Download presentation
Presentation is loading. Please wait.

1
Approach to lymphadenopathy
Dr. Mohamed Haseen Basha Assistant professor ( Pediatrics) Faculty of Medicine Al Maarefa College of Science and Technology
 Faculty of Medicine. Al Maarefa College of Science and Technology.")
2
Definition Lymphadenopathy is enlargement of the lymph nodes beyond this normal state. Practically this is any node >1.0 cm in greatest diameter. Lymphadenopathy refers to nodes that are abnormal in either size, consistency or number. Certain nodes should be considered enlarged at different sizes (i.e. Epitrochlear nodes > 0.5 cm, inguinal nodes > 1.5 cm, submandibular nodes > 1.5 cm)
")
3
Generalized - if lymph nodes are enlarged in two or more non-contiguous areas. It almost always indicates the presence of a significant systemic disease. Localized - if only one area is involved. Palpable lymph nodes are normal in anterior cervical, axillary and inguinal regions in healthy children.

5
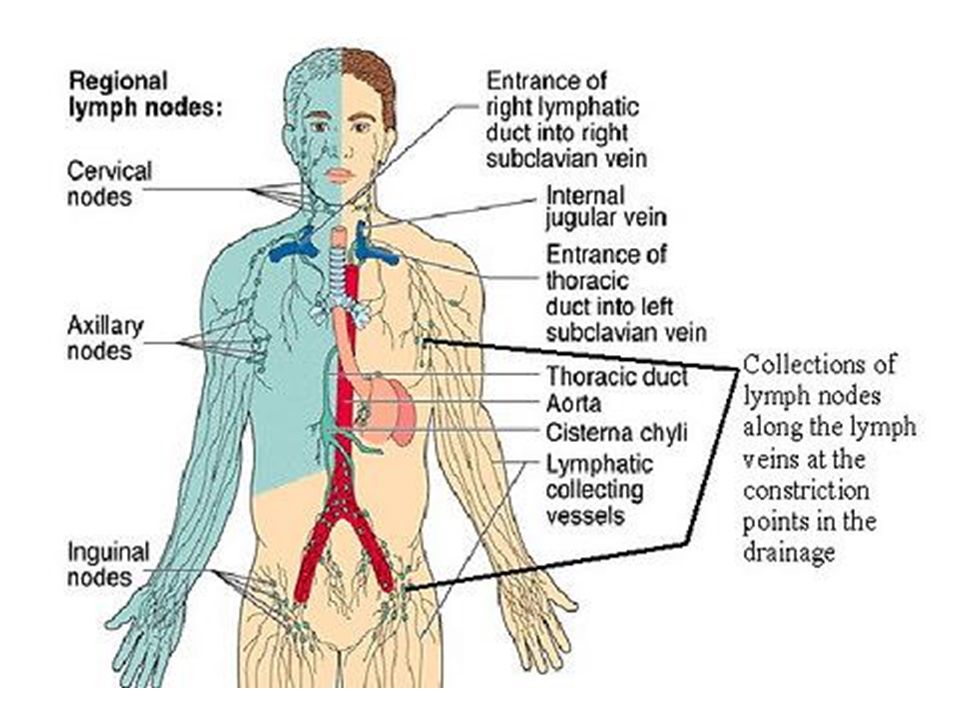
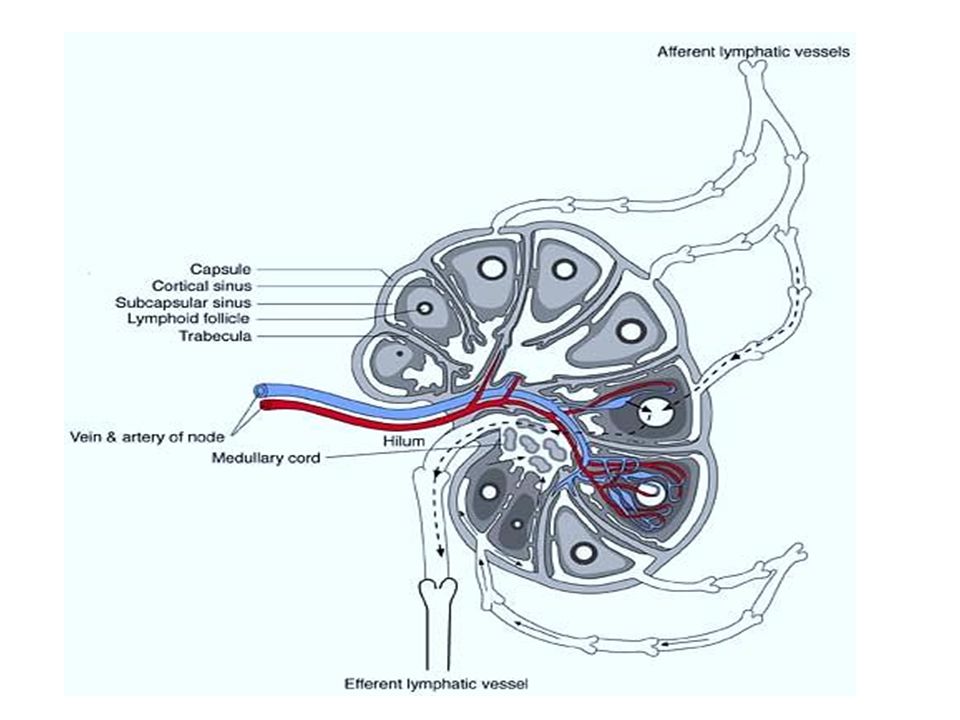
Lymph Node Anatomy Collection of lymphoid cells attached to both vascular and lymphatic systems Over 600 lymph nodes in the body Function To provide optimal sites for the concentration of free or cell-associated antigens and recirculating lymphocytes – “sensitization of the immune response” To allow contact between B-cells, T-cells and macrophages Lymphadenopathy - node greater than 1cm in size

8
Why do lymph nodes enlarge?
Increase in the number of benign lymphocytes and macrophages in response to antigens Infiltration of inflammatory cells in infection (lymphadenitis) In situ proliferation of malignant lymphocytes or macrophages Infiltration by metastatic malignant cells Infiltration of lymph nodes by metabolite laden macrophages (lipid storage diseases)
 In situ proliferation of malignant lymphocytes or macrophages. Infiltration by metastatic malignant cells. Infiltration of lymph nodes by metabolite laden macrophages (lipid storage diseases)")
9
Localized lymphadenopathy
1. Local infection in draining area 2. Metastasis from cancers 3. Lymphoma—Hodgkin’s disease 4. Scrofuloderma

10
Generalised lymphadenopathy
Infections Viral illnesses Ebstein Barr virus infection Cytomegalovirus infection Infectious mononucleosis HIV Bacterial Tuberculosis Brucellosis Chancroid (usually localized) Parasitic Toxoplasmosis Leishmaniasis Trypanosomiasis Fungal Histoplasmosis Coccidioidomycosis Chlamydia Lymphogranuloma venereum (usually localised)
 Parasitic. Toxoplasmosis. Leishmaniasis. Trypanosomiasis. Fungal. Histoplasmosis. Coccidioidomycosis. Chlamydia. Lymphogranuloma venereum (usually localised)")
11
Generalised lymphadenopathy
Malignant Hematological Hodgkin’s disease Non-Hodgkin’s lymphoma Acute and chronic leukaemias Metastatic Connective tissue disorder Systemic lupus erythematosus Rheumatoid arthritis MCTD Infiltrative Sarcoidosis Histiocytosis X Others (rare) Drugs, e.g. Phenytoin Mucocutaneous LN disease (Kawasaki’s disease)
 Drugs, e.g. Phenytoin. Mucocutaneous LN disease (Kawasaki’s disease)")
12
Drugs causing lymphadenopathy
Allopurinol Atenolol Captopril Carbamazepine Gold Hydralazine Phenytoin Primidone Pyrimethamine Quinidine Trimethoprim / Sulfamethozole Penicillins

13
Approach to Lymphadenopathy
Normally, lymphoid tissue enlarges until puberty and then undergoes gradual atrophy throughout the rest of life. Normal lymph nodes are most prominent in children ages 4 to 8 years old.

14
History History of fever:
History of fever is dominant in infectious mononucleosis, tuberculosis, HIV, Leishmaniasis, Disseminated fungal & parasitic infections and lymphoreticular malignancies. Ask about: Type and pattern of fever Duration of fever History of constitutional symptoms: Constitutional symptoms, i.e.anorexia, malaise, weight loss, night sweats. These symptoms are prominent in tuberculosis and also may be seen as “B-symptoms” in patients with lymphomas.

15
History of easy bruising, petechial hemorrhages, gum bleeds, epistaxis, suggesting thrombocytopenia—may be seen in acute leukaemias. History of onset generalized weakness, paleness of skin, shortness of breath may suggest anemia, which is an important feature of acute leukaemias and other hematological malignancies. History of any discharge from the nodes. Formation of a sinus and discharge from the nodes is very typical of tubercular lymphadenitis. Sexual behaviour—ask for a history of high risk behaviour. History of joint pains, swelling, myalgias, skin rash may suggest rheumatological or connective tissue disease. Past history—Ask for a past history of Tuberculosis or Receiving anti-tuberculosis drugs, Phenytoin intake

16
General Physical Examination
Vital signs Fever—always measure body temperature to assess for fever. Record the temperature pattern. Pallor—pallor of mucous membranes, lower palpebral conjunctiva, and of the skin is seen in anemia. Severe anemia may suggest a hematological malignancy such as acute leukemia or other disorders such as kala-azar Petechiae Ecchymosis Gum bleeds Epistaxis

17
Examination of Lymph Nodes
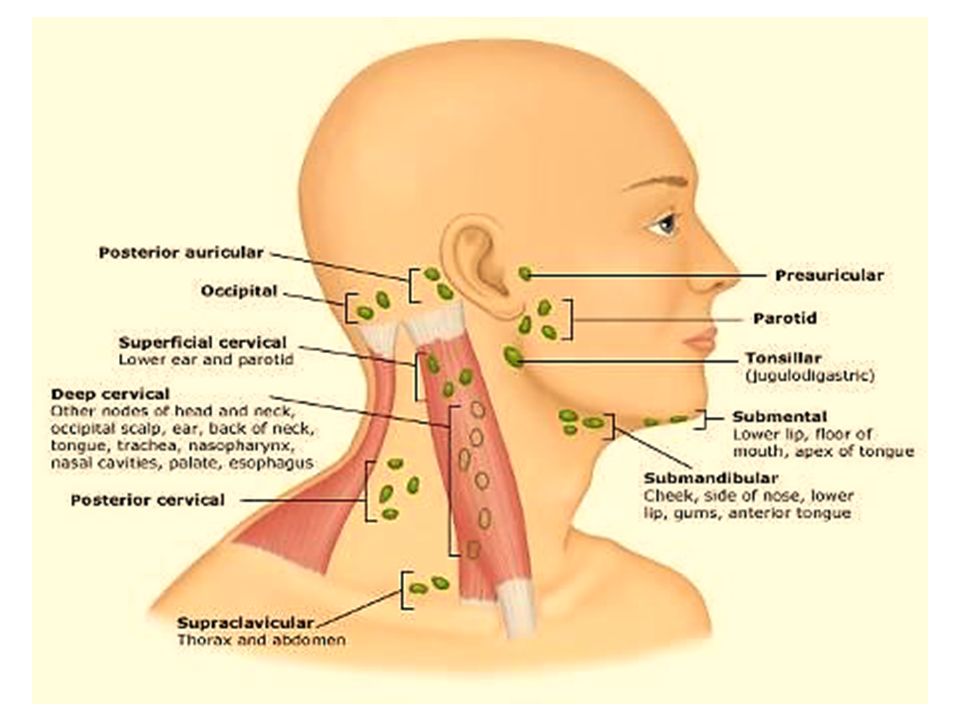
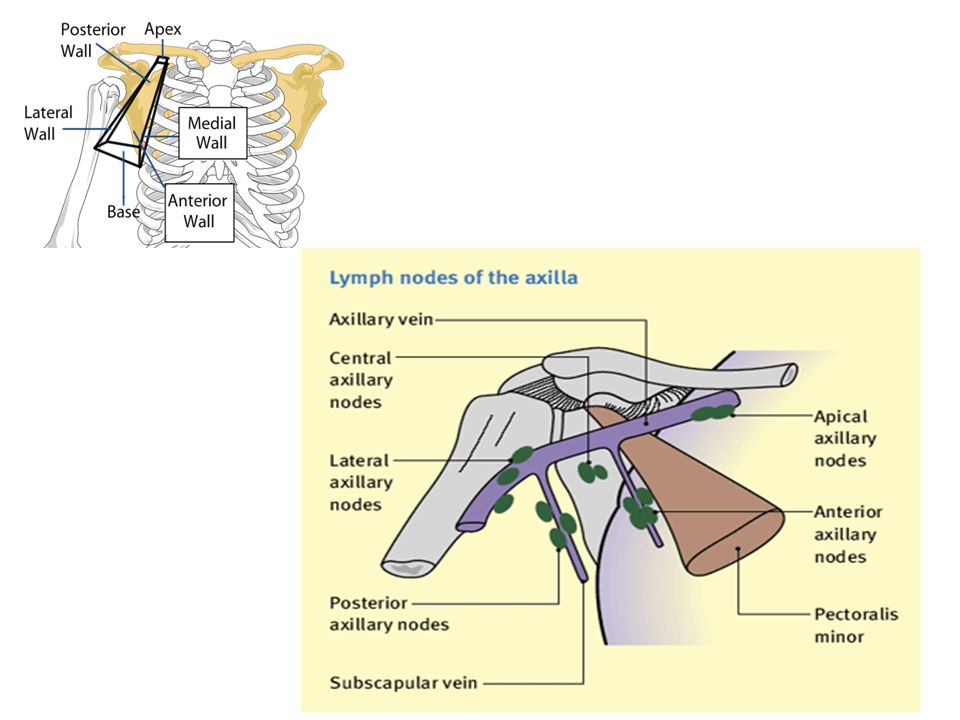
Head and Neck Preauricular Post auricular Occipital Tonsillar Submandibular Submental Superficial anterior cervical Deep cervical Posterior cervical Supra clavicular Infra clavicular The Arms Axillary Anterior axillary (pectoral) Lateral (brachial) Mid axillary (central) Posterior (subscapular) Epitrochlear The Legs Superficial superior inguinal Superficial inferior inguinal Popliteal (occasionally) It is also important to examine the oropharynx for the Waldeyer’s ring of lymph nodes and the abdomen for any abdominal lymph nodes that may be enlarged and palpable.
 Lateral (brachial) Mid axillary (central) Posterior (subscapular) Epitrochlear. The Legs. Superficial superior inguinal. Superficial inferior inguinal. Popliteal (occasionally) It is also important to examine the oropharynx for the Waldeyer’s ring of lymph nodes and the abdomen for any abdominal lymph nodes that may be enlarged and palpable.")
22
1. Site of Lymph Nodes Whether Generalised or localised
Which group(s) of lymph nodes Generalised lymphadenopathy is most commonly due to tuberculosis, lymphoma, HIV infection. Certain diseases may produce enlargement of specific lymph node groups. Ex: left supraclavicular lymph node— called “Virchow‘s node”—is suggestive of metastasis from a gastrointestinal tract primary malignancy. Waldeyer’s ring—enlargement of nodes in the posterior oropharynx and nasopharynx is seen especially in non-Hodgkin’s lymphoma. Cervical adenopathy—commonly seen in upper respiratory infections, infectious mononucleosis, tuberculosis.
 of lymph nodes. Generalised lymphadenopathy is most commonly due to tuberculosis, lymphoma, HIV infection. Certain diseases may produce enlargement of specific lymph node groups. Ex: left supraclavicular lymph node— called Virchow‘s node —is suggestive of metastasis from a gastrointestinal tract primary malignancy. Waldeyer’s ring—enlargement of nodes in the posterior oropharynx and nasopharynx is seen especially in non-Hodgkin’s lymphoma. Cervical adenopathy—commonly seen in upper respiratory infections, infectious mononucleosis, tuberculosis.")
23
Occipital lymphadenopathy —usually due to scalp infection
Cervical lymphadenopathy —diseases of oral cavity, metastases from head and neck, breast, thyroid and lung malignancies. Axillary adenopathy is mainly due to an infection of the upper limb. It may also be seen in metastasis from carcinoma of the breast and hence, examination of breasts is very important in any patient with isolated axillary node enlargement. Inguinal lymphadenopathy is quite common especially in those walking barefoot. However, sexually transmitted diseases must always be ruled out.

24
2. Size of Lymph Node Measure the size of the enlarged lymph nodes, in all enlarged groups and comment on them individually. If multiple nodes are enlarged always give the range from the size of the smallest node to the largest palpable node. Size is important as: Small nodes < 1 cm size are usually benign or due to reactive causes. Hence, isolated, small nodes, need not be aggressively subjected to a FNAC and/or biopsy and can be closely followed up. Nodes > 2 cm in size are unlikely to be ‘reactive’ and should be investigated.

25
3. Consistency and Texture
Describe the consistency of the lymph nodes as soft, firm, hard, rubbery. In many instances the consistency provides important clues to the etiology. Soft nodes - usually benign Hard nodes - infiltration by cancers. Rubbery nodes - lymphomas. 4. Tethering to Each Other Comment whether the lymph nodes are individually palpable or are all tethered to each other as a mass. Matted, conglomerate lymph nodes are seen in tuberculosis. Lymph nodes, though multiple in number, all still individually palpable in lymphomas.

26
6. Sinus Formation/Discharge
5. Fixity Assess whether the lymph nodes are fixed to the Overlying skin or Underlying structures Fixed, immobile lymph nodes - Malignant infiltration Lymph nodes in lymphoma - Freely mobile, unattached to overlying skin or underlying structures Tubercular lymph nodes may be tethered to overlying skin. 6. Sinus Formation/Discharge The presence of a draining or discharging sinus over a lymph node suggests Tuberculosis Actinomycosis

27
In addition to the general physical examination, perform a detailed systemic examination and examination of all suspected drainage areas. Respiratory Examination: Evaluate for evidence of: Tuberculosis Pleural effusion Mass lesion Abdomen: palpate for Hepatomegaly Splenomegaly Intra-abdominal lymph nodes Ascites Evaluate genitalia for possible primary tumours. Head and neck examination, especially in patients with cervical adenopathy.

28
Generalised lymphadenopathy with hepatosplenomegaly, the differential diagnosis would include:
a. Disseminated tuberculosis b. Lymphoma c. Disseminated histoplasmosis d. Kala-azar Enlarged nodes are matted and conglomerate - Disseminated tuberculosis Firm, rubbery, not matted/ fixed lymph nodes - Lymphoma

29
If splenomegaly is prominent and massive, with a history o prolonged fever and travel to an endemic area- kala-azar In a patient with severe anaemia, gum bleeds, ecchymosis, hepatosplenomegaly and lymphadenopathy - Acute leukaemia In a patient with hard, cervical lymphadenopathy with evidence of Horner’s syndrome and/or superior vena cava obstruction- Carcinoma Bronchus

30
Differentiation between benign and malignant lymphadenopathy
Feature Malignant Benign Size > 2 cm < 2 cm (< 1 cm ) Consistency Hard, firm or rubbery Soft Duration > 2 weeks < 2 weeks Mobility Fixed Mobile Surroundings Attached(Invasion) Not attached Location Supraclavicular, Epitrochlear or Generalized Inguinal, Submandibular Tenderness Usually non-tender Usually tender
 Consistency. Hard, firm or rubbery. Soft. Duration. > 2 weeks. < 2 weeks. Mobility. Fixed. Mobile. Surroundings. Attached(Invasion) Not attached. Location. Supraclavicular, Epitrochlear or Generalized. Inguinal, Submandibular. Tenderness. Usually non-tender. Usually tender.")
31
Mimicking Lymphadenopathy
Branchial cleft cyst Cystic hygroma Thyroglossal duct cyst Epidermoid cyst Sternocleidomastoid tumor

32
Management Identify underlying cause and treat as appropriate – confirmatory tests Bacterial infection results in large nodes that are warm, erythematous, and tender. Start on antibiotics that cover the bacterial pathogens frequently implicated in lymphadenitis, including staphylococcus aureus and streptococcus pyogenes. Reevaluate in 2-4 weeks. Biopsy if unchanged or larger. Generalized adenopathy – usually has identifiable cause Localized adenopathy 3-4 week observation period for resolution if not high clinical suspicion for malignancy Biopsy if risk for malignancy – excisional

33
When to Investigate ? Patients generally should be considered for investigation and/or referral if: Unexplained generalized lymphadenopathy Any palpable supraclavicular or popliteal node Significant constitutional symptoms Hepatic or splenic enlargement Anemia or bleeding Unresponsiveness to antibiotic treatment Not decreasing in size after appropriate period of observation

34
Investigations: Complete hemogram with peripheral blood smear examination ESR or C-reactive protein Lactate dehydrogenase Uric acid Liver function tests Purified Protein Derivative skin test (PPD) Viral titers Other titers - Toxoplasmosis, Bartonella henselae Chest X-ray (PA) view will help define - Pretracheal, mediastinal lymph node enlargement - Lung parenchymal lesion, e.g. tuberculosis - Lung malignancy—primary and metastasis
 Viral titers. Other titers - Toxoplasmosis, Bartonella henselae. Chest X-ray (PA) view will help define. - Pretracheal, mediastinal lymph node enlargement. - Lung parenchymal lesion, e.g. tuberculosis. - Lung malignancy—primary and metastasis.")
35
Ultrasonography and contrast enhanced CT of the abdomen to delineate
- Hepatomegaly - Splenomegaly - Any hepatic/splenic deposits - Intra-abdominal lymph nodes—identification of any specific character, e.g. central hypodensity/necrosis Patients with cervical adenopathy - to rule out head and neck cancers- CECT (head and neck) Bone marrow aspiration and/or biopsy - Haematological malignancy ELISA for HIV
 Bone marrow aspiration and/or biopsy - Haematological malignancy. ELISA for HIV.")
36
Fine needle aspiration cytology (FNAC) and/or lymph node biopsy
Fine needle aspiration cytology (FNAC) and/or lymph node biopsy. This is the most important diagnostic tool in patients with lymphadenopathy. In most patients with lymphadenopathy, an initial FNAC will provide the diagnosis, e.g. Demonstration of caseous necrosis and granulomas in TB lymphadenitis. Ziehl Neelsen staining may reveal acid-fast bacilli. Metastatic cancers However, a lymph node biopsy should also be performed in all patients with suspected lymphomas.
 and/or lymph node biopsy. This is the most important diagnostic tool in patients with lymphadenopathy. In most patients with lymphadenopathy, an initial FNAC will provide the diagnosis, e.g. Demonstration of caseous necrosis and granulomas in TB lymphadenitis. Ziehl Neelsen staining may reveal acid-fast bacilli. Metastatic cancers. However, a lymph node biopsy should also be performed in all patients with suspected lymphomas.")
37
Indication for biopsy Increase in size over baseline in 2 weeks.
No decease in size in 4-6 weeks. No regression to normal in 8-12 weeks. Development of new signs and symptoms. Persistent unexplained fever, weight loss, night sweats. Hard nodes / fixation of nodes to surrounding tissues.

38
Lymph node biopsy Once biopsy has been chosen , ideally the largest, most suspicious, and most accessible node is selected, taking in to account differing diagnostic yields by site. Inguinal nodes offer the lowest yield and supraclavicular nodes have the highest. Excisional biopsy remains the diagnostic procedure of choice.

39
Role of surgery Acute Suppurative lymphadenitis
Conservative, IV Antibiotics Incision / drainage of Abscess BCG Adenitis. Anti tubercular drugs Fistulated / adherent LN need surgical excision while non adherent lesions heal spontaneously without treatment. Non tuberculous Mycobacterial lymphadenitis Surgical excision is the mainstay of treatment.

40
Approach to Lymphadenopathy
Reassure Family Lymphadenopathy Yes Significant Physical Signs or Symptoms? e.g. Weight loss, Hepatosplenomegaly … Yes No Node(s) : Increase in size Not Resolving Observe : 2-3 Weeks Node(s) Resolving Investigate : (CBC, ESR …) Observe & Follow
 : Increase in size. Not Resolving. Observe : 2-3 Weeks. Node(s) Resolving. Investigate : (CBC, ESR …) Observe. & Follow.")
Similar presentations













 LL (inguinal, femoral and popliteal) Abdomen ( paraaortic,>")









