Download presentation
Presentation is loading. Please wait.

2
1- Direct toxicity : This usually takes time before it manifests clinically. The toxic effect is usually dose related, Other factors such as age and renal function can enhance toxicity.

3
2- Hypersensitivity reaction: This is not dose related and requires prior sensitization to the drug. It is a result of interactions between the drug and humeral antibodies or sensitized lymphocytes.

4
3- Pulmonary oedema: This can occur with various drugs. Pulmonary oedema typically occurs within hours of administration of the drug. 4- Pulmonary haemorrhage: This is most commonly a complication of anticoagulant therapy or drug- induced thrombocytopenia.

5
Amiodarone is one of the most frequently prescribed anti-arrhythmic agents worldwide. Although it is extensively used in the treatment of life-threatening arrhythmias, it can act as a double- edged sword considering its potentially serious side effects.

6
Amiodarone is considered a "broad spectrum" antiarrhythmic medication, Class III anti arrhythmic agent. It has a wide spectrum of electrophysiologic effects. It displays use-dependent sodium channel blockade, noncompetitive alpha and beta adrenoreceptor blockade and calcium channel blockade. Amiodarone is also a vasodilator and was initially developed as an anti-anginal agent.

7
Amiodarone toxicity is influenced by the dosage employed and the duration of its use. Its most feared toxicity is pulmonary fibrosis which can be fatal in 10% of individuals treated for recurrent ventricular arrhythmias.

8
The mechanisms involved in amiodarone-induced pulmonary injury are incompletely understood. Several mechanisms have been proposed by which amiodarone results in pulmonary toxicity.

9
Suspected mechanisms of amiodorone toxicity: a- Immunologic disorders (indirect toxicity) b- Direct toxicity to lung cells
 b- Direct toxicity to lung cells")
10
a- Immunologic disorders: - the damage is modulated by cellular immune mechanisms. - Amiodarone-induced lung disease is similar to hypersensitivity pneumonitis. -Systemic amiodarone treatment causes interstitial pulmonary inflammation with increased total number of lymphocytes and polymorphonuclear leukocytes in the lung.

11
b- Direct toxicity to lung cells Impairs lipid metabolism Damage to the pulmonary endothelium increases cellular phospho-lipid content Produce toxic oxidants when exposed to high oxygen concentrations

12
Within weeks of commencement of the therapy the patient typically complains of: The progressive development of nonproductive cough Dyspnea Weight loss Occasionally, low-grade fever.

13
A miodarone pulmonary toxicity clinical presentations I. Chronical interstitial pneumonitis (is the most common ) -Begins with nonproductive cough, dyspnea, and weight loss; these generally occur after two or more months of therapy.
 -Begins with nonproductive cough, dyspnea, and weight loss; these generally occur after two or more months of therapy..")
14
II. Organizational pneumonia: It presents with more acute findings initially: non-productive cough, crackles and signs of pleurisy ( sharp chest pain when breathing deeply ). There are irregular interstitial, alveolar or mixed infiltrates on chest X-ray. The clinical presentation mimics infectious pneumonitis.
. There are irregular interstitial, alveolar or mixed infiltrates on chest X-ray. The clinical presentation mimics infectious pneumonitis..")
15
III. Acute respiratory distress syndrome (ARDS): It occurs rarely, in patients undergoing surgery or pulmonary angiography and receiving amiodarone. It is characterized by diffuse alveolar damage, showing signs of acute interstitial pneumonitis with hyaline membranes IV. A solitary or multiple pulmonary masses: Typically located in upper lobes and may suggest lung neoplasm.
: It occurs rarely, in patients undergoing surgery or pulmonary angiography and receiving amiodarone. It is characterized by diffuse alveolar damage, showing signs of acute interstitial pneumonitis with hyaline membranes IV. A solitary or multiple pulmonary masses: Typically located in upper lobes and may suggest lung neoplasm..")
16
The clinical presentation can be similar to pneumonia, congestive heart failure or pulmonary embolism. a) A positive gallium scan: Can help differentiate AT from pulmonary embolism and congestive heart failure but can’t be relied upon exclusively to make the diagnosis.
 A positive gallium scan: Can help differentiate AT from pulmonary embolism and congestive heart failure but can’t be relied upon exclusively to make the diagnosis..")
17
b) Computed tomography (CT): Amiodarone contains about 37% iodine by weight, (without contrast) may be helpful in diagnosis. Infiltrates caused by amiodarone c) A bronchoscopy: - May be helpful in excluding infection. - Accumulation of foamy acrophages in the alveolar spaces, type II cell hyperplasia, and fibrosis are seen in amiodarone toxicity.
 A bronchoscopy: - May be helpful in excluding infection. - Accumulation of foamy acrophages in the alveolar spaces, type II cell hyperplasia, and fibrosis are seen in amiodarone toxicity..")
18
High cumulative dose (a daily dose greater than 400 mg/day) Duration of therapy (exceeding 2 months) Elderly patients preexisting lung disease or an abnormal chest x-ray before treatment with amiodarone, patients who undergo surgery and/or pulmonary angiography while on amiodarone therapy have an increased risk for developing amiodarone-induced pulmonary toxicity.
 Duration of therapy (exceeding 2 months) Elderly patients preexisting lung disease or an abnormal chest x-ray before treatment with amiodarone, patients who undergo surgery and/or pulmonary angiography while on amiodarone therapy have an increased risk for developing amiodarone-induced pulmonary toxicity.")
19
After stopping, amiodarone resolution is likely to be slow, this has been attributed to the long elimination half- life of the drug and the tendency to concentrate in tissues such as the lung. Corticosteroid drugs (Prednisone) should be given to speed up the recovery process and perhaps to minimize the likelihood of lung fibrosisat.
 should be given to speed up the recovery process and perhaps to minimize the likelihood of lung fibrosisat..")
20
Risk factors: 1- Age: 59-year old male 2- Smoker 3- Taking amiodarone for 5 years. Main complain: 1- Progressive dyspnea, 2- Cough 3- 5 kg weight loss. 4-Chest x-ray at admission showed enlarged heart shadow and enlarged lymph nodes.

21
Treatment: Amiodarone was eliminated from his medication profile. (patient’s clinical condition promptly improved, and chest x-ray performed after 7 days showed corresponding improvement) Treated with methylprednisolone (40mg IV daily during the first two weeks), and subsequently with prednisone (20 mg/day orally for two months).
 Treated with methylprednisolone (40mg IV daily during the first two weeks), and subsequently with prednisone (20 mg/day orally for two months)..")
22
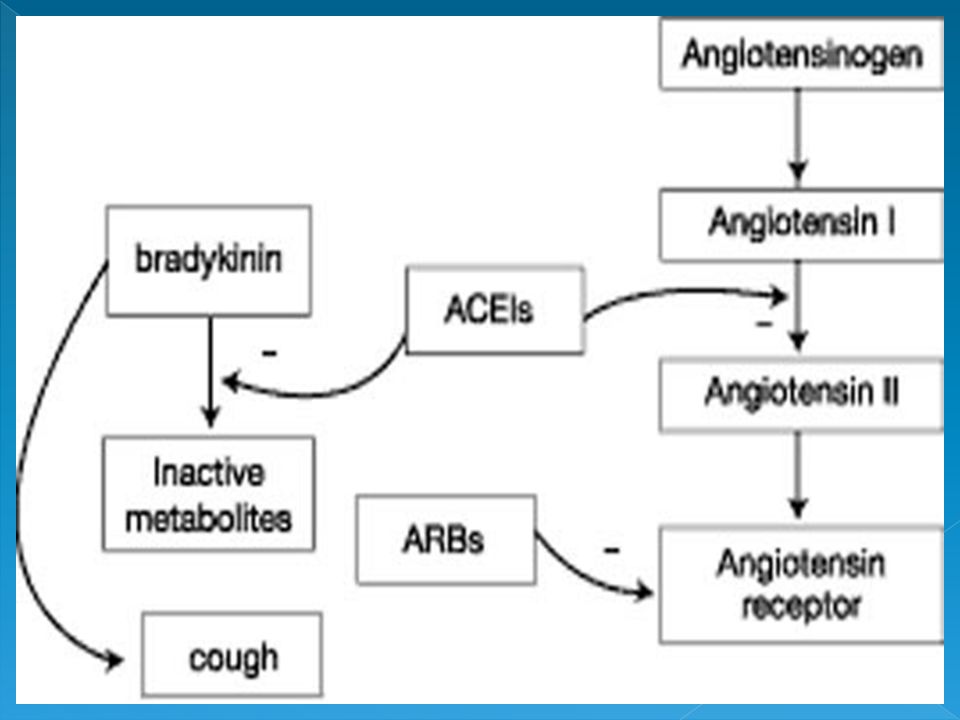
ACEI are associated with many respiratory side-effects. the most frequently reported being dry cough with or without bronchial hyper-reactivity. life-threatening angioedema was also reported.

23
ACE-associated cough: Is characterized by being: dry, persistent, nocturnal, resides only by stopping the drug (after 3-10 days). Kinins and substance P are suspected to play a role.

24
The inhibition of ACE (also known as kininase II and bradykinin dehydrogenase) prevents the conversion of angiotension I to angiotensin II. ACE inhibitor cough is thought to be linked to the suppression of ACE, which is proposed to result in an accumulation of substances normally metabolized by ACE: speciallly bradykinin.

25
The development of cough and angioedema may result from a more complex cascade of events. Bradykinin has been shown to induce the production of arachidonic acid metabolites and nitric oxide (NO), and promote cough through proinflammatory mechanisms.
, and promote cough through proinflammatory mechanisms..")
28
1- In cases in which the continuation of an ACEI is necessary despite cough, cromolyn (mast cell stabilizers, anti-inflammatory), theophylline (bronchodilator), and local anesthetics have been reported to be of benefit 2- Cyclooxygenase inhibitors (COX) has been reported to be of benefit, intermediate doses of aspirin (500 mg/day) but not low doses (100 mg/day) can suppress ACE inhibitor cough.
, theophylline (bronchodilator), and local anesthetics have been reported to be of benefit 2- Cyclooxygenase inhibitors (COX) has been reported to be of benefit, intermediate doses of aspirin (500 mg/day) but not low doses (100 mg/day) can suppress ACE inhibitor cough.")
29
3- The hypothesis that because NO has proinflammatory effects on bronchial epithelial cells, supplemental iron, an inhibitor of NO synthase, may reduce the cough associated with the use of ACE inhibitors.

30
4- If the patient has a good antihypertensive response to the ACE inhibitor, an angiotensin II receptor antagonist, such as losartan, which blocks only angiotensin II receptors and has no effect on kinins or other mediators, can be considered.

31
A 60 year old man was admitted to hospital with dyspnoea, fever and sweats. He was a smoker and had been treated with captopril 50 mg for high blood pressure for about 3 years. He had never had any respiratory symptoms but he said that episodes of dry cough sometimes attached him.

Similar presentations



>")








 Dr. Meg-angela Christi Amores.>")




 disorder. A complication of lung disorders where the.>")
 Harm associated with the use of a given medications OR Unwanted or harmful reaction experienced after the.>")

