Download presentation
Presentation is loading. Please wait.

1
Diuretics

2
A. Kidney functions Kidneys have a number of essential functions:

3
1. excretion

4
2. regulate: fluid balance electrolyte composition acid-base balance

5
3. secrete enzyme renin

6
4. secrete erythropoietin (a hormone that stimulates RBC production)
")
7
5. produce calcitriol, the active form of vitamin D, which helps maintain bone homeostasis

8
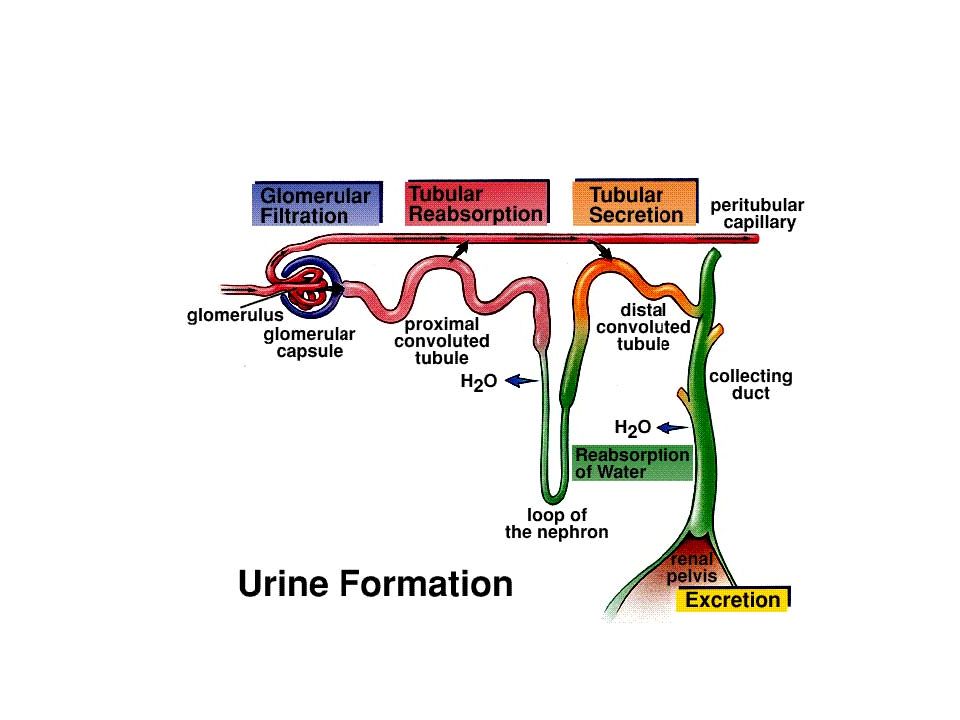
B. Kidney structure Each kidney contains more than 2 million nephrons, the functional unit of the kidney.

9
Each nephron is composed of several parts: glomerulus proximal convoluted tubule (PCT) loop of Henle distal convoluted tubule (DCT) collecting ducts
 loop of Henle distal convoluted tubule (DCT) collecting ducts")
10
The glomerulus is the site where filtration of substances in the blood occurs.

11
Small molecules, electrolytes and water are filtered from the blood into the glomerular filtrate by passing through filtration slits and pores.

12
Molecules small enough to be filtered include: amino acids creatinine certain drugs electrolytes glucose urea, uric acid certain vitamins

13
They generally have a diameter < 8 nm.

14
Substances in the blood greater than 8 nm are retained in the blood, and include: blood cells plasma proteins (i.e. albumin) hormones
 hormones.")
15
The rest of the nephron (PCT, loop of Henle and DCT) is involved with either: reabsorbing many of these small molecules, electrolytes, and water and transporting them back into the blood
 is involved with either: reabsorbing many of these small molecules, electrolytes, and water and transporting them back into the blood")
16
Water is the most important molecule re- absorbed.

17
For every 180 liters (47 gallons) of water entering the filtrate each day, 178.5 liters are reabsorbed, leaving only 1.5 liters to be excreted in the urine.
 of water entering the filtrate each day, liters are reabsorbed, leaving only 1.5 liters to be excreted in the urine.")
18
or, secreting other waste products from the blood to the filtrate for removal in urine

19
After leaving the glomerulus the filtrate enters the PCT.

20
The PCT is the site where water, electrolytes (Na 1+, Cl 1-, and HCO 3 1- ), glucose and amino acids are reabsorbed.
, glucose and amino acids are reabsorbed.")
21
After leaving the PCT, the filtrate travels through the loop of Henle. This is the site of tubular reabsorption of water, Na 1+, K 1+, Ca 2+, Mg 2+, Cl 1-, and HCO 3 1-.

22
Next, the filtrate passes through the DCT. This is the site of tubular reabsorption of most ions including Na 1+, K 1+, Ca 2+, Mg 2+, Cl 1-, and HCO 3 1-.

23
The convoluted part of the distal tubule is virtually impermeable to water and urea.

24
The late distal tubule has a varying permeability to water, depending on the concentration of ADH.

25
When ADH is elevated, water is reabsorbed. In the absence of ADH, water is not reabsorbed.

26
Then the filtrate passes into tubes called collecting ducts where water may be reabsorbed, again dependent on ADH levels.

28
Diuretics are drugs that increase urine output.

29
This is considered a desirable effect in the treatment of the following conditions:

30
hypertension (HT) heart failure (HF) kidney failure pulmonary edema liver failure or cirrhosis
 heart failure (HF) kidney failure pulmonary edema liver failure or cirrhosis")
31
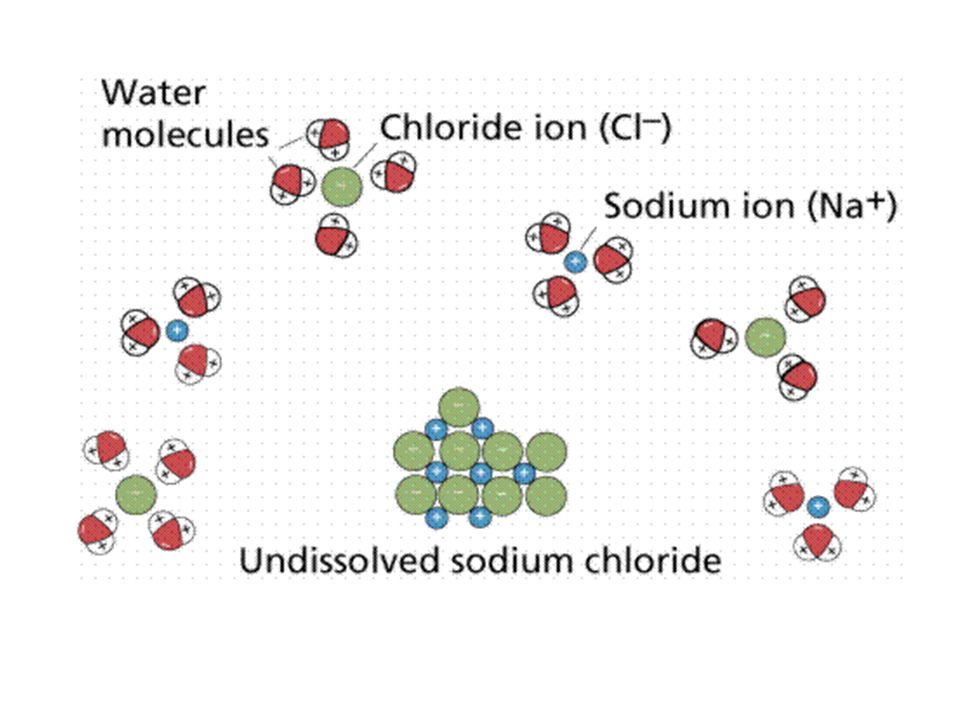
The most common way in which diuretics act is by blocking sodium reabsorption in the nephron, thus sending more of this ion into the urine.

32
Chloride ion also follows sodium

33
Water molecules also stay with both of these ions

35
Therefore, blocking the reabsorption of sodium will keep more water in the filtrate.

36
The more water retained in the filtrate, the greater the volume of urination, or diuresis.

37
C. Categories of diuretics

38
1. Thiazide diuretics Thiazide diuretics are some of the most widely used of the diuretic drugs.

39
The site of diuretic action for the thiazide diuretics is the early DCT.

40
Thiazides are the preferred diuretic in the treatment of HT, mild HF, and certain renal disease (nephrolithiasis, nephrogenic diabetes insipidus).
.")
41
They cause a greater diuresis than the K 1+ sparing diuretics, but a lesser diuresis than the organic acid diuretics.

42
They are the only diuretics which decrease Ca 2+ excretion.

43
This results in a mild increase in serum Ca 2+ levels, which decreases bone resorption (release of Ca 2+ from bone).
.")
44
They would be recommended for patients at risk of osteoporosis.

45
The distal tubule is the main site in the nephron for the secretion of K 1+, normally in exchange for Na 1+.

46
Thiazide diuretics work by inhibiting sodium reabsorption which increases its excretion, along with Cl 1- and substantial amounts of water.

47
Thiazides do not interfere with K 1+.

48
Thiazide diuretics include: chlorothiazide (diuril): 500 mg – 2,000 mg/day for both HT, edema. Duration: 6 – 12 hours

49
hydrochlorothiazide (HydroDIURIL, Hydropar, Ezide): 25 - 50 mg/day for HT 25 - 100 mg/day for edema Duration: 6 – 12 hours
: mg/day for HT mg/day for edema Duration: 6 – 12 hours")
50
This drug is a derivative of chlorothiazide that is more popular than the parent drug.

51
It is more potent than chlorothiazide, so the required dose is considerably less.

52
methyclothiazide (Enduron, Aquatensen) 2.5 – 5.0 mg/day for HT 2.5 – 10.0 mg/day for edema Duration: 24 hours
 2.5 – 5.0 mg/day for HT 2.5 – 10.0 mg/day for edema Duration: 24 hours")
53
The thiazide-like diuretics are not the same chemically as the thiazides, but have the same effects.

54
Many have a longer duration of action than the thiazides.

55
chlorthalidone (Hygroton, Thalitone): 15 - 50 mg/day for HT 30 - 120 mg/day for edema Duration: 24 – 72 hours
: mg/day for HT mg/day for edema Duration: 24 – 72 hours")
56
indapamide (Lozol) 1.25 – 5.0 mg/day for HT 2.5 – 5.0 mg/day for edema Duration: up to 36 hours
 1.25 – 5.0 mg/day for HT 2.5 – 5.0 mg/day for edema Duration: up to 36 hours")
57
metolazone (Zaroxolyn) 2.5 – 5.0 mg/day for HT 5.0 – 20 mg/day for edema Duration: 12 - 24 hours (Often used with an organic acid (loop) diuretic in refractory HF due to systolic dysfunction).
 2.5 – 5.0 mg/day for HT 5.0 – 20 mg/day for edema Duration: hours (Often used with an organic acid (loop) diuretic in refractory HF due to systolic dysfunction).")
58
Adverse effects commonly associated with the thiazide diuretics include: hypokalemia hyponatremia in some elderly hypochloremia orthostatic hypotension

59
hyperglycemia Hyperglycemia occurs primarily through the reduction in total body potassium and the subsequent decreased insulin secretion.

60
hyperuricemia Hyperuricemia is associated with the condition gout (crystals of urate/uric acid depositing in tissues of the body).
.")
61
Chronic gout can lead to deposits of hard lumps of uric acid in and around the joints, decreased kidney function, and kidney stones.

62
Thiazide diuretics decrease urate excretion by increasing net urate reabsorption. The mechanism by which this occurs is unclear.

63
2. Organic acid diuretics This class is classified as organic acid diuretics because most of them contain a carboxylic acid functional group.

64
They are more commonly referred to as loop diuretics, as their site of action is the loop of Henle.

65
Organic acid diuretics are indicated for the treatment of edema (pulmonary, peripheral, and edema associated with ascites), HT, and acute renal failure.
, HT, and acute renal failure.")
66
These conditions require a greater diuretic action than is achieved with a thiazide diuretic.

67
They are often used in patients who have developed a resistance to the thiazides.

68
They promote diuresis by inhibiting Na 1+ reabsorption in the loop of Henle.

69
This results in a greatly increased excretion of Na 1+,Cl 1-, and water.

70
They have the greatest Na 1+ excretion, as well as the greatest Ca 2+ excretion (not a desirable effect) of the diuretics.
 of the diuretics.")
71
The organic acid diuretics also result in an increase in K 1+ secretion (they are equivalent to the thiazide diuretics in terms of this).
.")
72
Organic acid diuretics include: bumetanide (Bumex) 0.5 – 10 mg/day Duration: 4 – 6 hours
 0.5 – 10 mg/day Duration: 4 – 6 hours")
73
furosemide (Lasix) 20-80 mg/day initially, may increase by 20- 40 mg Duration: 4 – 6 hours
 mg/day initially, may increase by mg Duration: 4 – 6 hours")
74
torsemide (Demadex) 10-20 mg/day 5 – 10 mg/day for edema associated with cirrhosis (i.e. ascites) Duration: 6 – 8 hours
 Duration: 6 – 8 hours.")
75
The dose may be doubled until desired effect is observed (up to 200 mg, generally in the context of renal failure).
.")
76
ethacrynic acid (Edecrin) 50 – 200 mg/day Duration: 6 – 8 hours
 50 – 200 mg/day Duration: 6 – 8 hours")
77
Adverse effects of the organic acid diuretics: Many of these are similar to the thiazides hypokalemia hyperuricemia hyperglycemia orthostatic hypotension

78
In addition: They produce tone deafness in some patients, especially if given in conjunction with an aminoglycoside antibiotic

79
3. Potassium sparing diuretics This type of diuretic is used when there is a need to maintain normal levels of potassium in the patient along with the diuresis (i.e after MI).
..")
80
Their site of action is the DCT, but farther along the tubule (closer to the collecting ducts) than the thiazides.
 than the thiazides.")
81
They prevent K 1+ secretion in the distal tubules by altering the membrane or blocking aldosterone receptors, so that K 1+ is not secreted in exchange for Na 1+

82
Na 1+ remains in the tubule.

83
When Na 1+ reabsorption is blocked, the body retains more K 1+.

84
Since most of the sodium has already been removed by the time the filtrate reaches the distal tubule, potassium sparing diuretics produce only a mild diuresis.

85
Their primary use is in combination with thiazide or organic acid diuretics to minimize potassium loss.

86
In patients with hepatic cirrhosis, potassium sparing diuretics are recommended along with either a loop or thiazide diuretic.

87
Potassium sparing diuretics are used alone when the patient has an excess of aldosterone (secondary hyperaldosteronism)
")
88
Potassium sparing diuretics include: amiloride (Midamor) 5-10 mg/day Duration: up to 24 hours
 5-10 mg/day Duration: up to 24 hours")
89
spironolactone (Aldactone) 50 – 100 mg/day for treatment of edema, HT 100 – 400 mg/day for treatment of hyperaldosteronism Duration: 48 – 72 hours
 50 – 100 mg/day for treatment of edema, HT 100 – 400 mg/day for treatment of hyperaldosteronism Duration: 48 – 72 hours")
90
eplerenone (Inspra) 25 – 50 mg/day Duration: 12 – 24 hours
 25 – 50 mg/day Duration: 12 – 24 hours")
91
triamterene (Dyrenium) 100 – 200 mg/day Duration: 12 – 16 hours
 100 – 200 mg/day Duration: 12 – 16 hours")
92
Combination diuretics spironolactone with hydrochlorothiazide (Aldactazide) triamterene with hydrochlorothiazide (Dyazide, Maxzide)
 triamterene with hydrochlorothiazide (Dyazide, Maxzide)")
93
These combination diuretics are recommended in patients with diabetes or impaired renal function to prevent hyperkalemia

94
Adverse effects of the potassium sparing diuretics: hyperkalemia nausea, diarrhea

Similar presentations













. Other excretory.>")
 of urine.>")




