Download presentation
Presentation is loading. Please wait.

1
DISC HERNIATIO Lecture 2 Prof.Dr. Sadeq Al-Mukhtar Consultant orthopaedic surgeon

2
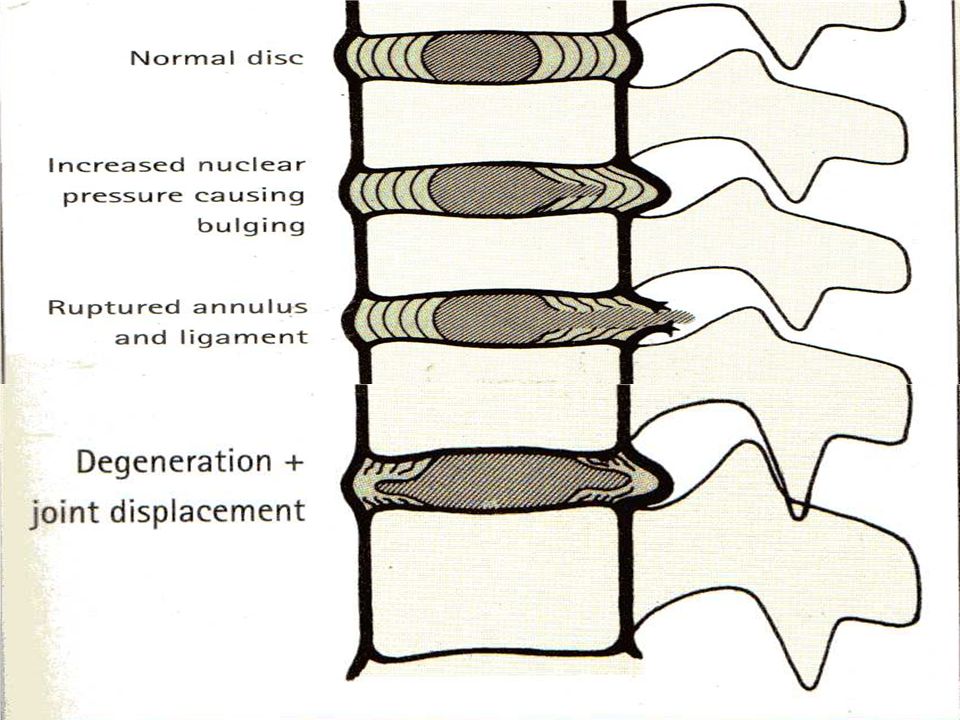
TYPE OF DISC HERNIATION Vertical Herniation Schmorls nodes Horizontal Herniation Protrusion Extrusion Sequestration

3
Site of Herniation Central Herniation: Small Central Massive Central Lateral Herniation: Intermediate Hermiation: Intraforaminal

5
Clinical Features 63% of working adults,age 45-49 years had low back pain. 37% of above having had Sciatica. History: Pain-acute/chronic. Site-Type-Radiation Intermittency of symptoms Parasthesia Loss of sensation or Motor Power Urgency or Frequency of Micturation

6
EXAMINATION Walking and Standing-undressed Gait Supine position-SLR-Test Confirm the test: Bragards test-Dorsiflexion of Ankle. Compression of common P.N. Flexion of Cervical Spine. Contralateral SLR-Test “Well Test”

7
Neurological Examination Muscle weakness and Atrophy Tendon Reflexes: Depressed Ankle(S1,2) Reflex in L5,S1 LEVEL- Examin both Ankles. Compression of L5 Root most commonly cause no reflex change,but sometime causes increased Knee jerk because of weak antagonists. L4 Root lesion result in depressed patellar tendon reflex(L2-4).
..")
8
Differential Diagnosis Bony Abnormalities: Spondylolisthesis/Spondylosis/Spinal canal stenosis. Inflammatory: Discitis/T.B/Acute extradural abscess/Viral radiculitis. Tumors: Ependymoma of filum terminale or conus medullaris/Neuroma/Meningioma. Degenerative: Degenerative lesions of spinal cord and peripheral neuropathies/D.M. Bony nerve Entrapment: Subluxation of facet joints/Narrowing of root canal. Vascular: Peripheral vascular occlusive diseases.

9
INVESTIGATIONS Plain X-Rays Radiculography-Colored Water soluble material injection intrathecal. CT-Scan MRI Haematological test:ESR/Wbc count/Brucella test ….etc. to exclude other differential diagnosis

11
Treatment Conservative:Bed rest-Skin traction for 3 weeks. Surgical: Full Laminectomy. Partial hemi-laminectomy. Fenestration. Micro discectomy-Endoscopic. Chemonucleolysis

12
Thank you

13
SPONDYLOLISTHESIS Lect-3 Prof. Dr.Sadeq Al-mukhtar Consultant orthopaedic surgeon

14
Spondylolisthesis Def: It is forward slippage of a cephalic vertebra on a caudal vertebra. Spondylos (vertebra). Olistharein (slip or fall) Spondylolysis: Greek word lysis (Loosening).It is used to describe a bony defect in the Pars interarticularis”the portion of neural arch just caudal to confluence of pedical and the superior articular process and at the most cephalic part of the lamina and the inferior articular process”.
. Olistharein (slip or fall) Spondylolysis: Greek word lysis (Loosening).It is used to describe a bony defect in the Pars interarticularis the portion of neural arch just caudal to confluence of pedical and the superior articular process and at the most cephalic part of the lamina and the inferior articular process ..")
15
Spondyloptosis: Ptosis is falling.This refers to the most severe form of spondylolisthesis.When the body of L5 has slipped into the pelvis and is positioned directly anterior to the sacrum

16
Clinical Feature: The symptom are caused by chronic muscle contraction(spasm) as the body attempt to limit motion around painful pseudoarthrosis of pars interarticularis by tears of annulus fibrosus of a degenerating disc or by compression of nerve roots.
 as the body attempt to limit motion around painful pseudoarthrosis of pars interarticularis by tears of annulus fibrosus of a degenerating disc or by compression of nerve roots.")
17
In children there is no pain. In adolescents usually back pain of movement particularly with hyper- extension as well as hamstring fatigue and pain,sometimes there are symptoms of sciatica. Over 50 years there is backache.

18
Examination: Flat buttocks. Abnormal transverse loin lines(loin creases). Step of spine. Spine movement: normal in young but restricted in elderly.

19
CLASSIFICATION Wiltse-Newman-Mcnab classification: Type-1:Congenital Dysplastic(20%):- Dysplastic disorder in the posterior elements of upper sacrum. Type-2:Isthmic (50%) :- Three subtypes; a-Lytic-stress fracture of Pars b-Elongated-healed lytic type c-Acute fracture of Pars.
 :- Three subtypes; a-Lytic-stress fracture of Pars b-Elongated-healed lytic type c-Acute fracture of Pars..")
20
Type-3:Degenerative”Pseudospondylosis” 25% Neural arch including pars is intact and olisthesis result from longstanding segmental instability. Type-4: Traumatic ;Fracture of bony hook rather than the pars(articular process).
..")
21
Type-5:Pathological; Generalized or localized bone disease that predisposes to olisthesis. Type -6:Post-surgical; Loss of posterior elements secondary to surgery.e.g:excessive removal of facet or arthrodesis above.

22
Treatment Conservative: Rest,Analgesia,NSAIDS,and physiotherapy. Surgery: Indications- 1-High-grade slip>50%. 2-Intractable pain or neurological signs. 3-Progressive postural deformity or gait abnormality.

23
Types of Surgery Primary repair of pars interarticularis defect under screen” Image intensifire” 1-Instrumental postero-lateral fusion in situ. 2-Arthrodesis. 3-Decompression.

24
Radiological Assessment Plain x-Ray : Anterior and Lateral; Shows the degree of subluxation and also reveal pars interarticularis deficit if present. Oblique views used to see Scott Dog sign. Meyerding classification: Radiological classification Grade -1: 0-25% Grade -2 : 25-50% Grade -3: 50-75% Grade -4 : 75-100% Grade -5 : >100% Slippage is graded as a percentage relative to the sagittal diameter of the inferior body. CT Scan MRI.

25
THANK YOU

Similar presentations





>")














