Download presentation
Presentation is loading. Please wait.

1
The recovery journey Dr David Best Senior Lecturer in Addictions (UoB) Consultant (ACT Research)
 Consultant (ACT Research)")
2
What is a career or lifecourse model?

3
The stages of an addiction or crime career Onset Escalation Persistence Desistance

4
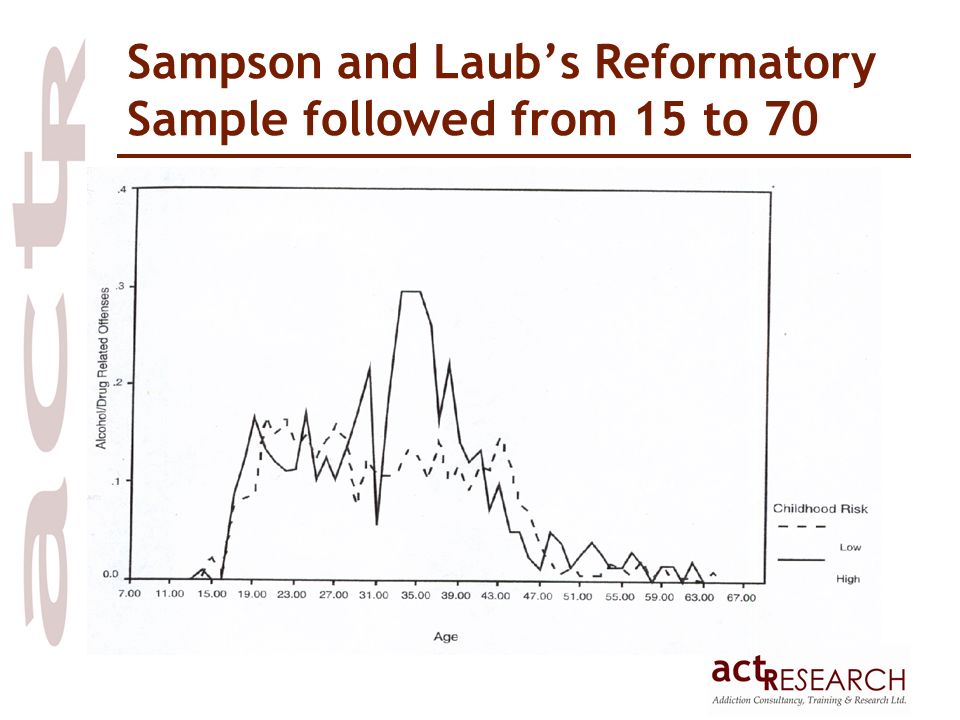
Sampson and Laub’s Reformatory Sample followed from 15 to 70

6
Cambridge Youth Study – Farrington and West Study of 411 boys recruited at age 8 in 1961-62 and followed up to age 32 Data based on the 403 alive at the upper age limit 36% had at least one conviction Of those who had at least one conviction, mean number of convictions was 4.4 Between 16 and 19, offenders were more likely to be hostile to the police, have low job stability, report heavy beer drinking and frequent gambling Between 12 and 15, offenders were more likely to have been frequently truant Between 8 and 11, offenders

7
Number of convictions in Cambridge Youth Study sample

8
So what is unique about the careers perspective? It is generally a model of hope The Laub and Sampson model rejects a risk factors approach in favour of adult growth While recognising the ‘chronic and relapsing’ nature of addiction, this is not seen as a life sentence Key concept of ‘turning points’ Windows of opportunity for change The key turning points are psychological and social not biochemical Links to White’s concept of ‘monocultural’ and ‘bicultural’ social networks

9
Structural Adversity Negative Temperament Ineffective Parenting Early Onset Antisocial Behavior Prosocial Competencies Antisocial Networks Prosocial Competencies Antisocial Networks Antisocial Behavior Prosocial Competencies Antisocial Networks Stability + + ++ + + - - + - + - + - + - + +++ Thornberry Model of Continuity in Anti Social Behaviour

10
So has this model been applied to the addictions field? Hser, Longshore and Anglin (2007): “The life course framework for the study of drug use focuses on long-term patterns of stability and change, both gradual and abrupt, in relation to transitions across the life span and into and out of roles such as patient, offender, spouse, parent, and/or worker” “Transitions, turning points, and social capital are important concepts in understanding processes of change in the life course of drug dependence. The life course of drug use involves onset, acceleration, relapse, and cessation demarcated by major changes in drug use trajectories” “Relative to onset and relapse, stable cessation is the least studied phenomenon in drug abuse research. Despite the theoretical and policy importance of understanding why people stop using and are able to maintain abstinence, we do not have robust conceptual models or rich empirical investigations of cessation”.
: The life course framework for the study of drug use focuses on long-term patterns of stability and change, both gradual and abrupt, in relation to transitions across the life span and into and out of roles such as patient, offender, spouse, parent, and/or worker Transitions, turning points, and social capital are important concepts in understanding processes of change in the life course of drug dependence. The life course of drug use involves onset, acceleration, relapse, and cessation demarcated by major changes in drug use trajectories Relative to onset and relapse, stable cessation is the least studied phenomenon in drug abuse research. Despite the theoretical and policy importance of understanding why people stop using and are able to maintain abstinence, we do not have robust conceptual models or rich empirical investigations of cessation ..")
11
Addiction careers

12
So what role does treatment play? In the developmental criminology model, interventions are accorded very little importance In our model, we hypothesise that rehab offers the possibility of a turning point However, there is a risk that maintenance treatment may medicate people over the recovery window Our programme of research has tried to address the lack of attention paid to cessation factors and long-term recovery predictors Two components to our research programme –“end of careers study” –“recovery journeys and communities”

13
1. End Of Careers Study Sample of 187 former addicts (alcohol, cocaine and heroin) currently working in the addictions field, from total group of 269 former users 70% male Mean age = 45 years 92% white Worked in the field for an average of 7 years Typical heroin career of around 10 years Best et al (2008)
 currently working in the addictions field, from total group of 269 former users 70% male Mean age = 45 years 92% white Worked in the field for an average of 7 years Typical heroin career of around 10 years Best et al (2008).")
14
What finally enabled participants to give up? Not at allA littleQuite a lotA lot Physical health problems19.6%42.4%15.2%22.8% Psychological health problems23.4%18.1%22.3%36.2% Criminal justice30.4%26.1%19.6%23.9% Family pressures36.0%24.7%21.3%18.0% Work opportunities76.5%9.4% 4.7% Support from partner72.6%15.5%6.0% Help from friends37.9%28.7%14.9%18.4% Tired of lifestyle6.3%4.2%13.5%76.0%

15
What enabled people to maintain abstinence? Not at allA littleQuite a lotA lot Support from a partner45.2%20.0%12.9%21.9% Support from friends14.5%21.1%16.9%47.6% Moving away from drug using friends 16.1%5.0%18.0%60.9% Having a job31.2%17.8%18.5%32.5% Having reasonable accommodation 10.3%17.6%26.1%46.1% Religious or spiritual beliefs22.3%11.4%16.3%50.0%

16
Current recovery research sample (n=269) Alcohol users only Alcohol and drugs Drug users only Wave 1 data collection 62 (32.6%)36 (18.9%)92 (48.4%) Wave 2 data collection 36 (45.6%)31 (39.2%)12 (15.2%) Total98 (36.4%)67 (24.9%)104 (38.7%)
 Alcohol users only Alcohol and drugs Drug users only Wave 1 data collection 62 (32.6%)36 (18.9%)92 (48.4%) Wave 2 data collection 36 (45.6%)31 (39.2%)12 (15.2%) Total98 (36.4%)67 (24.9%)104 (38.7%)")
17
Reasons for achieving detoxification by group Reasons for achieving abstinence Heroin only Alcohol only Both heroin and alcohol Χ, sig Physical health74.4%73.5%82.1%1.10 Psychological health75.3%81.8%76.2%0.61 Criminal justice factors64.0%42.1%67.6%8.54* Work opportunities21.1%44.6%21.1%10.19** Tired of the lifestyle95.3%90.8%100.0%4.81 Family and friends55.7%69.6%56.4%0.18

18
Reasons for sustaining abstinence by group Reasons for sustaining abstinence Heroin only Alcohol only Both H & A Χ, sig Support from partner31.0%47.1%22.7%5.83 Support from friends66.7%55.4%63.6%2.37 Moving away from substance using friends 84.4%60.4%91.7%14.63** Having a job41.9%48.1%50.0%2.25 Having reasonable accommodation 72.4%60.3%90.5%8.59* Religious or spiritual factors55.8%66.7%69.6%3.22

19
Key qualitative themes Key role of social learning Need to complement recovery belief with recovery of esteem and learning of skills People may move through and beyond mutual aid groups Incompatibility of treatment and mutual aid pathways

20
2. Mapping recovery journeys 3-stage process: 1.Identification of support groups and mutual aid groups in local communities 2.Access each group and describe their origins, aims, affiliations and links 3.Map the recovery journeys of individuals both linked to recovery groups and those who either no longer engage in groups or never did – including the use of the Lifetime Drug Use History (Best et al, 2007, Day et al, 2007)
.")
21
Heroin use Crimes committed Criminal Justice System Shoplifting Theft 1112131415161718 Chasing daily 0.5 gr Daily 0.6 Chasing daily 0.9 gr/d cannabis Sniffing solvents Crack cocaine Young Person Every day £100 Twice a month £1- £50 Every day £100-£1000 13 days/30 0.3 grs Supervision Order robbery 11 months Remand Awaiting trial Robbery 8 Months Robbery 0 8 Months Remand Kidnap Arson Every day £100 Charges dropped Kidnap 2 years probation arson Harmful use of Alcohol Buying illicit Benzodiazepines

22
Heroin use 1112131415161718 Treatment Life Events Young Person Chasing daily 0.5 gr Daily 0.6 Chasing daily 0.9 gr/d 13 days/30 0.3 grs Conduct disorder School for children Behavioural Problems Living with mother and siblings cannabis Sniffing solvents Harmful use of Alcohol Buying illicit Benzodiazepines Social Services Children’s Home Girlfriend 1: opioid dependence+alcohol dependence Social Services Children’s Home Moved in to live with Dad And step brother Brought By Social worker Slade Road Centre Methadone Px Poor Motivation Dropped Out Went to prison Education Employment Housing Relationships

23
Heroin use Crimes committed Criminal Justice System Shoplifting Dealing heroin 1920212223242526 2728 Chasing daily 0.5 grs Chasing 1 gr/d Robbery 1 year Chasing 0.5 gr/d Chasing 17/7 0.6-0.3 0.6 ch Alcohol Dependence Syndrome Crack cocaine Adulthood Every day £100 £ 1000+ Chasing 17/30 0.6 grs 9 months In prison Chasing 9/30 0.6 grs week 9 months Theft Benzodiazepine dependence syndrome 2 gr/d 21/30 £300 Burglary £3500 Remand 5 months DTTO Fraud Car theft 18 months Probation

24
Heroin use 1920212223242526 Treatment Life Events 27 28 Adulthood Chasing daily 0.5 grs Chasing 1 gr/d Chasing 0.5 gr/d Chasing 17/7 0.6-0.3 0.6 ch Chasing 17/30 0.6 grs Chasing 9/30 0.6 grs week 2 gr/d Education Employment Housing Relationships Girlfriend 1 Birth baby Joshua Dad Brother die Hostels Flat with G1 Benefits Income Support Job Seekers Girlfriend 2: OD Crack cocaine Alcohol Dependence Syndrome Benzodiazepine dependence syndrome G 2: flat Own flat G 2: flat B Chloe SRC Methadone Diazepam Px DTTO Inpatient Alcohol Detox Opioid +Benzo stabilisation SRC Day Centre Residential Rehab GP: banned fraud Banned visiting baby overdoses

25
So what are the aims of this work? To identify types of recovery journey, assessing the role of key life events as turning points To map the role of mutual aid and other support groups in the recovery journeys To identify the impact that treatment engagement has on recovery To characterise the recovery experiences and pathways of maintained versus abstinent recovery To provide an evidence base for hope and to chart what can be done to enable recovery communities To support the generation of ‘tipping points’ around long-term recovery communities

Similar presentations










 Theories>")



 National Institutes of Health Bethesda,>")




