Download presentation
Presentation is loading. Please wait.

1
Metabolism - Session 5, Lecture 2 Nitrogen metabolism Marks’ Basic Medical Biochemistry 2 nd edition. Section 7, chapters 37, 38 (39 &42) DR. Hasanat A. Aljabery
 DR. Hasanat A. Aljabery.")
2
Nitrogen metabolism Synthesis, utilisation, breakdown & excretion of N-compounds in the body (no storage). Major compounds: proteins & amino acids. DNA, RNA, (purines & pyrimidines). smaller amounts of others – porphyrins (haem), creatine, neurotransmitters. Clinically important because of changes in various disease states. - several N-compounds measured in blood/urine as an aid to diagnosis (urea, bilirubin, creatinine).
. smaller amounts of others – porphyrins (haem), creatine, neurotransmitters. Clinically important because of changes in various disease states. - several N-compounds measured in blood/urine as an aid to diagnosis (urea, bilirubin, creatinine)..")
3
Most nitrogen enters the body as amino acids derived from protein in the diet. Most nitrogen excreted from the body as urea in the urine. Smaller amounts of creatinine, uric acid & ammonia, protein (skin, hair, nails). Nitrogen balance
. Nitrogen balance.")
4
Overview of whole body N-metabolism (70kg male in nitrogen balance ) Dietary protein (16g N) Amino acid pool (16g N) N-compounds (60g N) Body proteins (2kg N) Loss of skin & hair (2g N) N-waste products in urine (14g N)
 Dietary protein (16g N) Amino acid pool (16g N) N-compounds (60g N) Body proteins (2kg N) Loss of skin & hair (2g N) N-waste products in urine (14g N)")
5
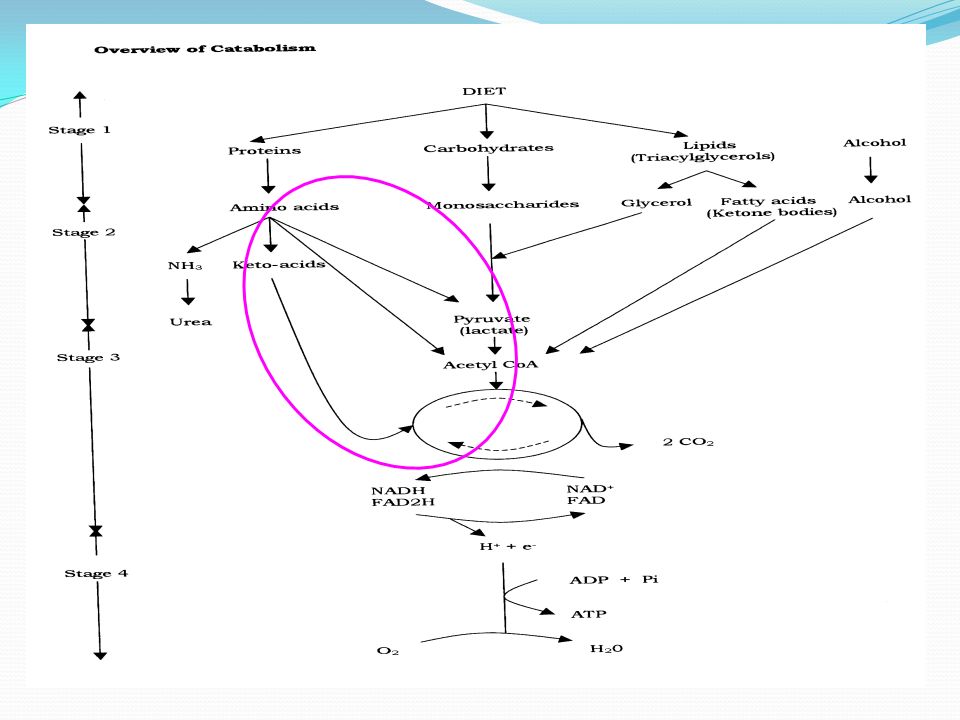
Amino acid functions Protein synthesis - requires all 20 amino acids Synthesis of other N-compounds - requires specific amino acids. Any excess is broken down to intermediates of carbohydrate and/or lipid metabolism.

7
Protein and Amino Acid Metabolism protein extracellular proteases in GI tract amino acids N Synthesis of proteins andureapyruvate N-cont’g cmpdsoxaloacetate (eg purines, creatine, haem) fumarate 2-ketoglutarate succinate acetyl~CoA I II
 fumarate 2-ketoglutarate succinate acetyl~CoA I II")
8
Amino acid breakdown Liver most important tissue. Each amino acid has its own pathway of breakdown related to nature of side chain (R-group): R-CH(NH 2 )-COOH * Pathways share common features: early step is removal of amino group (transamination/deamination) N-atoms converted to urea for excretion. C-atoms converted to intermediates of carbohydrate and/or lipid metabolism (glucogenic/ketogenic).
: R-CH(NH 2 )-COOH * Pathways share common features: early step is removal of amino group (transamination/deamination) N-atoms converted to urea for excretion. C-atoms converted to intermediates of carbohydrate and/or lipid metabolism (glucogenic/ketogenic)..")
9
R 1 R 2 R 1 R 2 H-C-NH 2 + C=O C=O + H-C-NH 2 COOH COOH COOH COOH amino acid 1 keto acid 2 keto acid 1 amino acid 2 -ketoglutarate glutamate (oxaloacetate) (aspartate) Amino group transferred to a keto-acid. Keto-acid usually -ketoglutarate (or oxaloacetate). Removal of the amino group - Transamination
. Removal of the amino group - Transamination.")
10
Most amino acids are transaminated. Reaction reversible – direction depends on [amino acid]. Transaminases (aminotransferases) are highly active in liver. released into the blood when liver damaged their measurement in blood used clinically to assess liver function. Removal of the amino group - Transamination
![Most amino acids are transaminated. Reaction reversible – direction depends on [amino acid].](http://images.slideplayer.com/35/10527222/slides/slide_10.jpg "Transaminases (aminotransferases) are highly active in liver. released into the blood when liver damaged their measurement in blood used clinically to assess liver function. Removal of the amino group - Transamination.")
11
Amino group released as NH 3. R-CH(NH 2 )-COOH R-CO-COOH + NH 3 N.B. NH 3 reacts with water: NH 3 + H 2 O NH 4 + + OH - Removal of the amino group - Deamination

12
Several enzymes of varying specificity: L & D amino acid oxidases: amino acid keto acid + NH 3 Glutaminase: glutamine glutamate + NH 3 NH 2 CO-(CH 2 ) 2 -CH(NH 2 )-COOH Glutamate dehydrogenase: glutamate + NAD + -ketoglutarate + NADH + NH 3 Removal of the amino group - Deamination
 2 -CH(NH 2 )-COOH Glutamate dehydrogenase: glutamate + NAD + -ketoglutarate + NADH + NH 3 Removal of the amino group - Deamination")
13
Glutamine, glutamate & - ketoglutarate (at pH 7) glutamineNH 2 CO-(CH 2 ) 2 -CH(NH 3 + )-COO - glutamate - OOC-(CH 2 ) 2 -CH(NH 3 + )-COO - -ketoglutarate - OOC-(CH 2 ) 2 -CO-COO - transaminases glutamate dehydrogenase glutaminase glutamine synthase -NH 3 + NH 3
 glutamineNH 2 CO-(CH 2 ) 2 -CH(NH 3 + )-COO - glutamate - OOC-(CH 2 ) 2 -CH(NH 3 + )-COO - -ketoglutarate - OOC-(CH 2 ) 2 -CO-COO - transaminases glutamate dehydrogenase glutaminase glutamine synthase -NH 3 + NH 3")
14
Ammonia metabolism Blood concentration normally low (25-40 M) – present as NH 4 +. Produced: during amino acid degradation. by gut bacteria (absorbed from gut) Toxic to cells
 Toxic to cells.")
15
Ammonia toxicity CNS very sensitive – blurred vision, tremors, slurred speech, coma. Toxicity of ammonia: reduces TCA cycle activity (reacts with -ketoglutarate to form glutamate) energy supply to cells disrupted - cell function impaired. pH effects. affects neurotransmitter synthesis.
 energy supply to cells disrupted - cell function impaired. pH effects. affects neurotransmitter synthesis..")
16
Ammonia detoxification Three major ways: 1) used to synthesise glutamine. 2) converted to urea. 3) some excreted directly in the urine.
 converted to urea. 3) some excreted directly in the urine..")
17
1) Synthesis of Glutamine Formed from glutamate + ammonia in cells (requires ATP). Highest concentration of any amino acid in blood (0.5mM). Can be used to synthesise N-compounds (purines & pyrimidines). Excess released from cells, transported in blood to liver & kidney where it is broken down to release ammonia (glutaminase): kidney – ammonia excreted directly in urine. liver – ammonia used to make urea.
. Can be used to synthesise N-compounds (purines & pyrimidines). Excess released from cells, transported in blood to liver & kidney where it is broken down to release ammonia (glutaminase): kidney – ammonia excreted directly in urine. liver – ammonia used to make urea..")
18
2) Synthesis of Urea High N-content CO(NH 2 ) 2. Non-toxic. Extremely water soluble. Synthesised in liver. Chemically inert – man has no enzymes to break it down. (bacteria can break it down to release NH 3 ) Most excreted in urine via the kidneys.
 Most excreted in urine via the kidneys..")
19
Cycle of 5 enzyme catalysed reactions (Urea cycle) Enzymes only expressed in liver. Pathway requires ATP. NH 4 + + HCO 3 - + aspartate + 3ATP CO(NH 2 ) 2 + fumarate + 2ADP + AMP + 4Pi Enzymes not subjected to feedback inhibition. Amount of enzymes in liver normally related to need to dispose of ammonia. (NB Group work for session 1- protein supplement hastened death of Sudanese children) 2) Synthesis of Urea
 2 + fumarate + 2ADP + AMP + 4Pi Enzymes not subjected to feedback inhibition. Amount of enzymes in liver normally related to need to dispose of ammonia. (NB Group work for session 1- protein supplement hastened death of Sudanese children) 2) Synthesis of Urea.")
20
Defects in urea cycle Inherited defects in urea cycle occur ~1 in 30,000 live births. Complete loss of an enzyme is fatal. Partial loss: hyperammonaemia. accumulation/excretion of urea cycle intermediates.

21
Defects in urea cycle Clinical picture: Vomiting, lethargy, irritability, mental retardation, seizures, coma. Severity depends on: extent of defect amount of protein eaten. Treatment: low protein diets. replace amino acids in diet with keto acids.

22
Clinical problems of amino acid metabolism Many inherited disorders – all result from enzyme defects. Only a clinical problem when affected enzyme is involved in amino acid breakdown. Problem: Amino acid and/or intermediate in its metabolism accumulate & may be toxic. Treatment: restrict amount of amino acid in diet. must be done early in life before damage is irreversible.

23
Phenylketonuria (PKU) -CH 2 -CO-COOH Urine contains large amount of phenylketones (phenylpyruvate) PKU caused by defect in 1 st step in phenylalanine breakdown: phenylalanine tyrosine (phenylalanine hydroxylase) As a consequence of the defect, phenylalanine: accumulates in blood & tissues. enters abnormal pathways of metabolism – phenylpyruvate.

24
Defect in phenylalanine hydroxylase -CH 2 CH(NH 2 )COOH HO- -CH 2 CH(NH 2 )COOH phenylalanine tyrosine Phenylketonuria (PKU) Complex reaction requiring O2 and H-carrier (tetrahydrobiopterin). ~ 98% of defects affect enzyme directly. ~ 2% of defects affect coenzyme system.

25
Phenylpyruvate is formed from phenylalanine by transamination: -CH 2 -CH(NH 2 )-COOH -CH 2- CO-COOH Formed from phenylalanine by transamination: Toxic, especially to the CNS: inhibits pyruvate uptake into mitochondria. reduces ATP synthesis from glucose. development and functioning of CNS impaired. Diagnosis must be made early in life before irreversible damage is done. Phenylketonuria (PKU)
.")
26
Diagnosis of PKU In UK all newborn are screened: phenylketones in urine. phenylalanine in blood (rises from 0.1 mM to > 1.0mM).
..")
27
Treatment of PKU Phenylalanine is an essential amino acid – total removal from diet is not an option. Modify diet to contain: proteins low in phenylalanine special protein hydrolysate - treated to remove phenylalanine.

28
Creatine phosphate

29
The reaction of creatine with ATP catalysed by creatine kinase is reversible in muscle cells (skeletal & cardiac): creatine + ATP creatine phosphate + ADP When the [ATP] is high When the [ATP] is low Thus, creatine phosphate can act as a small store of energy in muscle cells.
![The reaction of creatine with ATP catalysed by creatine kinase is reversible in muscle cells (skeletal & cardiac): creatine + ATP creatine phosphate + ADP When the [ATP] is high When the [ATP] is low Thus, creatine phosphate can act as a small store of energy in muscle cells.](http://images.slideplayer.com/35/10527222/slides/slide_29.jpg "The reaction of creatine with ATP catalysed by creatine kinase is reversible in muscle cells (skeletal & cardiac): creatine + ATP creatine phosphate + ADP When the [ATP] is high When the [ATP] is low Thus, creatine phosphate can act as a small store of energy in muscle cells.")
30
Clinical importance of C~P Amount of C and C~P in body related to muscle mass. C & C~P undergo non-enzymatic cyclization to creatinine. Creatinine has no function and is excreted from body via kidneys in urine. Rate of formation of creatinine related to [C] & [C~P]. Amount of creatinine in blood & urine related to: muscle mass (males> females). muscle turnover ( during muscle wasting). kidney function.
. muscle turnover ( during muscle wasting). kidney function..")
31
Clinical importance of creatine kinase Creatine kinase is composed of 2 subunits. The subunits are of 2 types (B & M) 3 different enzymes exist: BB (CK-1) in brain. BM (CK-2) in heart. MM (CK-3) in skeletal & heart muscle. CK-2 released from damaged cardiac muscle shortly (4-6hr) after a myocardial infarction (heart attack). Presence of CK-2 in blood used in diagnosis of a heart attack.
 3 different enzymes exist: BB (CK-1) in brain. BM (CK-2) in heart. MM (CK-3) in skeletal & heart muscle. CK-2 released from damaged cardiac muscle shortly (4-6hr) after a myocardial infarction (heart attack). Presence of CK-2 in blood used in diagnosis of a heart attack..")
Similar presentations





>")

In stomach: passage of food into stomach stimulates gastric mucosa to secret a polypeptide hormone called: Gastrin.>")











