Download presentation
Presentation is loading. Please wait.

1
Breast Cancer Susan B. Kesmodel, MD, FACS
Assistant Professor of Surgery, Surgical Oncology University of Maryland School of Medicine

2
Objectives Epidemiology Risk factors Screening and Diagnostics
Management Staging Multimodality treatment Outcomes and follow-up Good evening, tonight I’ll be focusing on the the development of SLN bx and the role of SLN bx in patients with melanoma, but I thought I’d start by giving a little background on the epidemiology of the disease, as well as the new AJCC staging system. Then I’ll review the development of SLN bx and finally the role of SLN bx in patients with melanoma.

3
Epidemiology Approximately 190,000 new cases of breast cancer were diagnosed in 2009 Current estimated lifetime risk of developing breast cancer for women in the U.S. is 1 in 8

4
From Jemal A. et al. CA Cancer J Clin 2009;59:225-249.
Breast cancer is the most common cancer in women in the United States, it is the second leading cause of cancer deaths in women behind lung cancer, and the main cause of death in women ages 40 to 59. The incidence of breast cancer in the United States doubled over the last 60 years of the 20th century from about 55 cases per 100,000 women to 118 cases per 100,000 women. The incidence of breast cancer in the United States peaked in 1998 and then there was a slight decline in cases from 2001 to 2003 with is thought to be due mainly to the decreased used of hormone replacement therapy. The increase in breast cancer incidence through the 1990’s was mainly in early stage cancers and was attributed to the increased use of screening in patients. While the incidence of breast cancer increased through the 1990’s, the mortality rate began declining in the early 1990’s. Some of this is due to earlier detection from screening, and some of this is due to adjuvant therapy. From Jemal A. et al. CA Cancer J Clin 2009;59: Copyright ©2009 American Cancer Society

5
Breast Cancer Incidence and Mortality
The incidence of breast cancer in the United States doubled over the last 60 years of the 20th century. There was a sharp increase in incidence in the 1980’s which is most likely due to the increased use of screening mammography. The incidence peaked in 1998 and declined from 2001 to 2004. Mortality from breast cancer began to decline in the early 1990’s due to earlier detection from screening and use of adjuvant therapy. Breast cancer is the most common cancer in women in the United States, it is the second leading cause of cancer deaths in women behind lung cancer, and the main cause of death in women ages 40 to 59. The incidence of breast cancer in the United States doubled over the last 60 years of the 20th century from about 55 cases per 100,000 women to 118 cases per 100,000 women. The incidence of breast cancer in the United States peaked in 1998 and then there was a slight decline in cases from 2001 to 2003 with is thought to be due mainly to the decreased used of hormone replacement therapy. The increase in breast cancer incidence through the 1990’s was mainly in early stage cancers and was attributed to the increased use of screening in patients. While the incidence of breast cancer increased through the 1990’s, the mortality rate began declining in the early 1990’s. Some of this is due to earlier detection from screening, and some of this is due to adjuvant therapy. 5

6
Incidence Rates by Race
Race/Ethnicity Female All Races 122.9 per 100,000 women White 126.5 per 100,000 women Black 118.3 per 100,000 women Asian/Pacific Islander 90.0 per 100,000 women American Indian/Alaska Native 76.4 per 100,000 women Hispanic 86.0 per 100,000 women _breast.pdf

7
Death Rates by Race Race/Ethnicity Female All Races
24.0 per 100,000 women White 23.4 per 100,000 women Black 32.4 per 100,000 women Asian/Pacific Islander 12.2 per 100,000 women American Indian/Alaska Native 17.6 per 100,000 women Hispanic 15.3 per 100,000 women _breast.pdf

8
Age-specific SEER incidence, rates of female breast cancer per 100,000, 2000-2003
_breast.pdf

9
FIGURE 6 Age-standardized Incidence and Mortality Rates for Breast Cancer
There are significant global variations in the incidence of breast cancer and mortality. Breast cancer rates are highest in North America and northern Europe and are lowest in Asia and Africa. Studies of migration patterns to the US have demonstrated the importance of cultural and environmental factors in the development of breast cancer. In general, the incidence of breast cancer increases in second-generation migrants and increases further in 3rd and 4th generation migrants. From Parkin, D. M. et al. CA Cancer J Clin 2005;55: Copyright ©2005 American Cancer Society

10
Risk Factors Age and gender Race and ethnicity Benign breast disease
Personal history of breast cancer Lifestyle and dietary factors Reproductive and hormonal factors Family history and genetic factors Exposure to ionizing radiation Environment factors Numerous risk factors have been identified for breast cancer and the contribution of these risk factors to the development of breast cancer is variable. Let’s look at each one separately. Age and gender are among the strongest risk factors. Women are 100 times more likely than men to develop breast cancer and the incidence of breast cancer increases with age up to the age of 80. Caucasian women are more likely to develop breast cancer than African American women. This is likely due to a combination of environmental and genetic factors. On the other hand, African American women are more likely to die from breast cancer. This again is likely due to a combination of genetic and societal factors that lead to more advanced stage, aggressive cancers. A positive family history of breast cancer confers a modest increased risk of developing breast cancer, 2-3 times that of the general population, however, women with multiple first-degree relatives with breast cancer may have a lifetime risk of as high as 50%, especially in the presence of know, high-risk genetic mutations. Lifetime exposure to estrogen is one of the most important factors for the development of breast cancer, and that is why age at Menarche, age of Menopause, and reproductive factors play a significant role in this disease.

11
Risk Assessment Age Menarche Age at 1st birth
Number of 1st degree relatives with breast cancer Prior breast biopsy How many breast biopsies (positive or negative)? Has the woman had at least one breast biopsy with atypical hyperplasia? Race/ethnicity Several different risk assessment tools have been developed using combinations of major risk factors. The purpose of these models is to help stratify women into risk categories so that optimal screening and prophylactic strategies can be applied. The most widely utilized tool to calculate breast cancer risk is the Breast Cancer Risk Assessment Tool, this is based on a model that was originally developed by Dr. Mitchell Gail and evaluated in caucasian women and has since been expanded to include race. This models are good for risk stratification, but their accuracy for predicting whether a woman will develop cancer is modest.
 Has the woman had at least one breast biopsy with atypical hyperplasia Race/ethnicity. Several different risk assessment tools have been developed using combinations of major risk factors. The purpose of these models is to help stratify women into risk categories so that optimal screening and prophylactic strategies can be applied. The most widely utilized tool to calculate breast cancer risk is the Breast Cancer Risk Assessment Tool, this is based on a model that was originally developed by Dr. Mitchell Gail and evaluated in caucasian women and has since been expanded to include race. This models are good for risk stratification, but their accuracy for predicting whether a woman will develop cancer is modest.")
12
Genetics of Breast Cancer
Only 5-6% of breast cancers are associated with inherited genetic mutations. Two susceptibility genes for breast and ovarian cancer have been identified, BRCA1 and BRCA2. Most breast cancer

13
Reproduced with permission from: Fletcher, S.
Overview of genetics in breast and ovarian cancer. In: UpToDate, Basow, DS (Ed), UpToDate, Waltham, MA, 2010. Copyright (c) 2010 UpToDate, Inc.
, UpToDate, Waltham, MA, Copyright (c) 2010 UpToDate, Inc.")
14
Mammogram Ultrasound MRI
Diagnostic Imaging Mammogram Ultrasound MRI

15
Breast Cancer Screening
Who should be screened? Risk stratification Age to begin Age to stop What method should be used? How often? There is more scientific evidence supporting screening for breast cancer than for any other cancer. The relevant issues are determining who should be screened based on risk assessment, when screening should start and stop, and what method should be used. There is very good evidence that screening mammography should be offered to women between the ages of 50 and 69. However, consensus is not as strong for women ages and women over the age of 70. The proportion of total reduction in overall US breast cancer mortality which is attributable to screening mammograms ranges from 28 to 65 percent (median 46%). Which suggests that screening mammograms have resulted in a 10% decrease in breast cancer mortality. The majority of breast cancers in the United States are diagnosed as a result of an abnormal screening study.
. Which suggests that screening mammograms have resulted in a 10% decrease in breast cancer mortality. The majority of breast cancers in the United States are diagnosed as a result of an abnormal screening study.")
16
Mammogram Screening tool that has picked up many breast cancers early, usually through calcifications or irregular masses Current ACS recommendation is to start screening at the age of 40 for average risk women For higher risk patients may recommend starting screening earlier than the age of 40 (additional screening modalities may also be recommended) Screening mammogram has been shown to significantly decrease breast cancer mortality Although there are several imaging modalities that may be utilized to identify breast cancer, screening mammography is the main imaging study which is utilized. Mammography is a screening tool that can clearly detect asymptomatic early stage breast cancer which can be identified through calcifications or irregular masses. There is strong support that screening mammography decreases cancer mortality in women over the age of 50, and there is also significant data that supports a decrease in cancer mortality in women age 40 to 49.
 Screening mammogram has been shown to significantly decrease breast cancer mortality. Although there are several imaging modalities that may be utilized to identify breast cancer, screening mammography is the main imaging study which is utilized. Mammography is a screening tool that can clearly detect asymptomatic early stage breast cancer which can be identified through calcifications or irregular masses. There is strong support that screening mammography decreases cancer mortality in women over the age of 50, and there is also significant data that supports a decrease in cancer mortality in women age 40 to 49.")
17
Clinical Breast Exam ACS Recommendations
Should be performed every 3 years for women in their 20-30’s Should be performed annually in women 40 and over Breast self examination starting in the 20’s in optional Women should know how their breasts look and feel so that changes can be promptly reported

18
Mammogram Squeeze Breast flat (up/down) and (side/side), then take a
Film Emory University

20
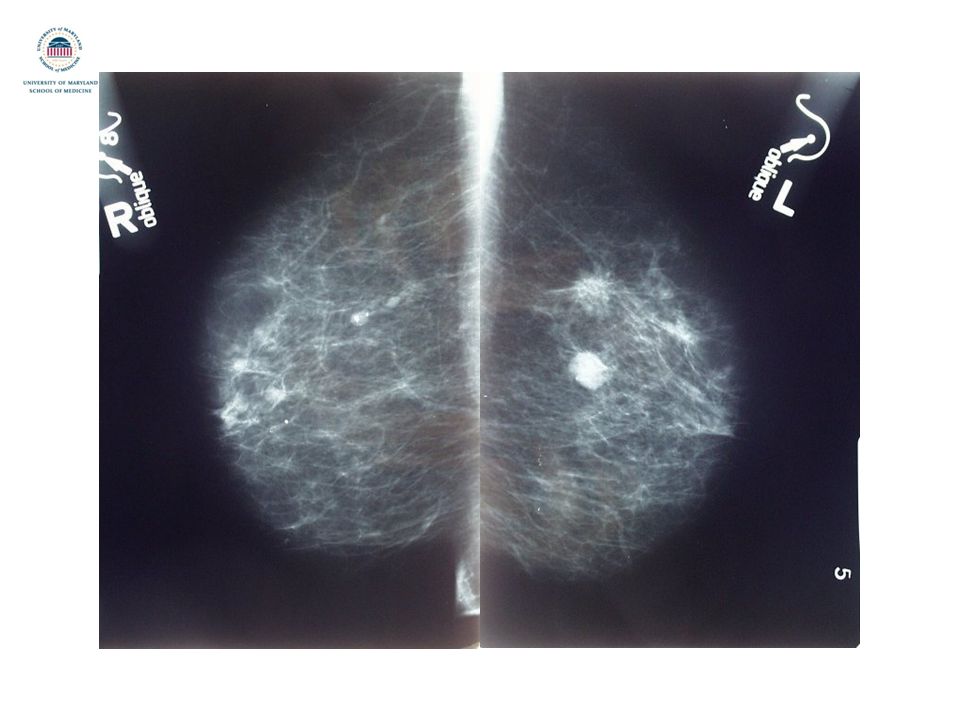
Round and Benign Irregular and Spiculated

22
Ultrasound Usually used as an adjunct to mammogram to further evaluate abnormalities identified. May also be used for primary evaluation of palpable masses that are not seen on mammogram. A second modality that is utilized for evaluating the breast is ultrasound. This is usually used as an adjunct to mammography to visualize additional characteristics of abnormalities which are identified. It can also be

23
Cyst Round Dark Bright Shadow

24
Cancer Dark Shadow Irregular

25
Breast MRI Newer imaging modality that is being utilized for breast evaluation Very good at identifying invasive cancers Also finds a lot of lesions that are not cancers Results in a lot of additional procedures ACS recommendations for screening MRI Patients with defined high risk genetic mutations Patients with an estimated lifetime risk of developing breast cancer of 20-25% (CA Cancer J Clin 2007;57:75–89)
")
26
Bilateral Breast MRI Blood vessels Suspicious ?

27
MRI: spiculated, irregular mass

28
MRI: irregular enhancing mass

29
Stereotactic (Mammogram) Ultrasound Guided MRI Guided
Biopsy Techniques Stereotactic (Mammogram) Ultrasound Guided MRI Guided
 Ultrasound Guided. MRI Guided.")
30
Types of Breast Cancer Non-invasive breast cancer
Ductal carcinoma in situ Lobular carcinoma in situ Invasive breast cancer Ductal carcinoma (75%) Lobular carcinoma (5-10%) Tubular carcinoma (2%) Medullary carcinoma (5-7%) Mucinous/colloid carcinoma (3%) So once a biopsy is taken the pathologist can tell us several things. The first and most important is whether or not this is a cancer. If it is a cancer, then I want to know whether it is a non-invasive cancer or an invasive breast cancer, and to understand the differences between these 2 types of breast cancer I think it will be helpful to first look at the anatomy of the breast and discuss the various changes that can occur.
 Lobular carcinoma (5-10%) Tubular carcinoma (2%) Medullary carcinoma (5-7%) Mucinous/colloid carcinoma (3%) So once a biopsy is taken the pathologist can tell us several things. The first and most important is whether or not this is a cancer. If it is a cancer, then I want to know whether it is a non-invasive cancer or an invasive breast cancer, and to understand the differences between these 2 types of breast cancer I think it will be helpful to first look at the anatomy of the breast and discuss the various changes that can occur.")
31
Breast Anatomy A = Duct B = Lobule C = Dilated duct D = Nipple E = Fat
F = Muscle G = Chest wall A’ = Ductal cell B’ = Basement membrane C’ = Duct center

32
Development of Breast Cancer
Normal cells Cell overgrowth = hyperplasia Atypical cell overgrowth Non-invasive cancer = carcinoma in situ Invasive cancer BRYSON©

33
Breast Cancer Receptors
Hormone receptors Estrogen Progesterone HER-2 gene overexpression Growth factor receptor The other important information that the pathologist can give us is whether or not specific receptors are expressed on the tumor cells and whether there is overexpression of the HER-2 gene which encodes for a growth factor receptor. This information is important because it will help us guide therapy for patients down the road.

34
Clinical Evaluation

35
Clinical Evaluation Risk assessment Current signs and symptoms
Physical exam Visual inspection Palpable mass? Size, location, fixation to chest wall, involvement of skin Palpable lymph nodes? Location, number, size, fixation Review of imaging studies Basically this entire clinical evaluation is helping me determine how extensive the cancer is, and this is something called staging. When patients are diagnosed with cancer we put them into different staging categories based on how advanced the disease is, and this helps to determine prognosis, but it also helps use determine how the patient will be managed. The most important clinical factors in staging breast cancer are the size of the tumor and whether or not the lymph nodes are involved.

36
Staging Clinical Pathologic Physical exam
Imaging (mammogram, ultrasound, MRI, PET/CT) Pathologic Surgical specimen
 Pathologic. Surgical specimen.")
37
Prognostic Factors for Breast Cancer
Tumor size Lymph node involvement Invasive vs. Non-invasive disease Receptor status Age/Menopausal status

38
2002 AJCC Breast Cancer Clinical Staging
Tumor (T) T0 = no evidence of tumor Tis = carcinoma in situ T1 = 0.1 – 2.0 cm T2 = >2.0 – 5.0 cm T3 = >5.0 cm T4 = direct extension to chest wall or skin T4a = extension to chest wall (not including pectoralis major muscle) T4b = skin edema or ulceration, or satellite skin nodules T4c = T4a and T4b T4d = Inflammatory In 2002 the American Joint Committee on Cancer introduced a new staging system for melanoma. This new staging system resulted from a multi-institutional collaborative effort, in which prognostic factors and outcomes were reviewed for almost 18,000 melanoma patients. Prognostic factors were evaluated separately for patients with localized disease, regional disease, and metastatic, and there were several important findings that came out of this analysis. First, for patients with localized disease (stage I or II) it was found that Breslow thickness and ulceration were the most powerful predictors of survival across all T categories, while level of invasion was only significant for thin melanomas. It was shown that there was no clear cutoff for Breslow thickness which truly could be considered a continuous variable, and therefore the T categories were changed to reflect this. In the previous staging system the T categories were odd in that they ranged from , In the new system, the T categories are based on whole numbers. For patients with regional lymph node involvement (stage III) disease, 3 independent prognostic factors were identified, the number of metastatic lymph nodes, the disease burden within the lymph nodes, and whether or not ulceration was present in the primary tumor. It was also noted that there was marked heterogeneity in survival in patients with stage III disease with 5-year survival ranging from 27-70%. In those patients with stage IV disease, non-visceral metastases were found to be associated with a slightly better prognosis. Therefore, the M category was divided based on the site of distant metastasis.
 T0 = no evidence of tumor. Tis = carcinoma in situ. T1 = 0.1 – 2.0 cm. T2 = >2.0 – 5.0 cm. T3 = >5.0 cm. T4 = direct extension to chest wall or skin. T4a = extension to chest wall (not including pectoralis major muscle) T4b = skin edema or ulceration, or satellite skin nodules. T4c = T4a and T4b. T4d = Inflammatory. In 2002 the American Joint Committee on Cancer introduced a new staging system for melanoma. This new staging system resulted from a multi-institutional collaborative effort, in which prognostic factors and outcomes were reviewed for almost 18,000 melanoma patients. Prognostic factors were evaluated separately for patients with localized disease, regional disease, and metastatic, and there were several important findings that came out of this analysis. First, for patients with localized disease (stage I or II) it was found that Breslow thickness and ulceration were the most powerful predictors of survival across all T categories, while level of invasion was only significant for thin melanomas. It was shown that there was no clear cutoff for Breslow thickness which truly could be considered a continuous variable, and therefore the T categories were changed to reflect this. In the previous staging system the T categories were odd in that they ranged from , In the new system, the T categories are based on whole numbers. For patients with regional lymph node involvement (stage III) disease, 3 independent prognostic factors were identified, the number of metastatic lymph nodes, the disease burden within the lymph nodes, and whether or not ulceration was present in the primary tumor. It was also noted that there was marked heterogeneity in survival in patients with stage III disease with 5-year survival ranging from 27-70%. In those patients with stage IV disease, non-visceral metastases were found to be associated with a slightly better prognosis. Therefore, the M category was divided based on the site of distant metastasis.")
39
2002 AJCC Breast Cancer Clinical Staging
Regional lymph nodes (N) NX = regional lymph nodes cannot be assessed N0 = No lymph node metastases N1 = Mets to movable ipsilateral axillary lymph nodes N2 = Mets to fixed/matted ipsilateral axillary lymph nodes or ipsilateral internal mammary nodes w/o axillary nodes N3 = Mets to infraclavicular or supraclavicular nodes or internal mammary & axillary nodes In 2002 the American Joint Committee on Cancer introduced a new staging system for melanoma. This new staging system resulted from a multi-institutional collaborative effort, in which prognostic factors and outcomes were reviewed for almost 18,000 melanoma patients. Prognostic factors were evaluated separately for patients with localized disease, regional disease, and metastatic, and there were several important findings that came out of this analysis. First, for patients with localized disease (stage I or II) it was found that Breslow thickness and ulceration were the most powerful predictors of survival across all T categories, while level of invasion was only significant for thin melanomas. It was shown that there was no clear cutoff for Breslow thickness which truly could be considered a continuous variable, and therefore the T categories were changed to reflect this. In the previous staging system the T categories were odd in that they ranged from , In the new system, the T categories are based on whole numbers. For patients with regional lymph node involvement (stage III) disease, 3 independent prognostic factors were identified, the number of metastatic lymph nodes, the disease burden within the lymph nodes, and whether or not ulceration was present in the primary tumor. It was also noted that there was marked heterogeneity in survival in patients with stage III disease with 5-year survival ranging from 27-70%. In those patients with stage IV disease, non-visceral metastases were found to be associated with a slightly better prognosis. Therefore, the M category was divided based on the site of distant metastasis.
 NX = regional lymph nodes cannot be assessed. N0 = No lymph node metastases. N1 = Mets to movable ipsilateral axillary lymph nodes. N2 = Mets to fixed/matted ipsilateral axillary lymph nodes or ipsilateral internal mammary nodes w/o axillary nodes. N3 = Mets to infraclavicular or supraclavicular nodes or internal mammary & axillary nodes. In 2002 the American Joint Committee on Cancer introduced a new staging system for melanoma. This new staging system resulted from a multi-institutional collaborative effort, in which prognostic factors and outcomes were reviewed for almost 18,000 melanoma patients. Prognostic factors were evaluated separately for patients with localized disease, regional disease, and metastatic, and there were several important findings that came out of this analysis. First, for patients with localized disease (stage I or II) it was found that Breslow thickness and ulceration were the most powerful predictors of survival across all T categories, while level of invasion was only significant for thin melanomas. It was shown that there was no clear cutoff for Breslow thickness which truly could be considered a continuous variable, and therefore the T categories were changed to reflect this. In the previous staging system the T categories were odd in that they ranged from , In the new system, the T categories are based on whole numbers. For patients with regional lymph node involvement (stage III) disease, 3 independent prognostic factors were identified, the number of metastatic lymph nodes, the disease burden within the lymph nodes, and whether or not ulceration was present in the primary tumor. It was also noted that there was marked heterogeneity in survival in patients with stage III disease with 5-year survival ranging from 27-70%. In those patients with stage IV disease, non-visceral metastases were found to be associated with a slightly better prognosis. Therefore, the M category was divided based on the site of distant metastasis.")
40
2002 AJCC Breast Cancer Clinical Staging
Distant metastasis (M) MX = Distant mets cannot be assessed M0 = No distant mets M1 = Distant mets In 2002 the American Joint Committee on Cancer introduced a new staging system for melanoma. This new staging system resulted from a multi-institutional collaborative effort, in which prognostic factors and outcomes were reviewed for almost 18,000 melanoma patients. Prognostic factors were evaluated separately for patients with localized disease, regional disease, and metastatic, and there were several important findings that came out of this analysis. First, for patients with localized disease (stage I or II) it was found that Breslow thickness and ulceration were the most powerful predictors of survival across all T categories, while level of invasion was only significant for thin melanomas. It was shown that there was no clear cutoff for Breslow thickness which truly could be considered a continuous variable, and therefore the T categories were changed to reflect this. In the previous staging system the T categories were odd in that they ranged from , In the new system, the T categories are based on whole numbers. For patients with regional lymph node involvement (stage III) disease, 3 independent prognostic factors were identified, the number of metastatic lymph nodes, the disease burden within the lymph nodes, and whether or not ulceration was present in the primary tumor. It was also noted that there was marked heterogeneity in survival in patients with stage III disease with 5-year survival ranging from 27-70%. In those patients with stage IV disease, non-visceral metastases were found to be associated with a slightly better prognosis. Therefore, the M category was divided based on the site of distant metastasis.
 MX = Distant mets cannot be assessed. M0 = No distant mets. M1 = Distant mets. In 2002 the American Joint Committee on Cancer introduced a new staging system for melanoma. This new staging system resulted from a multi-institutional collaborative effort, in which prognostic factors and outcomes were reviewed for almost 18,000 melanoma patients. Prognostic factors were evaluated separately for patients with localized disease, regional disease, and metastatic, and there were several important findings that came out of this analysis. First, for patients with localized disease (stage I or II) it was found that Breslow thickness and ulceration were the most powerful predictors of survival across all T categories, while level of invasion was only significant for thin melanomas. It was shown that there was no clear cutoff for Breslow thickness which truly could be considered a continuous variable, and therefore the T categories were changed to reflect this. In the previous staging system the T categories were odd in that they ranged from , In the new system, the T categories are based on whole numbers. For patients with regional lymph node involvement (stage III) disease, 3 independent prognostic factors were identified, the number of metastatic lymph nodes, the disease burden within the lymph nodes, and whether or not ulceration was present in the primary tumor. It was also noted that there was marked heterogeneity in survival in patients with stage III disease with 5-year survival ranging from 27-70%. In those patients with stage IV disease, non-visceral metastases were found to be associated with a slightly better prognosis. Therefore, the M category was divided based on the site of distant metastasis.")
41
2002 AJCC Breast Cancer Staging
Stage 0 = Tis N0 M0 Stage I = T1 N0 M0 Stage IIA = T0/1 N1 M0, T2 N0 M0 Stage IIB = T2 N1 M0, T3 N0 M0 Stage IIIA = T0/1 N2 M0, T2 N2 M0, T3 N1/2 M0 Stage IIIB = T4 Any N M0 Stage IIIC = Any T N3 M0 Stage IV = Any T Any N M1 In 2002 the American Joint Committee on Cancer introduced a new staging system for melanoma. This new staging system resulted from a multi-institutional collaborative effort, in which prognostic factors and outcomes were reviewed for almost 18,000 melanoma patients. Prognostic factors were evaluated separately for patients with localized disease, regional disease, and metastatic, and there were several important findings that came out of this analysis. First, for patients with localized disease (stage I or II) it was found that Breslow thickness and ulceration were the most powerful predictors of survival across all T categories, while level of invasion was only significant for thin melanomas. It was shown that there was no clear cutoff for Breslow thickness which truly could be considered a continuous variable, and therefore the T categories were changed to reflect this. In the previous staging system the T categories were odd in that they ranged from , In the new system, the T categories are based on whole numbers. For patients with regional lymph node involvement (stage III) disease, 3 independent prognostic factors were identified, the number of metastatic lymph nodes, the disease burden within the lymph nodes, and whether or not ulceration was present in the primary tumor. It was also noted that there was marked heterogeneity in survival in patients with stage III disease with 5-year survival ranging from 27-70%. In those patients with stage IV disease, non-visceral metastases were found to be associated with a slightly better prognosis. Therefore, the M category was divided based on the site of distant metastasis.
 it was found that Breslow thickness and ulceration were the most powerful predictors of survival across all T categories, while level of invasion was only significant for thin melanomas. It was shown that there was no clear cutoff for Breslow thickness which truly could be considered a continuous variable, and therefore the T categories were changed to reflect this. In the previous staging system the T categories were odd in that they ranged from , In the new system, the T categories are based on whole numbers. For patients with regional lymph node involvement (stage III) disease, 3 independent prognostic factors were identified, the number of metastatic lymph nodes, the disease burden within the lymph nodes, and whether or not ulceration was present in the primary tumor. It was also noted that there was marked heterogeneity in survival in patients with stage III disease with 5-year survival ranging from 27-70%. In those patients with stage IV disease, non-visceral metastases were found to be associated with a slightly better prognosis. Therefore, the M category was divided based on the site of distant metastasis.")
42
Management

43
Multimodality Approach
Surgery Resection and lymph node evaluation Reconstruction Medical therapy Chemotherapy Hormonal therapy Targeted therapy Radiation therapy

44
Surgical Management of Breast
Total Mastectomy Partial Mastectomy vs. + Adjuvant Radiation One of the major advances in the treatment of breast cancer over the last 40 years is a decrease in the extent of surgical resection. At the turn of the 20th century, Dr. Halsted, who was a surgeon at Johns Hopkins Hospital advocated the use of radical mastectomy for patients with breast cancer. This included removal of the breast, lymph nodes, and the chest wall muscles. As you can imagine, this was a very disfiguring procedure and the outcomes were quite poor, mainly because of the late presentation of patients. It was subsequently demonstrated that modified radical mastectomy, which preserves the chest wall muscles was as efficacious as radical mastectomy. And going even further, in the late 70’s and early 80’s it was demonstrated that for earlier stage breast cancer, partial removal of the breast with the addition of radiation therapy resulted in equivalent survival to mastectomy. = overall survival

45
Breast Conservation Therapy Contraindications
Absolute Prior XRT to the breast or chest wall Use of XRT in pregnancy Diffuse suspicious or malignant appearing calcifications Positive margins after multiple excisions Relative Active connective tissue disease involving the skin Multifocal disease that requires 2 incisions Multicentric disease Tumor size greater than 5 cm Focally positive margins after multiple excisions Given these 2 widely accepted surgical approaches to the treatment of breast cancer, which patients with early stage breast cancer are considered candidates for breast conservation therapy? The goal of BCT is to provide optimal cosmetic results without sacrificing local control. Important to the success of BCT is not only a patient’s desire to preserve the breast but the patient’s commitment to preventing advanced recurrences. All patients who undergo BCT must be considered candidates for adjuvant XRT. In addition, patients must understand the importance of lifelong surveillance for recurrence. Therefore, the decision to proceed with BCT is made on an individual basis. Clearly careful patient selection and multidisciplinary care are critical to the success of this approach. There are situations that are considered absolute contraindications to breast conservation therapy. These include prior radiation therapy to the chest wall or breast, use of XRT during pregnancy, diffuse suspicious or malignant appearing calcifications, and positive margins after multiple excisions. And then there are some situations that are considered relative contraindications including active connective tissue disease involving the skin such as lupus or scleroderma, multifocal disease that requires more than one incision for removal, multicentric disease, large tumor size, and focally positive margins after multiple excisions.

46
Surgical Management of Axilla
Axillary lymph node dissection Clinically positive lymph nodes Sentinel lymph node dissection Clinically negative lymph nodes vs.

47
Sentinel Lymph Node Dissection
Lymph Nodes Tumor Radiotracer Vital dye

48
Reconstruction None/Immediate/Delayed Rotational flaps Free flaps
TRAM Latissimus dorsi flap Free flaps DIEP Gluteus Implants +/- flap

49
Medical Therapy

50
Medical Therapy Chemotherapy Hormonal therapy Targeted therapy

51
Chemotherapy Combination chemotherapy Multiple agents are used
Adriamycin Cytoxan Taxanes

52
Hormonal Therapy For hormone receptor positive tumors Tamoxifen
Estrogen receptor + Progesterone receptor + Tamoxifen Selective estrogen receptor modulator Primarily utilized in premenopausal women Aromatase inhibitors Block peripheral production of estrogen Utilized in postmenopausal women Some breast cancers are known to be responsive to circulating hormones and modulation of these hormone levels is one of the methods utilized to decrease the risk of recurrence or the development of new cancers in breast cancer patients.

53
Targeted Agents Herceptin (Trastuzumab) Avastin (Bevacizumab)
Blocks the EGFR (Epidermal Growth Factor Receptor) HER-2 Avastin (Bevacizumab) Anti-angiogenic agent Blocks VEGF (Vascular Endothelial Growth Factor)
 HER-2. Avastin (Bevacizumab) Anti-angiogenic agent. Blocks VEGF (Vascular Endothelial Growth Factor)")
54
Radiation Therapy Partial breast Whole breast
Target the lymph node basins Patient population Patients undergoing breast conservation >= 4 positive axillary lymph nodes Tumors > 5 cm Clinical evidence of internal mammary or supraclavicular nodes

55
Stage Distribution and 5-year Relative Survival by Stage at Diagnosis for , All Races, Females Stage at Diagnosis Stage Distribution (%) 5-year Relative Survival (%) Localized (confined to primary site) 60 98.0 Regional (spread to regional lymph nodes) 33 83.6 Distant (cancer has metastasized) 5 23.4 Unknown (unstaged) 2 57.9 _breast.pdf
 5-year Relative Survival (%) Localized (confined to primary site) Regional (spread to regional lymph nodes) Distant (cancer has metastasized) Unknown (unstaged) _breast.pdf.")
56
Follow-Up Clinical exam, laboratory studies, chest xray every 4-6 months for 5 years and then every 12 months thereafter Diagnostic mammogram every 12 months and 6 months after completion of XRT Annual Gyn exam if on tamoxifen and uterus present Bone mineral testing for patients on aromatase inhibitors or with ovarian failure due to treatment Additional imaging based on patient signs and symptoms

57
Summary Breast cancer is the most common malignancy in women and the second most common cause of cancer death Screening mammogram has significantly changed the presentation and outcomes for patients with breast cancer Management of patients with breast cancer requires a multidisciplinary approach that includes surgery, medical therapy, and radiation SLN bx is an accurate technique that allows for identification of nodes that reflect the disease status of the lymph node basin SLN bx improves staging in patients with melanoma and provides important prognostic information. The technique is currently recommended for all patients with melanoma >1mm in depth. There is still controversy for patients with thin melanoma, but clearly there are groups of patients that have a significantly higher risk of recurrence in whom SLN bx should be considered. It is likely that additional prognostic factors will be considered in future versions of the AJCC staging system that will allow us to refine the staging for patients with melanoma and better select patients for SLN bx.

Similar presentations



: Department.>")
















