Download presentation
Presentation is loading. Please wait.

1
Thymoglobulin: An Overview of Its Performance in Clinical Trials as an Agent for the Induction Therapy Reference: Osama Gaber A, Knight RJ, Patel S, et al. A review of the evidence for use of thymoglobulin induction in renal transplantation. Transplant Proc. 2010;42:1395– 1400.

2
Introduction Prevention of early acute rejection in posttransplantation period can be achieved through the use of biological agents/monoclonals that deplete T or B cells or regularize the cellular/antibody response. This therapy is termed as an induction therapy. Presently, monoclonal antibody (IL2RA) blockers and lymphocyte-depleting antibodies are used in the induction therapy in kidney transplantation. Depleting antibodies such as thymoglobulin-activated cytokines, which are attributed with an increased chance of postinfusion reaction. Rabbit antihuman thymocyte globulin (rATG; thymoglobulin) is the most commonly used agent in the induction therapy, but has yet to be approved by the Food and Drug Administration (FDA). The delay in the approval has become a barrier in the assessment of rATG in large scale clinical induction trials, and its clinical performance as an induction therapy agent through registry data, a single-center trial and randomized trials. Osama Gaber et al. in a recent review compiled the various evidences of rATG for its use as an induction agent in renal transplantation.
 blockers and lymphocyte-depleting antibodies are used in the induction therapy in kidney transplantation. Depleting antibodies such as thymoglobulin-activated cytokines, which are attributed with an increased chance of postinfusion reaction. Rabbit antihuman thymocyte globulin (rATG; thymoglobulin) is the most commonly used agent in the induction therapy, but has yet to be approved by the Food and Drug Administration (FDA). The delay in the approval has become a barrier in the assessment of rATG in large scale clinical induction trials, and its clinical performance as an induction therapy agent through registry data, a single-center trial and randomized trials. Osama Gaber et al. in a recent review compiled the various evidences of rATG for its use as an induction agent in renal transplantation..")
3
Registry Analysis rATG vs. IL2RA vs. No Antibody Induction The safety and the effi cacy results of rATG obtained from the registry analysis have so far been promising. Results have been encouraging particularly in the high immunological risk and Afro-American renal transplant recipients. One of the analyses carried out by Willoughby et al., report rATG with signifi cant reduction in the incidence of triple end point, graft loss and patient death compared to tacrolimus and mycophenolate mofetil (MMF). The authors conclude that from studies carried out so far, rATG is as safe as IL2RA and provides better outcomes in high immunological risk patients and in a steroid- minimization regimen.
. The authors conclude that from studies carried out so far, rATG is as safe as IL2RA and provides better outcomes in high immunological risk patients and in a steroid- minimization regimen..")
4
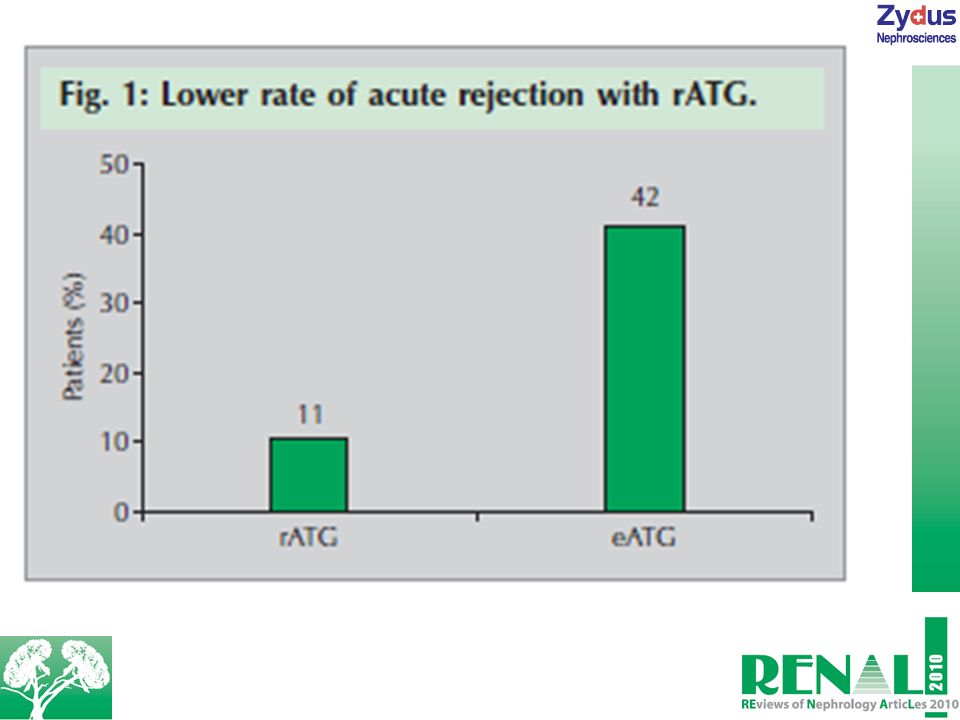
Performance of rATG in Randomized, Controlled Clinical Trials Effi cacy of rATG over eATG in Renal Transplant Recipients Comparison of rATG and equine antithymocyte globulin (eATG) in relation to safety and effi cacy was initially carried out in living adults and deceased donor kidney recipients in a study. Patients were randomized to receive rATG or eATG, which was administered intraoperatively and then up to 6 days. Cyclosporine (CysA), azathioprine/ MMF and prednisolone were administered as maintenance immunosuppressants to patients. – At 1 year, there was no difference in the groups in terms of survival rates (rATG-98%; eATG-96%). However, rATG treatment was associated signifi cantly with lesser episodes of acute rejections (4.2 vs. 25%). – Higher proportions of incident-free survival were observed with rATG treatment compared to eATG at the end of 5-year posttransplantation. – The actual advantages of rATG were observed at the 10- year posttransplantation follow-up. Compared to eATG, rATG was associated with higher event-free survival (48 vs. 29%) and lower 10-year cumulative acute rejection (11 vs. 42%; see Fig. 1). – Rabbit antihuman thymocyte globulin was associated with no posttransplant lymphoproliferative disorder.
, azathioprine/ MMF and prednisolone were administered as maintenance immunosuppressants to patients. – At 1 year, there was no difference in the groups in terms of survival rates (rATG-98%; eATG-96%). However, rATG treatment was associated signifi cantly with lesser episodes of acute rejections (4.2 vs. 25%). – Higher proportions of incident-free survival were observed with rATG treatment compared to eATG at the end of 5-year posttransplantation. – The actual advantages of rATG were observed at the 10- year posttransplantation follow-up. Compared to eATG, rATG was associated with higher event-free survival (48 vs. 29%) and lower 10-year cumulative acute rejection (11 vs. 42%; see Fig. 1). – Rabbit antihuman thymocyte globulin was associated with no posttransplant lymphoproliferative disorder..")
5
Effi cacy of rATG over Basiliximab and Daclizumab in High- Risk Renal Transplant Recipients The safety and effi cacy of rATG was compared against basiliximab in a multicentered, international study in deceased donor kidney transplant recipients at a risk of acute rejection episodes or delayed graft function (DGF). Patients were randomized to receive either rATG or basiliximab. At the end of the study, – At 1 year follow-up, comparisons of various parameters were; biopsy-proven acute rejection (BPAR) (15.6 vs. 25.5%), graft survival (90.8 vs. 89.8%) and patient survival (95.7 vs. 95.6%). – At 5-year follow-up, rATG was associated with lower incidences of a composite endpoint of BPAR, graft loss and death compared to basiliximab (37 vs. 51%), incidences of BPAR was also found to be signifi cantly less with rATG (15 vs. 27%).
 (15.6 vs. 25.5%), graft survival (90.8 vs. 89.8%) and patient survival (95.7 vs. 95.6%). – At 5-year follow-up, rATG was associated with lower incidences of a composite endpoint of BPAR, graft loss and death compared to basiliximab (37 vs. 51%), incidences of BPAR was also found to be signifi cantly less with rATG (15 vs. 27%)..")
7
Another study, which was a multicenter investigatorsponsored study, compared the safety and the effi cacy of rATG against daclizumab in high immunological risk renal transplant patients. Patients were randomized to receive either rATG or daclizumab. The maintenance immunosuppressants included tacrolimus, MMF and steroids. In the rATG group, tacrolimus was delayed up to day 5. – The rATG treatment was found to be equally effective in terms of overall graft survival (82.3 vs. 89.5%) and patient survival (95.6 vs. 96.5%). – The rATG showed a higher bacterial incidence (18.6 vs. 10.5%).
 and patient survival (95.6 vs. 96.5%). – The rATG showed a higher bacterial incidence (18.6 vs. 10.5%)..")
10
The overall outcomes of the study favored rATG, which was suggested to be better than daclizumab in high immunity risk kidney transplant recipients through BPAR. Rabbit antihuman thymocyte globulin also fi nds a mention in the Kidney Disease Quality Outcomes Initiative (KDQOI) clinical guidelines for the care of transplant recipients. They recommend its use in adult kidney recipients who are at risk for acute rejection episodes. The guidelines also suggest that leukocyte-depleting antibodies provide beneficial effects.
 clinical guidelines for the care of transplant recipients. They recommend its use in adult kidney recipients who are at risk for acute rejection episodes. The guidelines also suggest that leukocyte-depleting antibodies provide beneficial effects..")
11
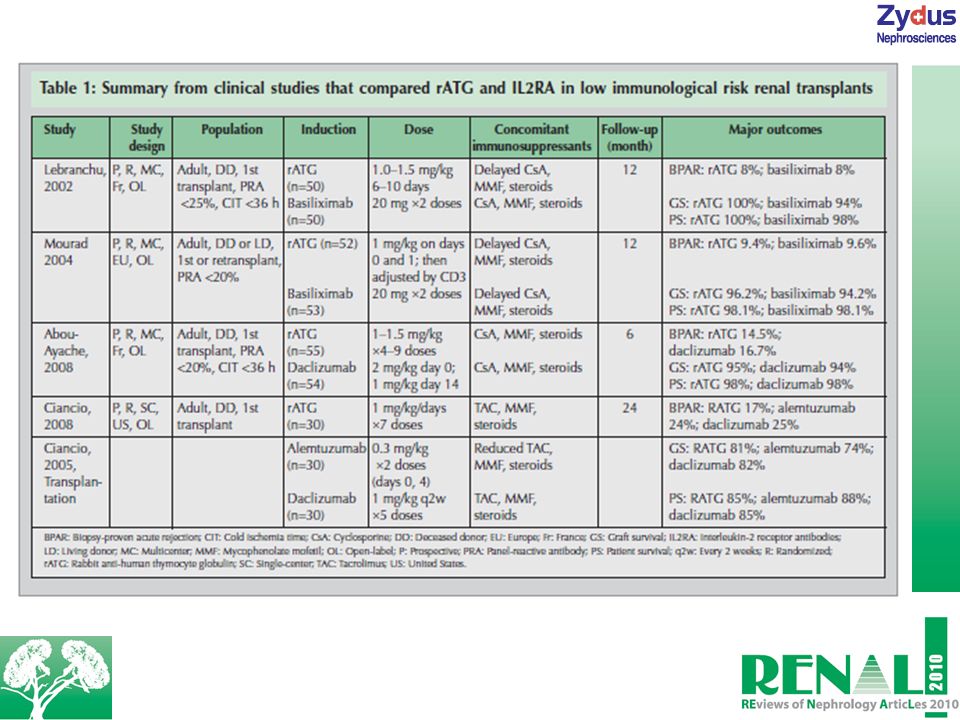
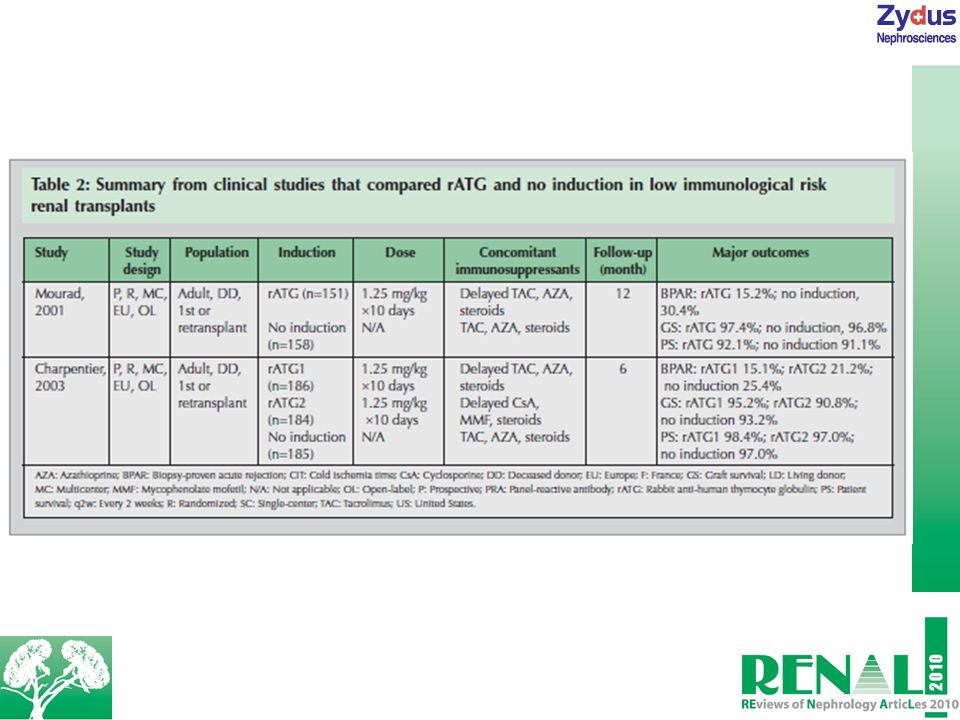
rATG vs. IL2RA in Low Immunological Risk Patients Investigations carried out so far with rATG in low immunological risk patients are summarized in Table 1. Four studies compared rATG with IL2RA, in which they were found to be equally effective in preventing BPAR in low immunological risk, primary kidney transplant patients. Thymoglobulin vs. No Induction Therapy An induction therapy containing rATG has been compared against tacrolimus vs. CysA maintenance therapy in two prospective, multicenter European studies (see Table 2). The rATG treatment has been observed with delayed initiation of tacrolimus administration. The rATG group was associated with a low rate of BPAR (15.2 vs. 30.4%). When compared to no antibody induction, rATG had lower incidences of acute rejection episodes and delayed the introduction of a calcineurin inhibitor. This is anticipated to be advantageous in patients with a risk of DGF or other adverse clinical conditions.
. The rATG treatment has been observed with delayed initiation of tacrolimus administration. The rATG group was associated with a low rate of BPAR (15.2 vs. 30.4%). When compared to no antibody induction, rATG had lower incidences of acute rejection episodes and delayed the introduction of a calcineurin inhibitor. This is anticipated to be advantageous in patients with a risk of DGF or other adverse clinical conditions..")
12
Summary The induction antibody therapy is used to reduce the incidence of early acute rejection episodes and minimize the use of immunosuppressants in early posttransplantation stage. This helps in the recovery of renal function before the use of calcineurin inhibitor-based immunosuppression. Despite not being approved by the FDA as an induction therapy, rATG therapy is evidenced to reduce incidences of acute rejection episodes after kidney transplantation in high-risk patients when compared against no antibody induction or interleukin-2 receptor blockers. Benefi ts of rATG treatment have given it a place in the KDQOI clinical guidelines. The advantage of delayed use of calcineurin inhibitors have also been evidenced in different clinical studies. However, its reactions such as cytokine activation, hematological abnormalities and increased risk of viral infections have rendered it to be used with caution against low immunological risk patients.

Similar presentations









: 1045-1095.>")





 Transplantation Kidney Transplant Inserting a kidney of another live or dead person into a person. The donor kidney is typically placed.>")

 in Patients with Secondary Myelodysplastic Syndromes (sMDS) Enrolled in the AVIDA Registry 1 Prospective Trial.>")
 in the Consolidation Treatment of Newly Diagnosed APL — First Interim Analysis of a Randomized Trial (APL 2006) by the French Belgian.>")
