Download presentation
Presentation is loading. Please wait.

1
PANNICULITIS Gentleman’s Review Daniel Martingano OMSII

3
PANNICULITIS

4
Definition Panniculitis is a group of heterogenous inflammatory diseases affecting primarily the subcutaneous adipose tissue. These disorders have been classically considered diagnostically challenging, both for dermatologists and pathologists, for several reasons.

5
Septal and Lobular Panniculitis The pathologists classify the panniculitic process as a mostly septal or a mostly lobular panniculitis, and this classification system is very helpful for initial diagnostic purposes. However, this step is just the first one in the diagnostic process, and it should be followed by the search for additional histopathologic findings that allow for a more specific final diagnosis in the language of clinical dermatology.

6
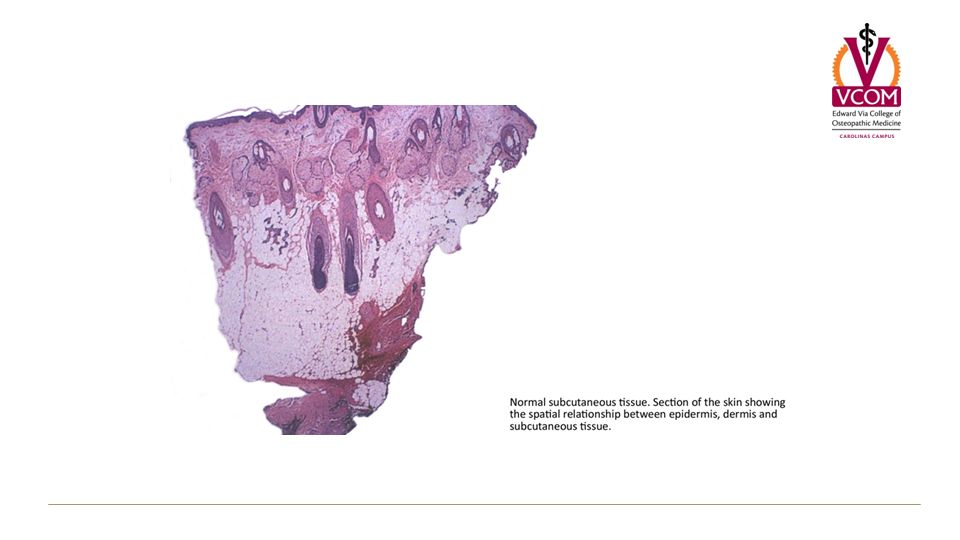
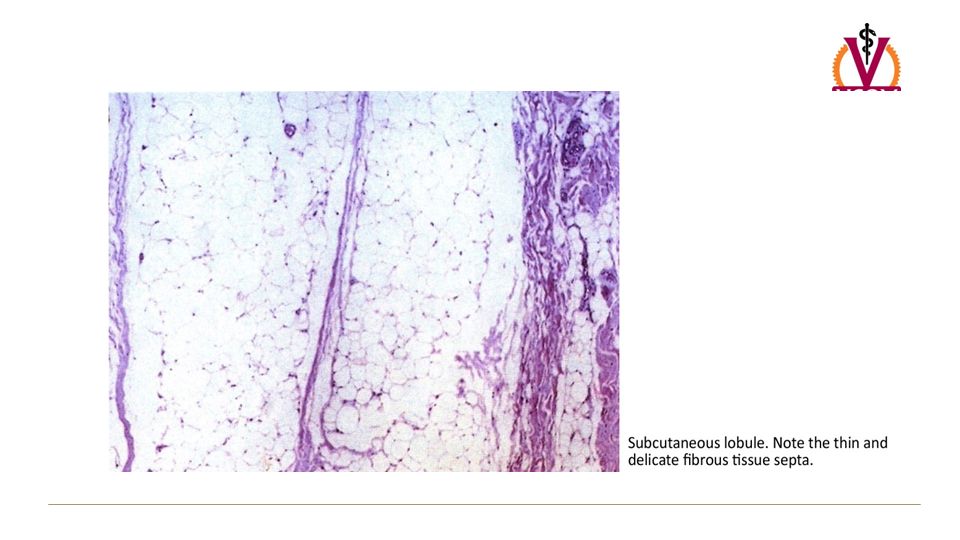
Histology of the Subcutaenous Tissue The basic unit of the subcutaneous tissue is the primary microlobule, which measures approximately 1 mm in diameter and is composed of a microscopic collection of adipocytes. Primary microlobules aggregate to form secondary lobules that measure approximately 1 cm in diameter and are surrounded by thin septa of connective tissue.

9
ERYTHEMA NODOSUM

10
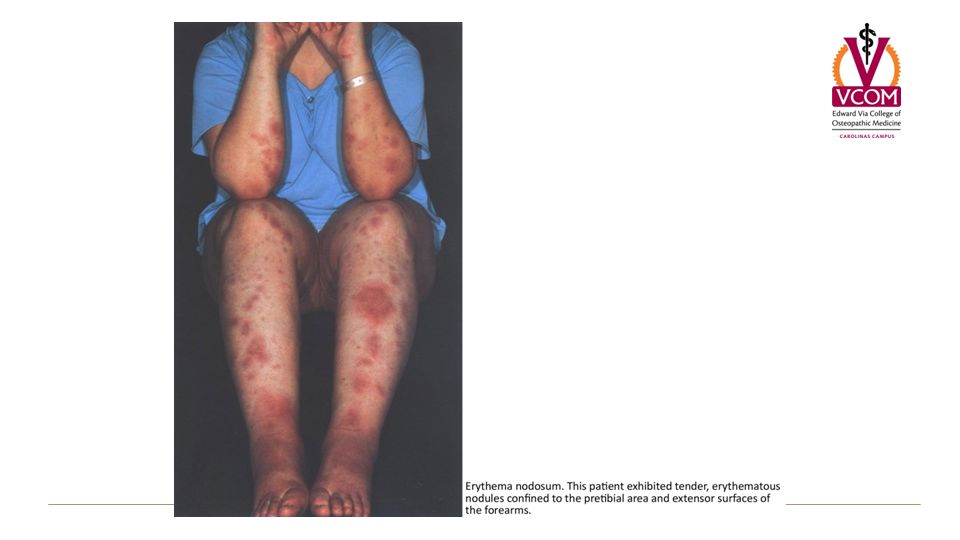
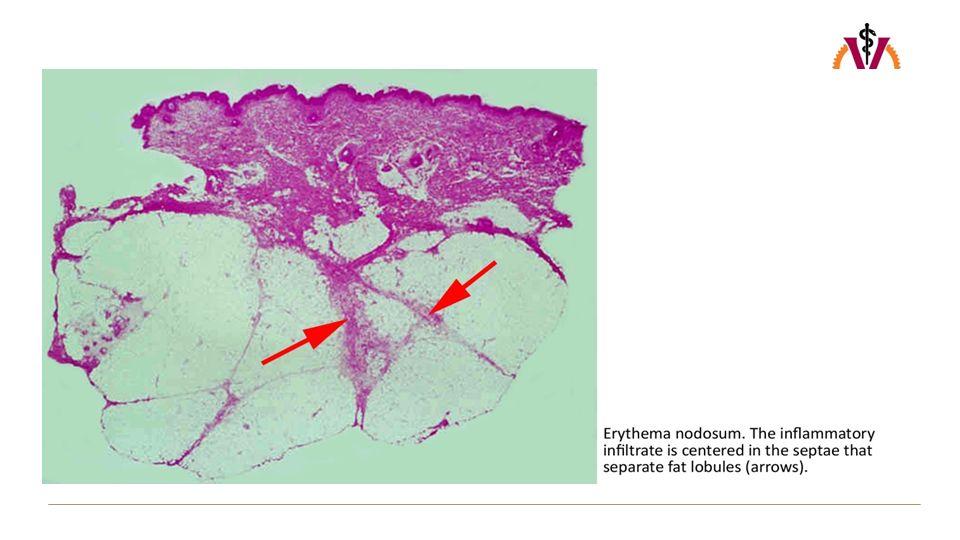
Definition Erythema nodosum is the most frequent clinicopathologic variant of panniculitis and is the paradigm of predominantly septal panniculitis. The disorder usually exhibits an acute onset and is clinically characterized by the sudden eruption of erythematous tender nodules and plaques located predominantly over the extensor aspects of the lower extremities. The lesions show spontaneous regression, without ulceration, scarring, or atrophy, and recurrent episodes are not uncommon.

11
ERYTHEMA NODOSUM Clinical Presentation

12
Erythematous Nodules The typical eruption is quite characteristic and consists of a sudden onset of symmetrical, tender, warm, raised erythematous nodules usually located on the shins, ankles and knees. The nodules, which range from 1 to 5 cm or more in diameter, are usually bilaterally distributed. –Nodules may become confluent resulting in erythematous plaques.

13
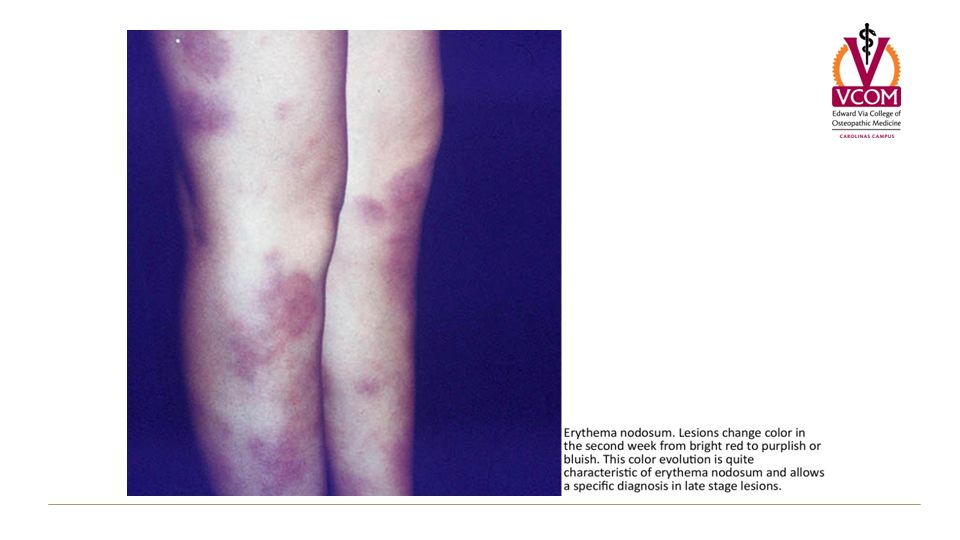
Characteristic Color Evaluation At first, the nodules show a bright red color and are raised slightly above the skin. –Lesions change color in the second week from bright red to bluish or livid. As absorption progresses, the color gradually fades to a yellowish or greenish hue, resembling a bruise. –This color evolution is quite characteristic of erythema nodosum and allows a specific diagnosis in late stage lesions.

14
Healing Ulceration and suppuration are never seen in erythema nodosum and the nodules heal without atrophy or scarring.

15
General Symptoms Usually acute bouts of erythema nodosum are associated with a fever of 38 to 39°C (100-102°F), fatigue, malaise, arthralgia, headache, abdominal pain, vomiting, cough, or diarrhea. Arthralgia occurs in more than 50% of patients and begins during the eruptive phase or precedes the eruption by 2-4 weeks.

16
General Symptoms Erythema, swelling, and tenderness occur over the joint, sometimes with effusions. Any joint may be involved, but the ankles, knees, and wrist are affected most commonly. Synovitis resolves within a few weeks. –No destructive joint changes occur. –Synovial fluid is acellular, and the rheumatoid factor is negative.

19
Laboratory Studies The white blood count is normal or only slightly increased, but the erythrocyte sedimentation rate is often very high, returning to normal when the eruption fades. The rheumatoid factor is usually negative, and there is a temporary increase in the alpha 2 - globulin.

20
Laboratory Studies A high antistreptolysin O titer is seen in those cases of erythema nodosum associated with a sore throat streptococcal infection.

21
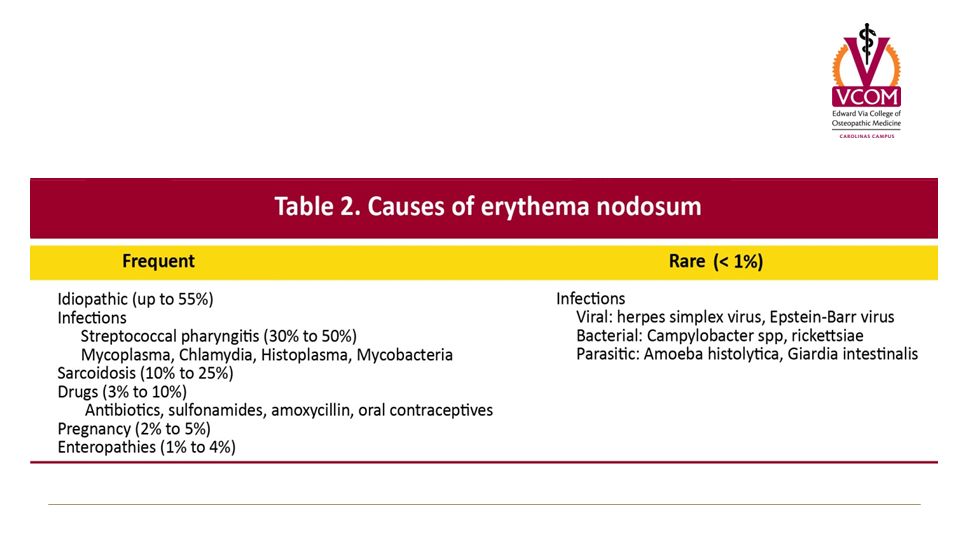
ERYTHEMA NODOSUM Etiology

23
Streptococcal Infections The relationship between a previous episode of upper respiratory tract infection by group A β-hemolytic streptococcus and erythema nodosum is well-known, especially in children and young adults. –Usually, the cutaneous lesions appear 2 or 3 weeks after the throat infection, and they are accompanied by an elevation of the antistreptolysin O (ASO) titer. When the cutaneous nodules develop, the cultures of routine throat swabs usually do not detect microorganisms.
 titer. When the cutaneous nodules develop, the cultures of routine throat swabs usually do not detect microorganisms..")
24
Tuberculosis Tuberculosis is now an uncommon etiologic factor for erythema nodosum. These cases are seen mostly in children, and the cutaneous lesions of erythema nodosum usually indicate a primary pulmonary infection

25
Drugs Sulfonamides and oral contraceptive pills have been long recognized as the most common medications responsible for acute bouts of erythema nodosum, but the list of possibilities is very large. In those cases in which the patient develops erythema nodosum when is taken an antibiotic for an infectious disease is difficult to discern whether the cutaneous reaction is due to the antibiotic or the infectious agent.

26
Sarcoidosis Sarcoidosis constitutes one of the most common etiologic factors in adult patients with secondary erythema nodosum. In northern Europe, erythema nodosum and bilateral hilar adenopathy frequently are seen as early manifestations of sarcoidosis (Löfgren syndrome).
..")
27
Inflammatory Bowel Disease In adults, erythema nodosum associated with enteropathies often correlates with a flare-up of the disease, although the cutaneous eruption may precede the clinical appearance of the inflammatory bowel disease. Ulcerative colitis is more frequently associated with erythema nodosum than Crohn disease

28
Malignancy Erythema nodosum may be a cutaneous marker of malignancy, most often lymphoma or leukemia.

29
Pathogenesis Erythema nodosum is considered to be a type IV, delayed hypersensitivity response to a wide variety of inciting factors. Histopathologic features in fully developed lesions suggest a delayed hypersensitivity mechanism.

30
ERYTHEMA NODOSUM Pathology

31
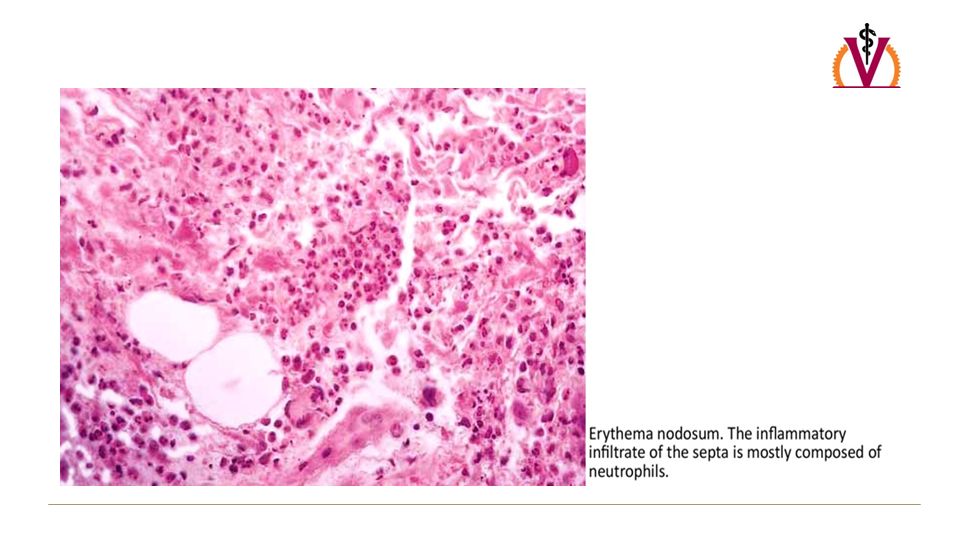
Early Stage Lesions The composition of the inflammatory infiltrate in the septa varies with age of the lesion. In early lesions, edema, hemorrhage, and neutrophils are responsible for the septal thickening. Late stage lesions in the septa are characterized by fibrosis, periseptal granulation tissue, lymphocytes, histiocytes, and multinucleated giant cells.

32
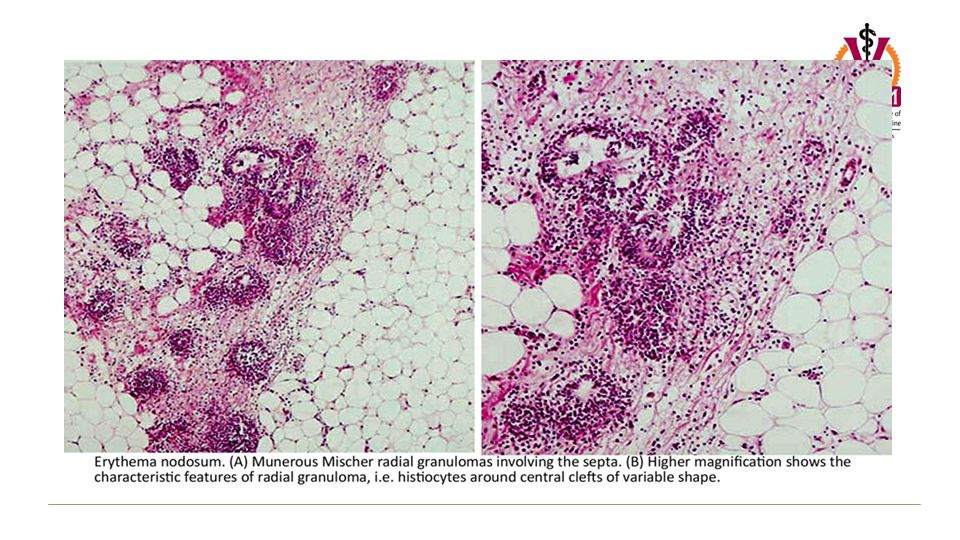
Meischer Radial Granulomas In the early stage of erythema nodosum, two histopathologic lesions are prominent: –septal infiltration with abundant numbers of neutrophils; –Miescher radial granulomas. Miescher radial granulomas are a histopathologic hallmark of erythema nodosum. –They consist of small, well-defined nodular aggregations of small histiocytes around a central stellate or banana shaped cleft.

33
Meischer Radial Granulomas Miescher radial granulomas are present in all stages of the evolution of erythema nodosum lesions. In early lesions, Miescher radial granulomas appear scattered in the septa and surrounded by neutrophils. In older nodules of erythema nodosum, histiocytes coalesce to form multinucleated giant cells.

34
Absence of Vasculitis Another histopathologic characteristic of erythema nodosum is the absence of vasculitis.

38
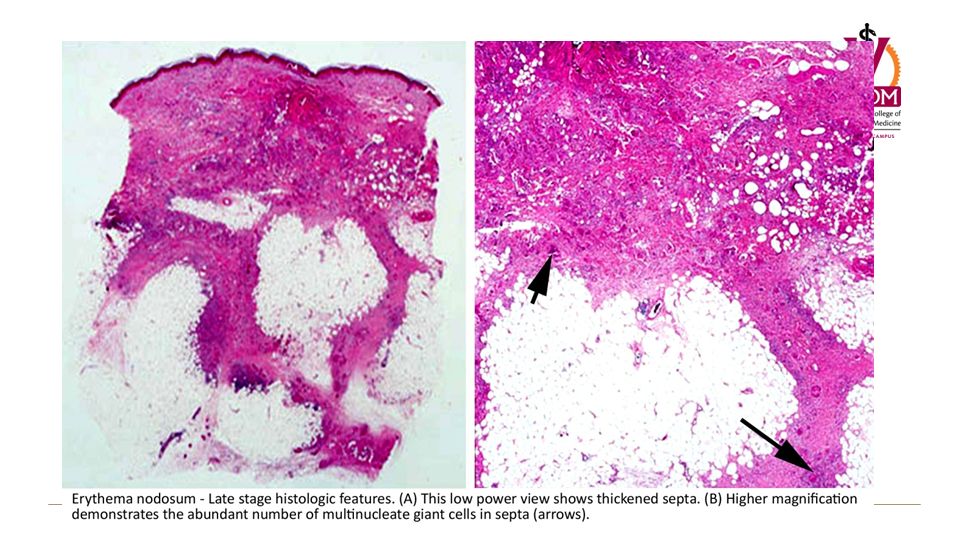
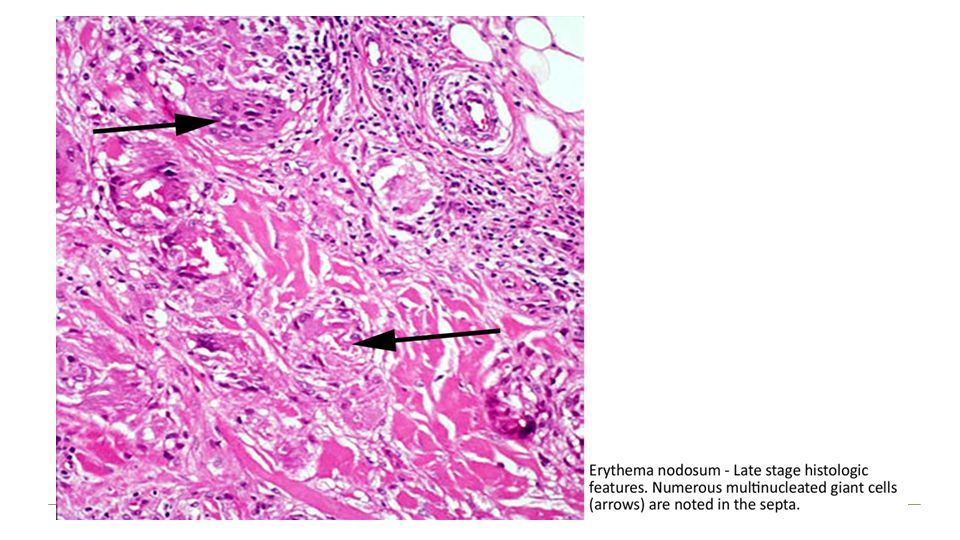
Late Stage Lesions In late stage lesions of erythema nodosum, the inflammatory infiltrate in the septa is sparse, and there are markedly widened septa with granulation tissue at the interface between connective tissue septa and fat lobules. As erythema nodosum evolves, the septa become fibrotic and replaced by granulomas containing multinucleated giant cells.

39
Late Stage Lesions The fat lobules become progressively replaced and effaced by widening septa, which can even completely obliterate the lobules. In these late lesions may be difficult to establish whether the lesion is a mostly septal or mostly lobular panniculitis, because the entire subcutaneous tissue is effaced by a fibrotic and granulomatous process. With time, despite the striking fibrosis, the lesions resolve without atrophy or scarring of the involved septa.

42
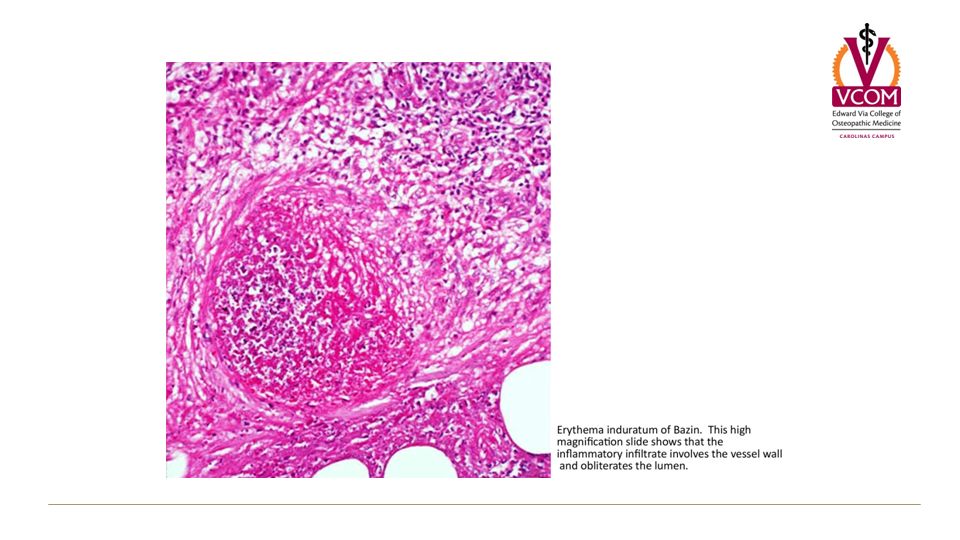
ERYTHEMA INDURATUM

43
Definition Erythema induratum of Bazin (EIB) is a chronic, nodular eruption that usually occurs on the lower legs of young women. Erythema induratum is regarded as a manifestation of type IV delayed hypersentivitity reaction to Mycobacterium tuberculosis.

44
Definition Patients with erythema induratum have a positive tuberculin skin test result and a marked increase in their peripheral T lymphocyte response to purified protein derivative (PPD) of tuberculin, –which causes a delayed-type hypersensitivity reaction against molecular fragments of tuberculosis bacilli.
 of tuberculin, –which causes a delayed-type hypersensitivity reaction against molecular fragments of tuberculosis bacilli.")
45
Clinical Presentation The clinical picture or erythema nodosum differs from erythema induratum of Bazin in showing lesions usually located on the shins that regress in a few weeks with no tendency for necrosis and scarring. In contrast, typical lesions of erythema induratum of Bazin appear on the posterior aspects of the legs of adult women, are more persistent, often ulcerate, and regress leaving an atrophic scar.

46
Clinical Presentation On physical examination, crops of small, tender, erythematous nodules are observed. –These nodules are concentrated on the lower third of the legs, especially around the ankles. Often subcutaneous nodules become adherent to the skin surface and ulcerate. Healing of these ulcers is usually a slow process, resulting in atrophic scars.

47
Clinical Presentation The course is protracted and recurrent episodes over years, even decades, are common. Individual lesions tend to involute, but new crops appear at irregular intervals. Patients with erythema induratum of Bazin are otherwise in good health.

48
Laboratory Studies Peripheral blood cell count and complete metabolic panel are normal. Erythrocyte sedimentation rate is elevated.

49
ERYTHEMA INDURATUM Pathology

50
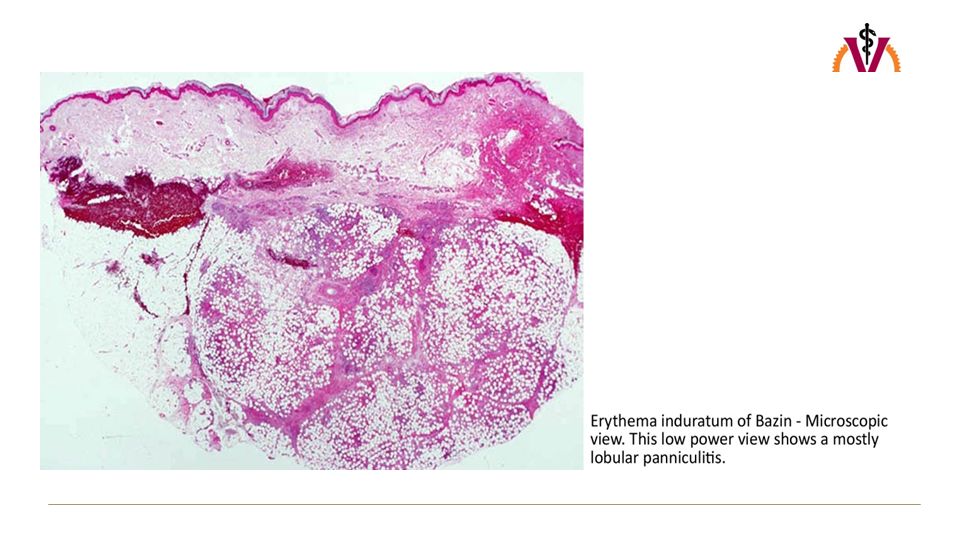
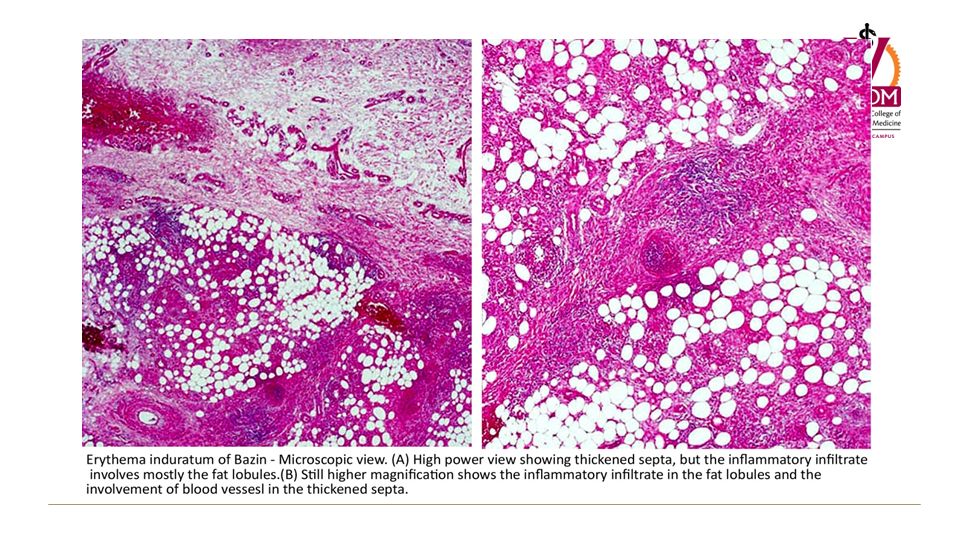
Erythema Induratum of Bazin In contrast to erythema nodosum, which is mainly septal panniculitis, erythema induratum initially is mainly a lobular panniculitis due to vasculitis that produces ischemic necrosis of the fat lobule with relatively less involvement of the structures of the septa.

52
Vasculitis The presence of vasculitis in the biopsy specimen is not always identified and is not considered a requisite for making the diagnosis. At the septae, a vasculitis of small and middle size vessels can be seen, sometimes affecting the muscular arteries with fibrinoid necrosis and hemorrhage.

53
Topography of Vascular Necrosis Vascular architecture of subcutaneous tissue explains the intralobular localization of necrosis. Each individual secondary lobule is supplied by a small muscular artery branching from the septa to form arterioles that supply every individual primary microlobule. The arterioles branch to form capillaries into the microlobule and a capillary network surrounds each individual adipocyte.

54
Topography of Vascular Necrosis Postcapillary venules meet in veins, which also run along the septa. In each microlobule, the arteriole occupies a central position, whereas the venule runs along the periphery. As a consequence, interference with the arterial supply results in diffuse necrosis within the fat lobule (lobular panniculitis).
..")
56
Lobular Histopathologic Changes At an early stage, the fat lobules are punctuated throughout by discrete collections of inflammatory cells, mostly neutrophils. There may be extensive necrosis of the adipocytes of the fat lobule (fat necrosis). –These necrotic adipocytes call for histiocytes that ingest lipid and become foamy.
. –These necrotic adipocytes call for histiocytes that ingest lipid and become foamy..")
57
Lobular Histopathologic Changes Later a second type of necrosis, caseous necrosis, develops. Epithelioid cells, multinucleated giant cells, and lymphocytes contribute to the granulomatous appearance of the inflammatory infiltrate in fully developed lesions of erythema induratum of Bazin. When intense vascular damage is present, extensive areas of caseous necrosis become extensive. Caseous necrosis may extend to the overlying dermis and secondarily involve the epidermis with ulceration and discharge of liquefied necrotic fat.

58
Ziehl-Neelsen Stain Ziehl-Neelsen stain (which is used to visualize acid- fast bacilli) does not reveal intact mycobacteria. In one third of cases granulomas are absent and lymphocytes and plasma cells predominate. Both the tuberculoid granulomas and lymphoid infiltrate extend between the fat cells, largely replacing them.

Similar presentations









, and the parenchyma.>")
 Definition: Rheumatic fever (RF) is an autoimmune disease affecting the heart and extra- cardiac.>")


, calor (heat), tumor (swelling), dolor (pain), and loss of function.>")






