Download presentation
Presentation is loading. Please wait.

1
NEONATAL SEPSIS Dr.Sayid.,MD. Dept.Paediatrics Dept.of Paediatrics

2
What is neonatal sepsis?
Welcome !! What is neonatal sepsis? Definition Causes What will I learn? Symptoms Diagnosis Treatments Summary

3
DEFINITION CLINICAL SYNDROME OF BACTERAEMIA CHARECTERIZED BY SYSTEMIC SIGNS AND SYPMTOMS OF INFECTION IN THE FIRST FOUR WEEKS OF LIFE.

4
What is Neonatal Sepsis?
When pathogenic bacteria gain access into the blood stream, they may cause overwhelming infection without much localization (septicemia) or may get predominantly localized to the lung (pneumonia) or the meninges (meningitis). Arthritis.osteomylitis,and UTI. Exception conjunctivitis and oral thrush.
 or may get predominantly localized to the lung (pneumonia) or the meninges (meningitis). Arthritis.osteomylitis,and UTI. Exception conjunctivitis and oral thrush.")
5
More facts about Neonatal Sepsis
Neonatal Sepsis affects approximately 1- 2 infants per 1000 births with a higher incidence in premature & low birth weight infants. Incidence in India 30/1000(NNPD)
")
6
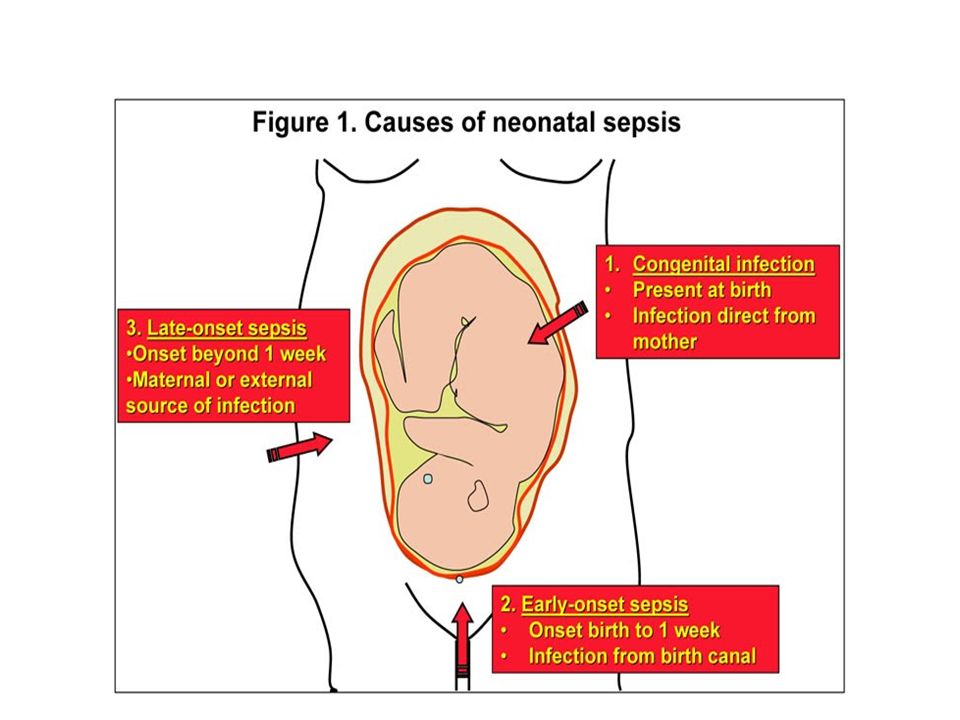
CLASSIFICATION Early onset <72 hours (RD,Pneumonia)
Late onset >72 hours nosocomial, (Septicemia .pneumonia or meningitis)
")
7
RISK FACTORS LBW OR PREMATURITY ILLNES 2 WEEKS PRIOR TO DELIVERY
FOULSMELLING/MECONIUM LIQUOR RUPTURE OF MEMBRANE>24HRS PROLONGED LABOR.24HRS ASPHYXIA SINGLE/UNCLEAN OR>3 STERILE P/V- MECHANICAL VENTILATION,IP,IVF,

9
Causes of Neonatal Sepsis
E.coli, Staphylococcus,Klebsiella and Group Beta Strep (GBS). neonates are more susceptible coz Immature immune response Genetic predisposition
. neonates are more susceptible coz Immature immune response. Genetic predisposition.")
10
What makes a neonate’s immune system immature?
Normally an immune system responds to a pathogen in a specific manner, but if there are problems with any element the immune system is unable to function properly Pathogen enters body Neutrophils move in Chemotaxis occurs Opsonization causes phagocytosis Monocytes kill pathogen

11
Neutrophils: An important cell in immunity against pathogens
Neonatal neutrophils are deficient in their ability to adhere to vessel walls at site of infection and have a decreased ability to “deform” & migrate into tissues Red Blood Cells Neutrophils I

12
Chemotaxis Neonatal neutrophils have decreased chemotaxis due to
decreased chemoattractant . Chemoattractants attract neutrophils to the site of infection .

13
Opsonization Neonates have a decreased amount of opsonins (antibodies that promote opsonization) Opsonization Pathogen

14
Monocytes: Another important cell in the fight against pathogens
Monocytes are deficient which are another main cells in fighting infection I

15
What makes a neonate’s immune system susceptible to sepsis?
OR Maturity Immaturity

16
You’re Right!!!! The immaturity of a neonate’s immune system makes them MORE SUSCEPTIBLE to sepsis.

17
Genetic Role Polymorphisms cause either an over expression or under expression of proteins and/or genes that have significant roles in the immune response to infection. This alters their ability to properly function which makes a neonate more susceptible to sepsis.

18
CLINICAL FEATURES

19
SUBTLE/NON SPECIFIC HYPOTHERMIA OR FEVER LETHERGY/POOR CRY.REFUSAL OF FEED POOR PERFUSION CRT>3sec. HYPOTONIA WEAK OR ABSENT NNR BRADY/TACHYCARDIA RD,APNEA,GASPING RESPIRATION HYPO/HYPERGLYCEMIA & ACIDOSIS

20
A CASE OF SEPSIS

21
heart rate changes tachypnea
SYSTEMIC FEATURES The symptoms of neonatal sepsis are not concrete and vary widely heart rate changes tachypnea hypotension DOB,Grunting shock cyanosis feed intolerance vomiting / diarrhea DIC abd. Distension bleeding NEC petechia/purpura hepatomegaly jaundice umbilical redness/discharge ARF sclerema irritability mottling high pitched cry,vacant stare pustule,abscess bulging AF,seizures stupor/coma

22
A Case of Septicemia

23
A CASE OF NEONATAL MENINGITIS

24
Inflammation in Neonatal Sepsis
It occurs because of an exaggerated systemic inflammatory response . Let’s find out how this is true Inflammatory Process

25
Inflammatory Process Pathogen enters body Inflammatory mediators
released (cytokines) Injury to endothelium Tissue factors released Production of thrombin Increased activity of fibrinolysis inhibitors Coagulation promotes clot formation Decreased fibrinolysis
 Injury to endothelium. Tissue factors released. Production of thrombin. Increased activity of. fibrinolysis inhibitors. Coagulation promotes. clot formation. Decreased fibrinolysis.")
26
Inflammation Overall, the imbalance among inflammation, over coagulation, and decreased fibrinolysis are the cause for the majority of deaths in sepsis.

27
How is Neonatal Sepsis Diagnosed?
There is no definite marker in neonatal sepsis, but there are determinants of infection. * Blood & Urine cultures * Septic screen: Complete Blood Count and DLC * Lumbar Puncture (LP) * Radiology CXR,Neurosonogram,CT * Line cultures
 * Radiology CXR,Neurosonogram,CT * Line cultures")
28
Sepsis screen CBC: white blood cell count and differential count.
Leukopenia <5000mm3 An absolute neutrophil count of < 1800 per cmm Neutropenia Immature neutrophils (Band cells + myelocytes + metamyelocytes) to total neutrophils ratio (l/T) > 0.20
 to total neutrophils ratio (l/T) >")
29
Thrombocytopenia, Toxic granules on peripheral smear and Gastric aspirate smears showing more than 5 Polymorphs per high power field Elevated micro- ESR->15mm in 1st hour CRP-Positive >1mg/dl

30
NORMAL CSF IN NEONATES TERM PRETERM WBC /cmm upto 30 upto 90
Polymorphs % % Protein mg/dl Upto Glucose mg/dl

31
BAND FORM

33
Is there a diagnostic marker for neonatal sepsis?
True False

34
Yeah!!! You are correct! There is NOT a specific diagnostic marker, only determinants of infection (labs, x-rays).
.")
35
Treatments for Neonatal Sepsis
It is of vital importance that treatment is initiated as soon as sepsis is suspected, especially for those infants at risk. Why????

36
Why is it so important to start antibiotic treatment?
If not treated as soon as sepsis is suspected a neonate is more likely to die from sepsis and it’s complications.

37
INDICATIONS FOR ANTIBIOTICS
Presence of >3 risk factors Presence of foul smelling liqour Presence of 2 antenatal risk factors &positive septic screen Strong clinical suspicion of sepsis

38
ANTIMICROBIAL THERAPY
Septicemia or Pneumonia 1 st line; Inj Ampicillin 50 mg/kg/dose 7-10 days / Inj Cloxacillin 50 mg/kg/ dose 7-10 days + InjGentamicin 2.5mg/kg/dose 7-10 days / Inj Amikacin 7.5 mg/kg/dose 7-10 days 3rd line drugs for resistant strains CEFOTAXIME OR PIPERACILLIN-TAZOBCTAM AMIKACIN

39
ANTIMICROBIAL THERAPY
I. Meningitis with or without positive blood/CSF C/S (1) Inj Ampicillin 100 mg/kg/ dose 3 weeks Inj Gentamicin 2.5 mg/ kg/dose 3 weeks Add cefotaxime II. Blood Culture positive,but no meningitis. (2) Inj Cefotaxime 50 mg/kg/ dose 2 weeks Inj Gentamicin 2.5 mg/kg/ dose 2 weeks III.Culture and sepsis screen negative,but clinical course compatible; continue 5-7 days.
 Inj Ampicillin 100 mg/kg/ dose 3 weeks. Inj Gentamicin 2.5 mg/ kg/dose 3 weeks. Add cefotaxime. II. Blood Culture positive,but no meningitis. (2) Inj Cefotaxime 50 mg/kg/ dose 2 weeks. Inj Gentamicin 2.5 mg/kg/ dose 2 weeks. III.Culture and sepsis screen negative,but clinical course compatible; continue 5-7 days.")
40
SUPPORTIVE CARE Thermoneutral environment Establish IV line
Correct SHOCK Correct hypoglycemia Vitamin K If cardiopulmonary compromise- CPR Exchange transfusion in case of sclerema

41
DURATION OF ANTIBIOTICS
if baby appears ill with negative culture,sepsis screen positive ;Antibiotic should be continued for 7-10 days Deep-seated infections (osteomyelitis) may require therapy for 3-6 weeks.
 may require therapy for 3-6 weeks.")
42
Superficial infections :local application of antimicrobial agents
Superficial infections :local application of antimicrobial agents. Pustules can be punctured with sterile needles and cleaned with spirit or betadine . Purulent conjunctivitis : neosporin or chloramphenicol ophthalmic drops. Oral thrush : local application of clotrimazole or nystatin (200,000 units per ml) and hygienic precautions
 and hygienic precautions")
43
Prevention of infections
A good antenatal care Tetanus toxoid to mother. Any infection in antenatal period to be diagnosed early and treated early. Exclusive breast feeding for 6m. Cord care. Hand washing

44
Prevention of infection in hospital
The nursery environment should be clean and dry with 24 hour water supply and electricity. adequate ventilation and lighting. temperature to be maintained between Overcrowding to be avoided Aseptic precautions

45
Unnecessary invasive interventions should be kept to the barest minimum.
use of disposables. Stock solutions to be avoided. separate thermometer and stethoscope and all barrier nursing measures for each baby

46
Strict house-keeping routines for washing, disinfection, cleaning of cots and incubators should be ensured and these policy guidelines should be available in the form of a manual in the nursery. The use of prophylactic antibiotics for prevention of nosocomial infections is strongly condemned. They are not only useless but also dangerous because of the potential risk of emergence of resistant strains of bacteria.

47
PROPHYLACTIC ANTIBIOTICS
EXCHANGE TRANSFUSION VENITILATED NEONATES

48
RESERVE ANTIOBIOTICS AZTREONAM against Gram negative organism
MEROPENEM most bacterial pathogen except MRSA and Enterococcus IMEPENEM _generaly avoided—seizures VANCOMYCIN /CIPROFLOXACIN WITH AMIKACIN for MRSA and ENTEROCOCUS

49
ADJUNCTIVE THERAPY EXCHANGE TRANSFUSION NO ROLE IVIg.
GM-CSF under trial.

50
SUMMARY In conclusion, manifestations of neonatal sepsis are non-specific. A high index of suspicion with or without lab evidences of infection is the key for early diagnosis. Prompt institution of antibiotic therapy and supportive care will save most of the cases of neonatal sepsis.

51
I hope you have enjoyed your experience and have learned some new information about neonatal sepsis.

Similar presentations


>")

















 LECTURE Dr. Essam H. Jiffri.>")