Download presentation
Presentation is loading. Please wait.

1
By: Haya M. Al-Malaq Clinical pharmacy department KSU
TB By: Haya M. Al-Malaq Clinical pharmacy department KSU

2
Introduction TB is the leading global infectious killer with 2.9 million deaths annualy.

3
Characteristics of the organism
M. tuberclusis is an acid fast bacillus b/c of its resistance to decolonization by acid alcohol after staining with basic function. It thrives in environments with high O2 tension. (e.g. epics of the lung)
")
4
Risk factors Immunosuppressant. Poor nutrition. DM.
Crowded living conditions. Various chronic diseases.

5
Pathophysiology The inflammation produced with TB infection is granulomatous, with epithelioid macrophages and Langhans giant cells along with lymphocytes, plasma cells, maybe a few PMN's, fibroblasts with collagen, and characteristic caseous necrosis in the center. The inflammatory response is mediated by a type IV hypersensitivity reaction.

6
Diagnosis Subjective findings Objective findings
Potential misdiagnoses

7
Subjective Findings Productive cough Fatigue Night sweats Fever
Pleuritic pain General malasie Dyspnea

8
Objective findings Chest radiograph( lower RTI, nodular infiltrates)
Positive sputum smear for AFB Positive PPD skin test (14mm) Hematologic manifestation (leukocytosis,Anemia)
 Hematologic manifestation (leukocytosis,Anemia)")
10
PPD skin test Chapter 61 page 4

11
Tuberculin PPD skin test Mantoux method
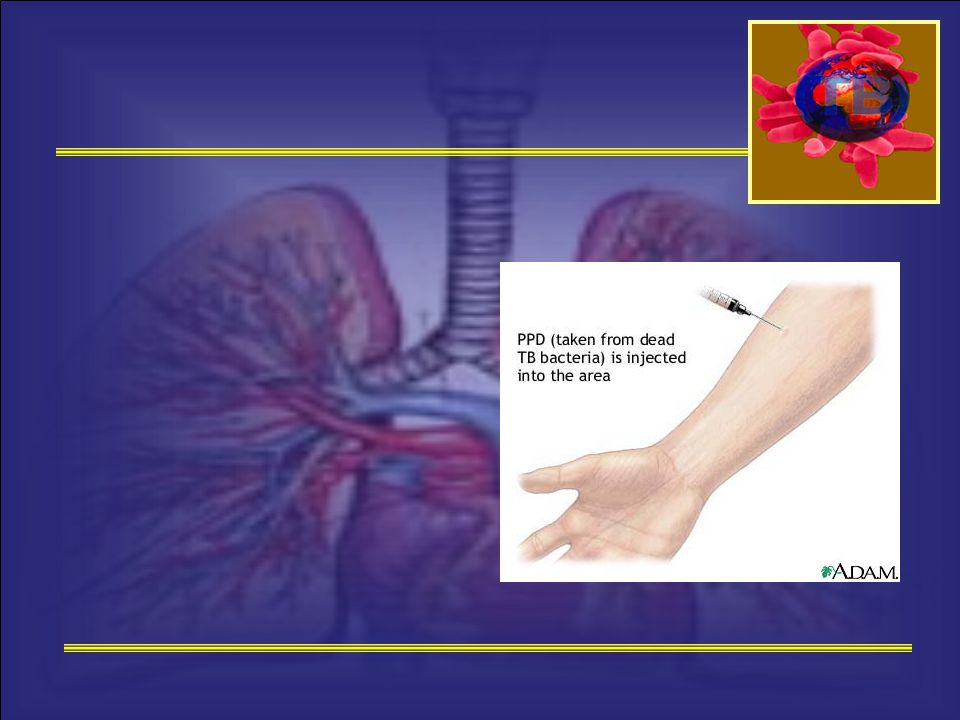
Diagnostic tool used to detect infection with M.tuberculosis but not active TB. PPD refers to Purified Protein Derivative of M.tuberculosis, which is prepared from a culture of tubercle bacilli. The solution available: 1 TU per0.1ml 5 TU Per 0.1ml 250 TU Per 0.1ml

14
PPD skin test method Injecting 0.1ml of 5TU PPD intradermaly into volar or dorsal surface of the forearm. If the patient previously infected with M.tuberculosis,sensitized T cells are recruited to the skin site T cells cytokines induration (raised area)
")
15
Tuberculin PPD skin test
Induration is local vasodilatation, edema,fibrin deposition, and recruitment of other inflammatory cells to the area. The reaction to tuberculin begins 5-6hr. Max induration observed 48-72hr. The diameter of the induration should be measured in millimeters.

17
Tuberculin PPD skin test
Induration≥5mm consider to be a positive reaction: Recent history of close contact Fibrotic changes on chest radiograph consistent with old TB Organ transplant patients Immunosuppressed patients HIV positive persons

18
Tuberculin PPD skin test
Induration size of 10mm is used as the cut point for +vety in clinical condition that inc risk of TB: DM Silicosis CRF Leukemia Lymphoma Gastrectomy Wt loss of >10% of ideal body wt.

19
Tuberculin PPD skin test
Induration ≥10mm is considered to be +ve: Countries with high prevalence of TB Drugs users Employees of high-risk congregate settings Mycobacteriology laboratory personnel Children <4 years of age

20
Tuberculin PPD skin test
False-positive tuberculin skin test: Infection secondary to other mycobacterial species BCG vaccine Impurities in the solutions False-negative tuberculin skin test: Bacterial, viral,fungal Vaccination CRF Disease of lymphoid organ Age Drugs

21
Tuberculin PPD skin test
False-negative tuberculin skin test occur 25% Anergy decresed ability to respond to antigens due to sever debility, old age,immaturity in newborns,live vaccinations

22
Tuberculin PPD skin test
Positive PPD skin test DOSE NOT confirm diagnosis of active TB. Other test to confirm TB: Sputum culture(AFB) Gastric aspiration Spinal fluid Urineanalysis Tissue biopsy
 Gastric aspiration. Spinal fluid. Urineanalysis. Tissue biopsy.")
23
AFB Limmitation of AFB: Negative AFB dose not rule out active TB
AFB dose not has the ability to differentiate between mycobacterial species & viable-nonviable bacteria.

24
Case 1 Chapter 61 page 3

25
Case M.W 36 yo f CC: 2m history of cough recently became productive, she also is experiencing fatige, night sweats, wt loss 10Ib. Other medical problem DM (10u NPH daily, poor nutritional status 2ry to frequent dieting. She works as a volunteer in a nursing home several days a wk.

26
Case Recently it has been discovered that 2 pt that she has been caring for had active TB. PE: N, CXR reviled bibasilar infiltrates. PPD, AFB, CLT of sputum was ordered. Initial labs were WNL. PPD was 14mm ein 48hrs, sputum smear was +ve for AFB, MTB culture was ordered to confirm the diagnosis.

27
Questions What S&O findings dose M.W have that r consistent with TB?
What is PPD skin test? How should results be interperted in M.W? b/c M.W PPD skin test is +ve, does this confirm the diagnosis of active TB?

28
Questions Should M.W be tested for HIV?
Would a –ve PPD skin test eliminate the possibility of infection in M.W?

29
Case 6 Chapter 61 page 6

30
Booster Phenomenon S.N 50 yo hospital employee receiving his initial PPD skin test (PPD-mantoux), & had a 7 mm induration. b/c of his age & previous hospital employment, it was decided to retest him 1 wk later to rule out “booster” effect. the results of the repeated test was 12 mm, he denied any exposure to a person with TB.

31
What is the significance of this reaction?
Should S.N be placed on INH therapy for latent TB infection?

32
Definition Some people experience increase in size of a TB skin test not caused by TB infection.

33
Possible Causes TB skin test it self if preformed every 1-2 yrs.
Infection with other mycobacteria. Remote TB. Prior BCG vaccination. The incidence of the rx increase with age & may appear 1 wk after the previous test.

34
How to know 2 step skin test is for new employee only.
If the repeated test is +ve (>10 mm)--- booster phenomena. If change to +ve but <10 mm (6 mm inc) after 1 yr---recent converter.
--- booster phenomena. If change to +ve but <10 mm (6 mm inc) after 1 yr---recent converter.")
35
Case 7 Chapter 61 page 6-7

36
BCG Vaccine C.T is a 25 yo F refugee from Combodia, was given a routine PE upon entering this country. As a part of this examination, she received a tuberculin skin test with 5TU PPD. The test results were +ve with 12mm induration. She denies receiving TB tx but remembered receiving BCG vaccine several yrs agp

37
What is BCG vaccine? Does this +ve skin test indicate infection with MTB?

38
Case 29 Chapter 61 page 22

39
Case E.F, 25 yo f, treated with: INH (15 mg/kg)
Rifampin 600 mg twice a wk. For uncomplicated TB, thinks she is pregnant

40
Risk / Teratogenicity Should therapeutic abortion be considered?
What are the risks of TB & its treatment on the mother & fetus? Are these drugs teratogenic?

41
Risk / Teratogenicity Untreated TB is greater risk than treatment.
INH, Rif, Eth are teratogenic in animals not in humans. They are safe to use in normal dose in pregnancy.

42
Risk / Teratogenicity Pyrazinamide has been used safely but its teratogenic potential has not been studied adequately for FDA approval, it is only reserved for resistant cases. All pregnant women receiving INH should receive pyridoxine 25 mg/d b/c of the possibility of CNS toxicity.

43
Risk / Teratogenicity There is some risk of limb malformation & hypoprothrombinemia but not stat sig. Streptomycin should not be used (except as a last alternative) b/c of risk of ototoxicity. Therapeutic abortion is not recommended. INH, rif, eth safely used for 9 m.
 b/c of risk of ototoxicity. Therapeutic abortion is not recommended. INH, rif, eth safely used for 9 m.")
44
Lactation E.F may breast-feed while taking her medn.

45
Case 30 Chapter 61 page 22-23

46
Pediatrics A.M is a 3 yo African American boy, is suspected of having TB. His father has been receiving tx for TB for the last 2 m. He has productive cough, fever, & general malaise. His sputum is +ve for AFB, & +ve PPD skin test (10 mm).
.")
47
Pediatrics What is the incidence of TB in children?
How should A.M. be treated?

48
Pediatrics Incidence dec 3/100000 in 1993 to 1.5/100000 in 2001.
b/c of risk of disseminated TB pt should be tx asap (directly after diagnosis). The same regimen as for adults except for Eth (difficulty in assessing visual acuity).
. The same regimen as for adults except for Eth (difficulty in assessing visual acuity).")
49
Pediatrics 3 drug combination is recommended b/c of lo bacillary population & difficulty for an infant to take 4 drug. Regamin is INH (10-15mg/kg/d)+ Rif (10-20mg/kg/d)+ Pyrz (15-30mg/kg/d) for 8 wks then INH+Rif daily or 2-3t/wk for 4m (no resistance).
+ Rif (10-20mg/kg/d)+ Pyrz (15-30mg/kg/d) for 8 wks then INH+Rif daily or 2-3t/wk for 4m (no resistance).")
50
Pediatrics If resistance is suspected add Eth (15-20mg/kg/d) until susceptibility is confirmed. Examine routinely for hepatitis, occurs within 3 months of therapy and more associated with hi dose & combination therapy.

51
High-Priority Candidates for Treatment of Latent Tuberculosis Infection
Treatment Should be recommended for the following persons with a positive tuberculin skin test, regardless of age:. Persons with known or suspected HIV infection. Close contacts with infectious TB. Recent tuberculin skin test converters. DM, corticosteroids and immunosuppressive therapy, ESRD injection drug users, rapid weight loss.

52
High-Priority Candidates for Treatment of Latent Tuberculosis Infection
Treatment Should be recommended for the following persons with a positive tuberculin skin test who are < 35 years of age and do not have additional risk factors:. Foreign-born persons from high-prevalence countries. Medically underserved low-income populations. Resident of facilities for long term care.

53
Thank You

Similar presentations













 PHCL 442 Lab Discussion Jamilah Al-Saidan, M.Sc.>")




 Gram (+) rod (bacilli). Acid-fast Pulmonary.>")
Caused by Mycobacterium.>")

 is caused by a bacterium called Mycobacterium tuberculosis that is.>")
