Download presentation
Presentation is loading. Please wait.

1
Diuretics: drugs that affect the renal system

2
Learning Objectives After studying this content, the student will be able to: Review normal distribution of water/fluid volume in the human body. Review capillary forces (hydrostatic and oncotic pressure) that determine filtration vs. reabsorption in capillaries under normal, healthy conditions. Review the major functions of the kidneys; the functionally distinct sections of the renal nephron; and describe how water is reabsorbed from the tubular fluid. In general, describe the primary therapeutic uses of diuretics and the broad types of adverse effects. Describe the mechanism of action that most diuretics have in common. List the four major classes of diuretics; describe mechanism / site of action in nephron, clinical uses, side effects, and any key considerations. Describe the relative efficacy of loop diuretics, thiazides, and potassium-sparing diuretics in increasing urine output. Describe several ways by which renal function can be monitored. Describe parameters used in monitoring patients undergoing drug therapy with diuretics. Pay particular attention to safety considerations. Highlight key considerations regarding patient education for diuretic therapy.
 that determine filtration vs. reabsorption in capillaries under normal, healthy conditions. Review the major functions of the kidneys; the functionally distinct sections of the renal nephron; and describe how water is reabsorbed from the tubular fluid. In general, describe the primary therapeutic uses of diuretics and the broad types of adverse effects. Describe the mechanism of action that most diuretics have in common. List the four major classes of diuretics; describe mechanism / site of action in nephron, clinical uses, side effects, and any key considerations. Describe the relative efficacy of loop diuretics, thiazides, and potassium-sparing diuretics in increasing urine output. Describe several ways by which renal function can be monitored. Describe parameters used in monitoring patients undergoing drug therapy with diuretics. Pay particular attention to safety considerations. Highlight key considerations regarding patient education for diuretic therapy.")
3
Review

4
Normal Distribution of Water in the Human Body
Under normal healthy conditions, total body water is properly distributed between body compartments Total body water comprises ~ % of body weight How is TBW distributed? Intracellular fluid (ICF) = 66% of total body water Extracellular fluid (ECF) = 33% of total body water Interstitial fluid 75% of ECF Plasma 25% of ECF Na+ Cl- Bicarbonate K+ PO4-
 = 66% of total body water. Extracellular fluid (ECF) = 33% of total body water. Interstitial fluid 75% of ECF. Plasma 25% of ECF. Na+ Cl- Bicarbonate. K+ PO4-")
5
Distribution of body water depends on forces acting on the water molecules and on the permeability of tissues Vocabulary: Hydrostatic pressure Oncotic pressure Capillary permeability “Net” force Filtration Reabsorption

6
Hydrostatic Pressure and Oncotic Pressure
Hydrostatic pressure refers to the pressure that a fluid exerts on the walls of its container (think of a balloon filled with water.) The main cause of hydrostatic pressure in the circulatory system is the force of blood on the blood vessel walls (ie “Blood pressure”) Oncotic pressure is a form of osmotic pressure exerted by proteins (notably albumin), typically in the blood plasma Capillary permeability can be thought of as the “leakiness” of the capillary endothelium; ie the capacity of the microvasculature to allow small molecules (eg ions, water, nutrients) or even whole cells (eg lymphocytes on their way to the site of inflammation) to flow out of, or into, a capillary
 The main cause of hydrostatic pressure in the circulatory system is the force of blood on the blood vessel walls (ie Blood pressure ) Oncotic pressure is a form of osmotic pressure exerted by proteins (notably albumin), typically in the blood plasma. Capillary permeability can be thought of as the leakiness of the capillary endothelium; ie the capacity of the microvasculature to allow small molecules (eg ions, water, nutrients) or even whole cells (eg lymphocytes on their way to the site of inflammation) to flow out of, or into, a capillary.")
7
Hydrostatic and Oncotic Pressure
Hydrostatic pressure and oncotic pressure are opposing forces in blood vessels. Under normal conditions, hydrostatic pressure tends to “push” fluid out of the capillary (filtration) whereas oncotic pressure tends to “pull” fluid into the capillary (reabsorption) The “net force” determines whether filtration or reabsorption occurs at any single location along the capillary microvasculature net Opposing forces are equal in magnitude net
 whereas oncotic pressure tends to pull fluid into the capillary (reabsorption) The net force determines whether filtration or reabsorption occurs at any single location along the capillary microvasculature. net. Opposing forces are equal in magnitude. net.")
8
Questions?

9
Kidneys and Diuretics The kidneys have three basic functions:
Maintain plasma (ECF) volume and composition Maintenance of acid-base balance Excretion of metabolic wastes and foreign substances Diuretics are used primarily to decrease plasma fluid volume: Diuretics promote excretion of water To do this, diuretics must interfere with the normal operation of the kidney Adverse effects of diuretics may include: Hypovolemia Acid-base imbalance Altered electrolyte levels 9
 volume and composition. Maintenance of acid-base balance. Excretion of metabolic wastes and foreign substances. Diuretics are used primarily to decrease plasma fluid volume: Diuretics promote excretion of water. To do this, diuretics must interfere with the normal operation of the kidney. Adverse effects of diuretics may include: Hypovolemia. Acid-base imbalance. Altered electrolyte levels. 9.")
10
Therapeutic Uses of Diuretics
1- *Treatment of hypertension 2- *Mobilization of edematous fluid eg heart failure, liver failure, kidney disease, other There are many causes of edematous states, but they share the common characteristic in that the normal distribution of body water is altered 3- used to prevent renal failure How do diuretics promote excretion of water? By reducing the amount of water reabsorbed from tubular filtrate Let’s review function of the nephron

11
Basic Nephron Anatomy The nephron is the functional unit of kidney
Each kidney has about one million nephrons Nephron micro-anatomy Glomerulus Proximal convoluted tubule Loop of Henle Descending Ascending Distal convoluted tubule Collecting duct

12
Basic nephron processes
Filtration:~ 20% of the plasma that flows through the glomerular capillaries gets filtered into Bowman’s Capsule (180 liters filtrate produced daily) Occurs only at glomerulus Reabsorption: more than 99% of the water, nutrients and ions get reabsorbed. Na reabsorption creates osmotic gradient. Cl may be co-absorbed or passively follow the sodium “Water follows salt.” By reabsorbing sodium from the tubular fluid, water also gets reabsorbed from tubular fluid. Occurs at several highly specific locations in nephron Active secretion: various wastes, drugs and toxins Occurs at PCT Net result: 1.5 – 2 liters of urine produced daily
 Occurs only at glomerulus. Reabsorption: more than 99% of the water, nutrients and ions get reabsorbed. Na reabsorption creates osmotic gradient. Cl may be co-absorbed or passively follow the sodium. Water follows salt. By reabsorbing sodium from the tubular fluid, water also gets reabsorbed from tubular fluid. Occurs at several highly specific locations in nephron. Active secretion: various wastes, drugs and toxins. Occurs at PCT. Net result: 1.5 – 2 liters of urine produced daily.")
13
Diuretic Agents MOA: most diuretics block reabsorption of sodium and chloride from the tubular fluid Specific diuretics block reabsorption of sodium and chloride at specific locations in the nephron. See next slide for locations where the four major classes of diuretics work By blocking the reabsorption of sodium and chloride, osmotic pressure is developed within the tubules: this osmotic pressure holds water within the tubules… resulting in this fluid being eliminated from the body in urine

15
Four major classes of diuretics
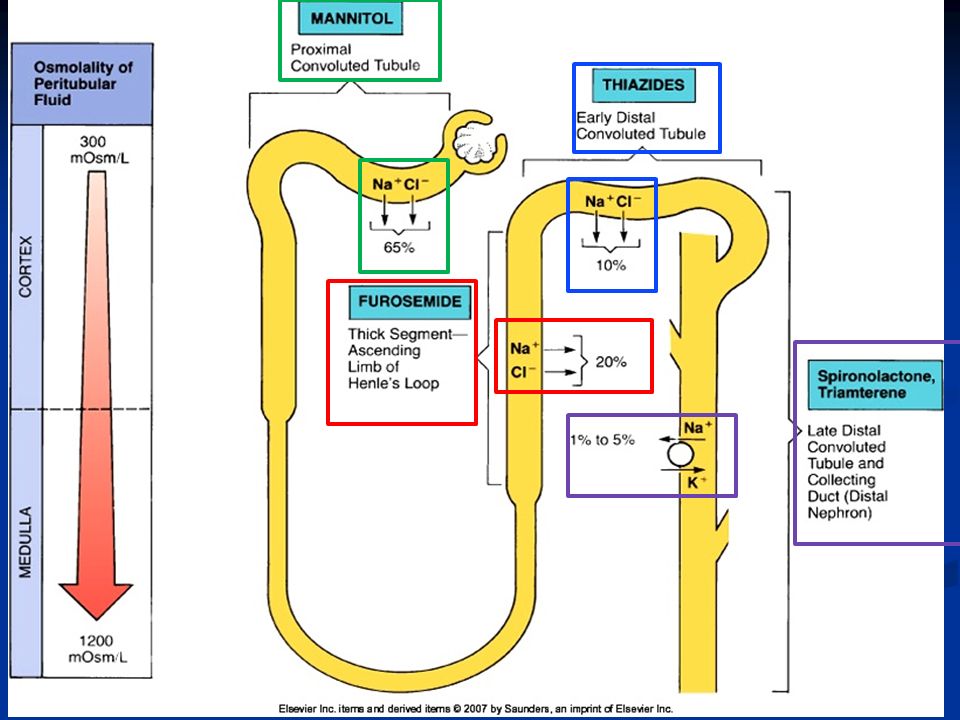
Osmotic diuretics- have a unique MOA Highly osmotic molecules that are freely filtered at the glomerulus, and drag water into the filtrate too (non-reabsorbed, non-metab’d) Loop diuretics- Block reabsorption of Na, Cl in the Loop of Henle Thiazides- Block reabsorption of Na, Cl in the early Distal Convoluted Tubule Potassium-sparing diuretics Block reabsorption of sodium and prevent the excretion of potassium in the collecting duct
 Loop diuretics- Block reabsorption of Na, Cl in the Loop of Henle. Thiazides- Block reabsorption of Na, Cl in the early Distal Convoluted Tubule. Potassium-sparing diuretics. Block reabsorption of sodium and prevent the excretion of potassium in the collecting duct.")
16
Osmotic Diuretics Mannitol = caution! Must be used with CAUTION!
Mannitol is a highly osmotic molecule (draws water to it) Mannitol cannot cross BBB, but CAN leave vascular system at all other capillaries (risk of edema!) Used mainly in acute settings for very specific indications such as to reduce intracranial pressure (eg head injuries) reduce intraocular pressure Mechanism & Site of Action: filtered at glomerulus, pulling water along with it. Not reabsorbed, not metabolized. Increases osmotic gradient in lumen of nephron. Results in increased urine production.
 Mannitol cannot cross BBB, but CAN leave vascular system at all other capillaries (risk of edema!) Used mainly in acute settings for very specific indications such as. to reduce intracranial pressure (eg head injuries) reduce intraocular pressure. Mechanism & Site of Action: filtered at glomerulus, pulling water along with it. Not reabsorbed, not metabolized. Increases osmotic gradient in lumen of nephron. Results in increased urine production.")
17
Osmotic Diuretics Pharmacokinetics
Onset 1-3 hours, half-life 1-2 hours Dosing Mannitol gm/kg IV Q4-6 hours Adverse Effects Edema! Extreme Caution if CHF, risk of pulmonary edema Headache N/V Fluid & Electrolyte imbalances!!! Again, use caution! Watch for dehydration! Drug Specifics

18
Loop Diuretics Loop diuretics are the MOST EFFECTIVE diuretic available! And result in more fluid and electrolyte loss than any other diuretic! Effective even when the glomerular filtration rate (GFR) is low (ie, when urine output is decreased) Mechanism and Site of Action Inhibit sodium and chloride reabsorption in the ascending limb of the Loop of Henle Avoid when less efficacious agents will suffice
 is low (ie, when urine output is decreased) Mechanism and Site of Action. Inhibit sodium and chloride reabsorption in the ascending limb of the Loop of Henle. Avoid when less efficacious agents will suffice.")
19
Loop Diuretics Furosemide (prototype) is most commonly prescribed
Therapeutic uses: Pulmonary edema Edematous states Hypertension PO, IV, IM IV route for emergency use (eg pulmonary edema) that requires immediate mobilization of fluid; ICU setting- continuous infusion Pharmacokinetics Rapid absorption, GI edema may impair, highly protein bound, hepatic metabolism, renal elimination Dosing: Furosemide (Lasix) mg/day PO/IV (“average” dose mg/day) Bumetanide 2-8mg/day PO/IV Torsemide mg/day PO/IV
 that requires immediate mobilization of fluid; ICU setting- continuous infusion. Pharmacokinetics. Rapid absorption, GI edema may impair, highly protein bound, hepatic metabolism, renal elimination. Dosing: Furosemide (Lasix) mg/day PO/IV ( average dose mg/day) Bumetanide 2-8mg/day PO/IV. Torsemide mg/day PO/IV.")
20
Loop Diuretics Adverse Effects
Electrolyte Imbalances! Hyponatremia, hypochloremia! Hypokalemia- is especially problematic for patients taking digoxin Hypotension Dehydration- sequellae include falls, venous thrombosis Signs of dehydration? DVT? Electrolyte abnormalities? Hyperglycemia; Hyperuricemia; Use in pregnancy Impact on lipids, calcium, and magnesium Ototoxicity- rare: hearing loss is usually transient vs irreversible Hypersensitivity Drug Interactions- digoxin, ototoxic drugs, potassium-sparing diuretics, lithium, anti-hypertensives, NSAIDS Drug Specifics Torsemide has better absorption with GI edema Continuous IV infusion may improve diuresis over bolus dosing

21
Thiazides and related Diuretics
Mechanism and Site of Action Prevent sodium resorption in the distal convoluted tubule Thiazide diuretics produce less diuresis than loop diuretics Thiazide diuretics are ineffective when the GFR is low, ↓urine output Risk of dehydration and hypokalemia But do not cause hearing loss. Thiazide-induced hypokalemia is a special problem for patients taking digoxin Increase excretion of Na, Cl, K & water Can elevate blood glucose and plasma uric acid

22
Thiazide Diuretics Pharmacokinetics
Good absorption, renal elimination, onset 1-2 hours Therapeutic uses: Essential hypertension Edema Diabetes insipidus Dosing Hydrochlorothiazide 25-50mg PO Qday Most widely used Chlorothiazide mg PO/IV q6-12hrs Metolazone mg PO Qday

23
Thiazide Diuretics Adverse Effects
Electrolyte imbalances- hyponatremia, hypochloremia, hypokalemia Dehydration Use in pregnancy and lactation Hyperglycemia; Hyperuricemia; Impact on lipids, calcium, and magnesium May precipitate gout Drug interactions- like loop diuretics Drug Specifics Chlorothiazide the only IV thiazide Metolazone only thiazide to work in patients with moderate-severe renal dysfunction HCTZ= Drug interactions Digoxin Augments effects of hypertensive medications Can reduce renal excretion of lithium (leading to accumulation) NSAIDs may blunt diuretic effect Can be combined with ototoxic agents without increased risk of hearing loss
 NSAIDs may blunt diuretic effect. Can be combined with ototoxic agents without increased risk of hearing loss.")
24
Potassium Sparing Diuretics
Produce only a modest increase in urine production, but a substantial decrease in potassium excretion Often used in conjunction with a loop or thiazide diuretic, to counteract losses of potassium Mechanism and Site of Action Decrease sodium absorption in distal convoluted tubule Results in K+ absorption, and excretion of sodium

25
Potassium Sparing Diuretics
Therapeutic uses Hypertension Edematous states Heart failure (decreases mortality in severe failure) Primary hyperaldosteronism Premenstrual syndrome Polycystic ovary syndrome Acne in young women
 Primary hyperaldosteronism. Premenstrual syndrome. Polycystic ovary syndrome. Acne in young women.")
26
Potassium Sparing Diuretics: key considerations
The principal adverse effect of potassium-sparing diuretics is hyperkalemia. Potassium-sparing diuretics should not be combined with one another or with potassium supplements They should be used cautiously in patients taking angiotensin-converting enzyme (ACE) inhibitors, angiotensin-receptor blockers, or direct renin inhibitors.
 inhibitors, angiotensin-receptor blockers, or direct renin inhibitors.")
27
Potassium Sparing Diuretics
Oral agents Spironolactone- delayed effects (up to 48 hours); used for HTN, edema Reduces mortality and hospital admissions in CHF pts Risk of hyperkalemia Endocrine effects include gynecomastia, menstrual irregularities, impotence hirsutism, deepening of the voice Triamterene- Amiloride- Dosing Spironolactone: mg PO Qday-BID Triamterene: mg PO Qday-BID Amiloride: mg PO Qday
; used for HTN, edema. Reduces mortality and hospital admissions in CHF pts. Risk of hyperkalemia. Endocrine effects include gynecomastia, menstrual irregularities, impotence hirsutism, deepening of the voice. Triamterene- Amiloride- Dosing. Spironolactone: mg PO Qday-BID. Triamterene: mg PO Qday-BID. Amiloride: 5-10mg PO Qday.")
28
Potassium Sparing Diuretics
Adverse Effects Electrolyte imbalances Dehydration Impotence Gynecomastia- become tender/ painful (spironolactone) Drug Specifics Weak diuretic effect Most often used in combination w/ thiazides Spironolactone useful in patients with liver failure and ascites (high aldosterone levels) avoid concomitant use with other agents that can raise potassium levels
 Drug Specifics. Weak diuretic effect. Most often used in combination w/ thiazides. Spironolactone useful in patients with liver failure and ascites (high aldosterone levels) avoid concomitant use with other agents that can raise potassium levels.")
29
General Considerations of Diuretic Therapy

30
Monitoring Renal Function
Creatinine Clearance Cockcroft-Gault Equation- has an adjustment for age, as well as gender-based differences in serum creatinine levels Urine Output: 0.5-1 mL/kg/hr Intake and Output Electrolytes Sodium

31
Monitoring Parameters
Therapeutic Urine Output Daily weights- same time every day usually right after the first morning void Laboratory Na, Hct Other- K, Ca, Mg Adverse Effects Electrolytes Hemodynamics- fluid volume, blood pressure,

32
Patient Education Purpose Duration Timing- don’t take at bedtime
Symptoms Therapeutic- Adverse effects Dietary Considerations Sodium Potassium Fluids

33
Drug-Induced Nephrotoxicity
Antibiotics Aminoglycosides (gentamicin, tobramycin) Antifungals (Amphotericin B) Vancomycin Non-steroidal anti-inflammatory drugs Ibuprofen, et. al. Angiotensin converting enzyme (ACE) inhibitors Captopril, Lisinopril Hypersensitivity reactions Cancer chemotherapy drugs Cisplatin Cyclophosphamide, Ifosfamide
 Antifungals (Amphotericin B) Vancomycin. Non-steroidal anti-inflammatory drugs. Ibuprofen, et. al. Angiotensin converting enzyme (ACE) inhibitors. Captopril, Lisinopril. Hypersensitivity reactions. Cancer chemotherapy drugs. Cisplatin. Cyclophosphamide, Ifosfamide.")
34
Patient Case TR, slide 1 TR is a 62 YO WM who presents in clinic complaining of some difficulty breathing while lying down at night, and increased swelling in his feet and ankles. He is diagnosed with mild congestive heart failure secondary to ischemic heart disease, and is placed on hydrochlorothiazide 50mg PO QD.

35
Patient Case TR, slide 2 What do you think is probably causing this patient’s symptoms? What parameters are important to monitor in this patient with respect to: Therapeutic effect? Adverse effects? What instructions does this patient need to ensure appropriate therapy?

36
Patient Case NK, slide 1 NK is a 74 YO WM, POD 6 from CABG surgery. He is on 3L O2, with bilateral crackles in the bases. Weight is 104.4kg (preop 98kg). His renal function is mildly impaired, with a creatinine of 1.9 mg/dl. What diuretic would be appropriate for this patient?
. His renal function is mildly impaired, with a creatinine of 1.9 mg/dl. What diuretic would be appropriate for this patient")
37
Patient Case NK, slide 2 What monitoring parameters should be followed? What are some options if the patient doesn’t respond?

Similar presentations













. Other excretory.>")
 of urine.>")




