children younger than 5 years were attributable to the serotypes included in PCV13, with serotype 19A accounting for 43% of cases; PCV7 serotypes caused less than 2% of cases.
 Prevnar 13® (PCV13, pneumococcal conjugate vaccine) Pneumococcal polysaccharide vaccine is composed of purified preparations of pneumococcal capsular polysaccharide. The first polysaccharide pneumococcal vaccine was licensed in the United States in It contained purified capsular polysaccharide antigen from 14 different types of pneumococcal bacteria. In 1983, a 23-valent polysaccharide vaccine (PPSV23) was licensed and replaced the 14-valent vaccine, which is no longer produced. PPSV23 contains polysaccharide antigen from 23 types of pneumococcal bacteria that cause 88% of bacteremic pneumococcal disease. In addition, cross-reactivity occurs for several capsular types that account for an additional 8% of bacteremic disease. The polysaccharide vaccine currently available in the United States (Pneumovax 23, Merck) contains 25 mcg of each antigen per dose and contains 0.25% phenol as a preservative. The vaccine is available in a single-dose vial or syringe, and in a 5-dose vial. Pneumococcal vaccine is given by injection and may be administered either intramuscularly or subcutaneously. The first pneumococcal conjugate vaccine (PCV7) was licensed in the United States in It includes purified capsular polysaccharide of seven serotypes of S. pneumoniae (4, 9V, 14, 19F, 23F, 18C, and 6B) conjugated to a nontoxic variant of diphtheria toxin known as CRM197. In 2010 a 13-valent pneumococcal conjugate vaccine (PCV13) was licensed in the United States. It contains the 7 serotypes of S pneumonia as PCV7 plus serotypes 1, 3, 5, 6A, 7F and 19A which are also conjugated to CRM197. A 0.5-mL PCV13 dose contains approximately 2.2 µg of polysaccharide from each of 12 serotypes and approximately 4.4 μg of polysaccharide from serotype 6B; the total concentration of CRM197 is approximately 34 µg. The vaccine contains 0.02% polysorbate 80 (P80), mg of aluminum as aluminum phosphate (AlPO4) adjuvant, 5mL of succinate buffer, and no thimerosal preservative. Except for the addition of six serotypes, P80, and succinate buffer, the formulation of PCV13 is the same as that of PCV7. ABCs data indicate that in 2008, a total of 61% of invasive pneumococcal disease cases among children younger than 5 years were attributable to the serotypes included in PCV13, with serotype 19A accounting for 43% of cases; PCV7 serotypes caused less than 2% of cases.")
75
ACIP Recommendations on Pneumococcal Vaccinations in Adults

76
PPSV23 (Pneumovax®) Age Who receives the vaccine? ≥65 years old
Vaccination history unclear or never received vaccine before Revaccinate: If patient received vaccine before the age of 65 and it has been ≥ 5 years since administration 2-64 years old Chronic cardiovascular disease (CHF, cardiomyopathies) Chronic pulmonary disease (COPD) Diabetes mellitus Alcoholism Chronic liver disease Cerebrospinal fluid leaks Re-vaccination after 5 years if: functional or anatomic asplenia Immunocompromising conditions Chronic kidney disease 19-64 years old Cigarette smokers Asthma immunocompromising conditions: HIV, leukemia, hodgkins, malignancy, renal failure, nephrotic syndrome, chemotherapy, corticosteroids, organ or bone marrow transplant
 Chronic pulmonary disease (COPD) Diabetes mellitus. Alcoholism. Chronic liver disease. Cerebrospinal fluid leaks. Re-vaccination after 5 years if: functional or anatomic asplenia. Immunocompromising conditions. Chronic kidney disease years old. Cigarette smokers. Asthma. immunocompromising conditions: HIV, leukemia, hodgkins, malignancy, renal failure, nephrotic syndrome, chemotherapy, corticosteroids, organ or bone marrow transplant.")
77
PCV13 (Prevnar®) Age Who receives the vaccine?
6 weeks through 5 years old Routine series at 2, 4, 6, and 12 through 15 months. Minimum intervals: Dose 1 to Dose 2: 4 weeks Dose 2 to Dose 3: 4 weeks Dose 3 to Dose 4: 8 weeks 6-18 years old Children 6 through 18 years who have not received PCV13 previously, and are at high risk for invasive pneumococcal disease because of: Anatomic or functional asplenia (including sickle cell disease) Immunocompromising conditions, including HIV infection Cochlear implant CSF leaks should receive a single dose of PCV13 (regardless of any previous history of PCV7 and/or PPSV23). Contraindications and Precautions PCV13 is contraindicated for people who have had an anaphylactic reaction to a diphtheria-toxoid containing vaccine, because the antigens in PCV13 are conjugated to diphtheria CRM197 protein. PCV13 is contraindicated for anyone with a history of anaphylactic hypersensitivity to any vaccine component. For a list of PCV13 vaccine contents, see the package insert or the vaccine excipient table[4 pages]( PCV13 packaging does not contain latex. "The presence of a moderate or severe acute illness with or without a fever is a precaution to administration of all vaccines." (ACIP General Recommendations on Immunization, p.11) (The definition of "moderate or severe acute illness" is left up to the clinical judgment of the provider.)
 Immunocompromising conditions, including HIV infection. Cochlear implant. CSF leaks. should receive a single dose of PCV13 (regardless of any previous history of PCV7 and/or PPSV23). Contraindications and Precautions. PCV13 is contraindicated for people who have had an anaphylactic reaction to a diphtheria-toxoid containing vaccine, because the antigens in PCV13 are conjugated to diphtheria CRM197 protein. PCV13 is contraindicated for anyone with a history of anaphylactic hypersensitivity to any vaccine component. For a list of PCV13 vaccine contents, see the package insert or the vaccine excipient table[4 pages]( PCV13 packaging does not contain latex. The presence of a moderate or severe acute illness with or without a fever is a precaution to administration of all vaccines. (ACIP General Recommendations on Immunization, p.11) (The definition of moderate or severe acute illness is left up to the clinical judgment of the provider.)")
78
PCV13 (Prevnar®), cont’d Age Who receives the vaccine? Adults 19
years old and older Adults 19 and older who have not received either PCV or PPSV previously, and are at high risk for invasive pneumococcal disease because of: Anatomic or functional asplenia (including sickle cell disease) Immunocompromising conditions, including HIV infection Cochlear implant CSF leaks should receive a single dose of PCV13. (This should be followed with a dose of PPSV at least 8 weeks later. Those who have indications for revaccination with PPSV should receive a second dose at least 5 years after the first.) Adults 19 and older with any of these conditions who have received one or more doses of PPSV previously should receive a single dose of PCV13 at least one year after the last dose of PPSV. [Note that use of PCV13 for persons 18 through 49 years of age, while recommended by ACIP in these circumstances, is off-label.] Appropriate intervals between doses of PCV and PPSV can be found in PCV MMWR (for children) and PSV MMWR (for adults). Contraindications and Precautions PCV13 is contraindicated for people who have had an anaphylactic reaction to a diphtheria-toxoid containing vaccine, because the antigens in PCV13 are conjugated to diphtheria CRM197 protein. PCV13 is contraindicated for anyone with a history of anaphylactic hypersensitivity to any vaccine component. For a list of PCV13 vaccine contents, see the package insert or the vaccine excipient table[4 pages]( PCV13 packaging does not contain latex. "The presence of a moderate or severe acute illness with or without a fever is a precaution to administration of all vaccines." (ACIP General Recommendations on Immunization, p.11) (The definition of "moderate or severe acute illness" is left up to the clinical judgment of the provider.)
 Immunocompromising conditions, including HIV infection. Cochlear implant. CSF leaks. should receive a single dose of PCV13. (This should be followed with a dose of PPSV at least 8 weeks later. Those who have indications for revaccination with PPSV should receive a second dose at least 5 years after the first.) Adults 19 and older with any of these conditions who have received one or more doses of PPSV previously should receive a single dose of PCV13 at least one year after the last dose of PPSV. [Note that use of PCV13 for persons 18 through 49 years of age, while recommended by ACIP in these circumstances, is off-label.] Appropriate intervals between doses of PCV and PPSV can be found in PCV MMWR (for children) and PSV MMWR (for adults). Contraindications and Precautions. PCV13 is contraindicated for people who have had an anaphylactic reaction to a diphtheria-toxoid containing vaccine, because the antigens in PCV13 are conjugated to diphtheria CRM197 protein. PCV13 is contraindicated for anyone with a history of anaphylactic hypersensitivity to any vaccine component. For a list of PCV13 vaccine contents, see the package insert or the vaccine excipient table[4 pages]( PCV13 packaging does not contain latex. The presence of a moderate or severe acute illness with or without a fever is a precaution to administration of all vaccines. (ACIP General Recommendations on Immunization, p.11) (The definition of moderate or severe acute illness is left up to the clinical judgment of the provider.)")
79
ACIP Recommendations on Pneumococcal Vaccinations in Adults
Both PCV13 and PPSV23 should be administered routinely in series to all adults aged ≥ 65 years. Pneumococcal vaccine-naïve persons. Adults aged ≥65 years who have not previously received pneumococcal vaccine or whose previous vaccination history is unknown should receive a dose of PCV13 first, followed by a dose of PPSV23. The dose of PPSV23 should be given 6–12 months after a dose of PCV13. If PPSV23 cannot be given during this time window, the dose of PPSV23 should be given during the next visit. The two vaccines should not be coadministered, and the minimum acceptable interval between PCV13 and PPSV23 is 8 weeks. MMWR September 19, 2014 / 63 (37)
")
80
Pneumococcal vaccine-naïve persons aged > 65 years
*minimum interval between sequential administration of PCV13 and PPSV23 is 8 weeks; PPSV23 can be given later than 6-12 months after PCV13 if this window is missed.

81
Persons who previously received PPSV23 at age > 65 years
*minimum interval between sequential administration of PCV13 and PPSV23 is 8 weeks; PPSV23 can be given later than 6-12 months after PCV13 if this window is missed.

82
Persons who previously received PPSV23 before age 65 years who are now aged > 65 years

83
Administration Pneumovax® & Prevnar®: 0.5 mL dose
1 inch, 25 gauge needle Intramuscular (IM) - deltoid CDC: Vaccines and Immunizations. Pneumococcal Disease. Accessed 30 July 2014.
 - deltoid. CDC: Vaccines and Immunizations. Pneumococcal Disease. Accessed 30 July")
84
What is the Healthy People 2020 goal for pneumococcal vaccination for adults 65 and older?
100% 90% 70% 50%

85
A 65-year-old man who is pneumonia vaccine naïve
A 65-year-old man who is pneumonia vaccine naïve. What pneumonia vaccine(s) is/are recommended? Pneumovax only Prevnar only Both; Pneumovax prior to Prevnar Both; Prevnar prior to Pneumovax
 is/are recommended Pneumovax only. Prevnar only. Both; Pneumovax prior to Prevnar. Both; Prevnar prior to Pneumovax.")
86
Same day, opposite arm, separate syringe
Which of the following statements about the administration of influenza and pneumonia vaccines is true? Same day, opposite arm, separate syringe Same day, same arm, mixed in 1 syringe Must be separated by at least 7 days Must be separated by at least 4 weeks

87
Which of the following vaccines is a live vaccine?
Pneumovax Flumist Prevnar Fluarix Fluzone HD

88
Questions and Discussion

89
Pathogen (Common name) Table
Classification Transmission Complication Influenza (flu) virus Respiratory Pneumonia Pneumococcus Gram + Bacteria Meningitis/Bacteremia Varicella (chicken pox) Bacterial infection Zoster (shingles) Latent varicella Neuralgia HPV (genital warts) Sexual contact Cervical cancer Meningococcus Gram - Bacteria Invasive disease Tetanus (lockjaw) Gram + Bacteria-toxin wound Respiratory failure Diphtheria Myocarditis/Neuritis Pertussis (whooping cough) Measles Diarrhea, pneumonia Mumps Meningitis Rubella Arthritis Hepatitis A Fecal-oral Acute/chronic hepatitis Hepatitis B Blood-serous fluids Acute hepatitis
 virus. Respiratory. Pneumonia. Pneumococcus. Gram + Bacteria. Meningitis/Bacteremia. Varicella (chicken pox) Bacterial infection. Zoster (shingles) Latent varicella. Neuralgia. HPV (genital warts) Sexual contact. Cervical cancer. Meningococcus. Gram - Bacteria. Invasive disease. Tetanus (lockjaw) Gram + Bacteria-toxin. wound. Respiratory failure. Diphtheria. Myocarditis/Neuritis. Pertussis (whooping cough) Measles. Diarrhea, pneumonia. Mumps. Meningitis. Rubella. Arthritis. Hepatitis A. Fecal-oral. Acute/chronic hepatitis. Hepatitis B. Blood-serous fluids. Acute hepatitis.")
90
Adult Vaccine Table Vaccine Vaccine Type Route / Reconstitute Series
Storage Influenza IIV Inactivated IM / No 1x annually Fridge Flumist Live Intranasal / No Pneumovax IM or SQ / No 1-2 doses Zostavax SQ / Yes 1 dose Freezer Gardasil (HPV9) Cervarix (HPV2) 3 doses Td 1 q 10 years Tdap 1x, then Td Varivax 2 doses MMR Fridge or Freezer Menactra, Menveo Menomune (MPSV4) 1-2+ doses Havrix, Vaqta Recombivax-HB Engerix-B
 Cervarix (HPV2) 3 doses. Td. 1 q 10 years. Tdap. 1x, then Td. Varivax. 2 doses. MMR. Fridge or Freezer. Menactra, Menveo. Menomune (MPSV4) 1-2+ doses. Havrix, Vaqta. Recombivax-HB. Engerix-B.")
Similar presentations