Download presentation
Presentation is loading. Please wait.

1
Paediatric Urodynamics Divyesh Desai Paediatric Urologist Director, Paediatric Urodynamics Unit Great Ormond Street Hospital for Children NHS Trust

2
Urodynamics: Aims Reproduce patients complaints / symptoms Contribute a pathophysiological explanation for the problem

3
Paediatric Urodynamics: Aims Define the pressure / volume relationships within a pathological system o Is the bladder safe? o Are there any abnormal dynamics ….. likely to contribute to bladder / renal function deterioration? that can be treated to reduce morbidity?

4
Paediatric Urodynamics Specialist Aims To understand the evolving natural history of lower tract function in specific pathological conditions o e.g. PUV, VUR, Neurogenic Bladders, Bladder Exstrophy o Can we improve our management?

5
Poor understanding - inappropriate management of lower urinary tract function can lead to: o impaired renal function o unnecessary morbidity handicap a child for life Think: Urodynamic Function

6
Urinary Control 2 nd Year of Life – learns to ‘HOLD’ 2 – 4 Years of Age – Voluntary Control 4 – 5 Years of Age – Void on Demand with a partially full bladder 6 – 7 Years of Age – Complete Bladder Control (94 – 95%)
")
7
Prevalence By Age 7 Years Isolated Daytime Incontinence – 1 – 6 % Female : Male 3 : 1 Isolated Nocturnal Incontinence – 3 – 20% Nocturnal Incontinence > 15 yrs age – 1 – 3% Male > > > Female Day and Night Incontinence – 10 – 12% Male = Female

8
What is the purpose of Urodynamics? Understand bladder function Explain symptoms Direct treatment

9
Urodynamics Investigation Measurement of function or dysfunction of the urinary tract by any appropriate means Simple urodynamics Invasive urodynamics

10
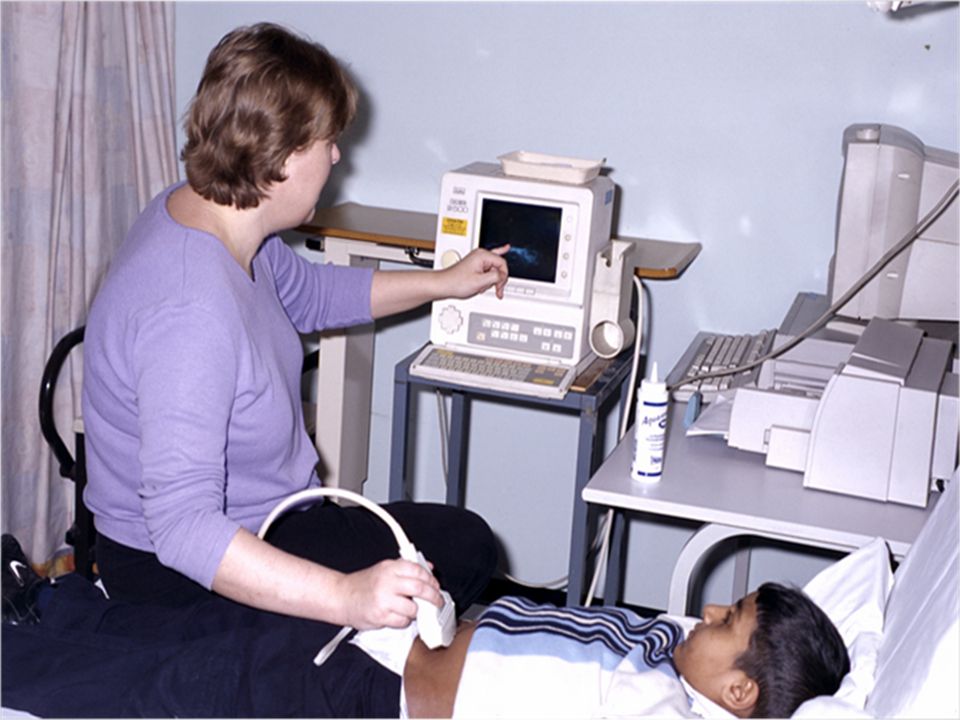
Non Invasive Assessment

11
Non invasive assessment Serves as a baseline assessment Assist in ongoing follow ups Directs treatment/ treatment modification Assists in selection of patients requiring further invasive studies

12
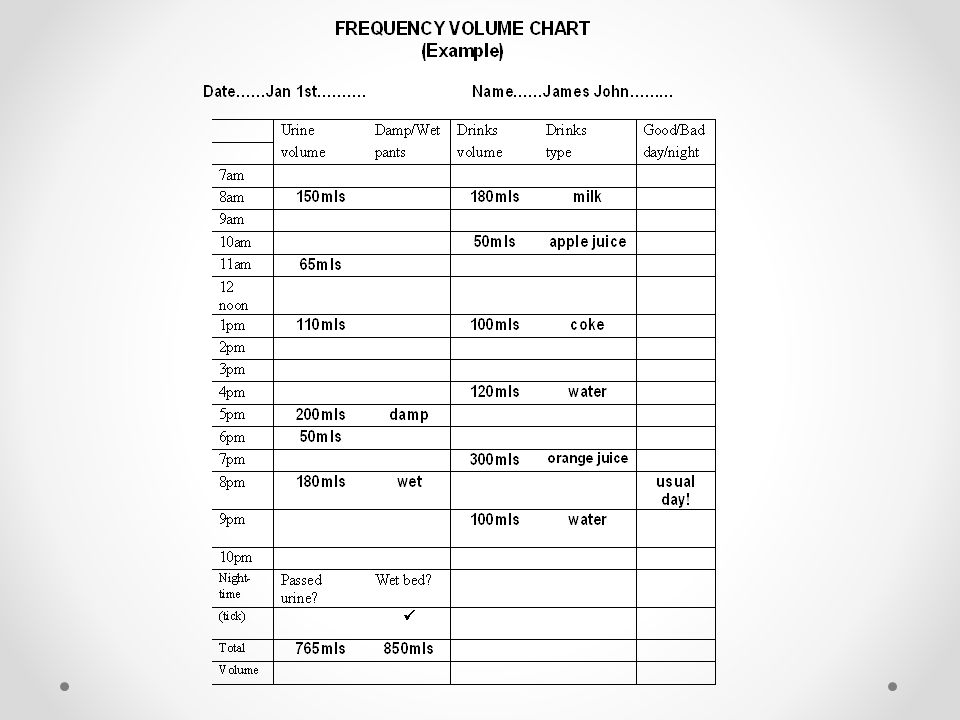
Tools of investigation History taking – parents/child Physical examination Bladder diary Voiding observation Other relevant information e.g. imaging

13
Urinary Incontinence Continuous v/s Intermittent Daytime / Night / Both Organic / Functional Neurogenic / Non-Neurogenic

14
PUV Intermittent Enuresis Day / Night + / - Poor urinary stream + / - Straining Polyuria Non-Neurogenic

15
Vaginal Ectopic Ureter Continuous urinary incontinence With normal voiding in-between

16
Vaginal Reflux Post void incontinence Intermittent

17
Female Epispadias Continuous urinary incontinence

18
Spinal Dysraphism Lipoma Hemangioma

20
Expected bladder capacity Under 2 years: - 7.0 x weight Kg (Koff 1983) e.g. 10Kg x 7 = 70mls Over 2 years: - 30 +(age in years x 30) (Hjalmas 1988) e.g. 30 + (5 x 30) = 180mls
 (Hjalmas 1988) e.g (5 x 30) = 180mls.")
21
Bell shaped curve

22
Tower shaped curve

23
Interrupted flow

24
Staccato Flow

25
Plateau Flow

27
Average flow rates Age 4 – 7 years: - ( ♂ and ♀) - 10mls/sec Age 8 – 13: - ♂ = 12ml/sec ♀ = 15ml/sec Age 14 – adult: - ♂ = 21mls/sec ♀ = 18mls/sec
 - 10mls/sec Age 8 – 13: - ♂ = 12ml/sec ♀ = 15ml/sec Age 14 – adult: - ♂ = 21mls/sec ♀ = 18mls/sec")
28
Invasive Urodynamics Natural fill urodynamics (NFU) Standard artificial filling CMG Video contrast filling CMG Isotope filling CMG - (QIC) Natural fill + direct isotope CMG (NFIDC)
 Standard artificial filling CMG Video contrast filling CMG Isotope filling CMG - (QIC) Natural fill + direct isotope CMG (NFIDC)")
29
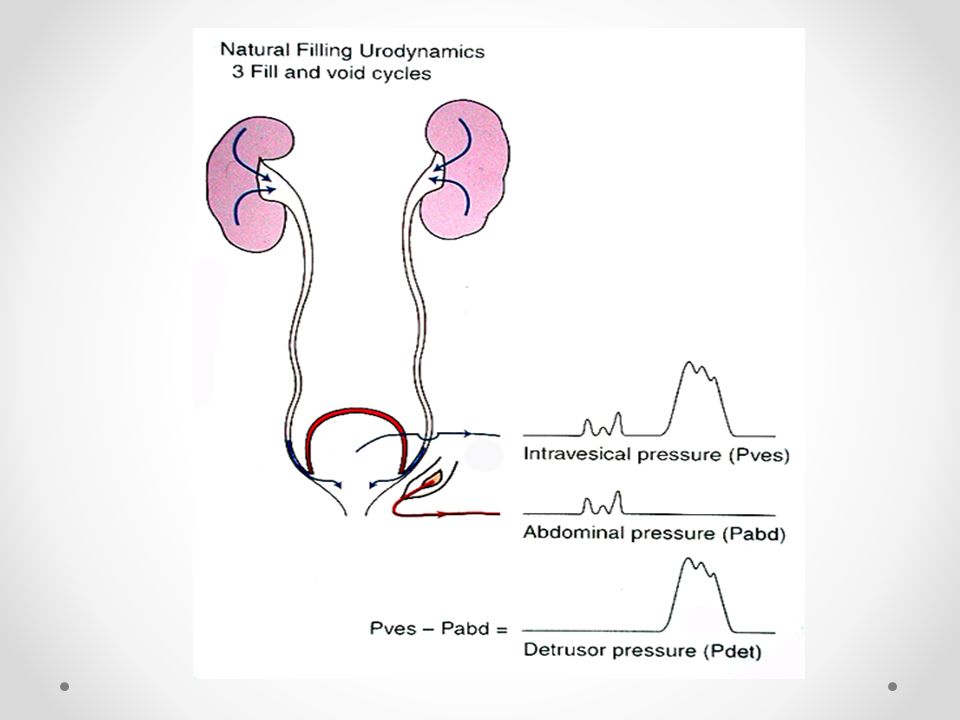
Rectal catheter -abdominal pressure Bladder catheter -intravesical pressure Invasive Urodynamics

30
Filling Phase Detrusor overactivity (Instability) - neurogenic / idiopathic Compliance (< 10cm water change for EBC) Bladder Capacity Sensation - reduced / absent Urgency Leak Vesicoureteric reflux
 - neurogenic / idiopathic Compliance (< 10cm water change for EBC) Bladder Capacity Sensation - reduced / absent Urgency Leak Vesicoureteric reflux")
31
Bladder Capacity Over 2 years age (age in years + 2) 30 = volume ml (Koff 1983) e.g. (5 + 2) 30 = 210 ml 30 + (age in years x 30) (Hjalmas 1988) e.g. 30 + (5 x 30) = 180 ml (+/- 80 ml)
 30 = 210 ml 30 + (age in years x 30) (Hjalmas 1988) e.g (5 x 30) = 180 ml (+/- 80 ml).")
32
Bladder Capacity Under 2 years age 38 + (age in months x 2.5) (Holmdahl 1996) e.g. 38 + (10 mo. x 2.5) = 63 ml 7.0 x weight kg (Koff 1983) e.g. 10 kg x 7 = 70 ml o Poor correlation with weight
 = 63 ml 7.0 x weight kg (Koff 1983) e.g. 10 kg x 7 = 70 ml o Poor correlation with weight.")
33
Compliance Change in volume / unit change in pressure (mls / cm H 2 O) o poor comparative ‘standard’ 500 ml / 5 cm H 2 O = 100 500 ml / 40 cm H 2 O = 12.5 70 ml / 5 cm H 2 O= 14
 o poor comparative ‘standard’ 500 ml / 5 cm H 2 O = ml / 40 cm H 2 O = ml / 5 cm H 2 O= 14")
34
Compliance

35
Compliance With bladder filling-: 1. Bladder unfolds from collapsed state 2. Elastic and Viscoelastic properties allow stretch o Elasticity - stretch without increase in tension o Viscoelasticity 1st - increased tension 2nd - tension decay (stress relaxation)
.")
36
Factors Affecting Compliance Alter the relationship between rate of stretch and rate of stretch relaxation Remember Normal bladder will reach the limit of compliance when over-filled o e.g. with active inhibition of micturition

37
Factors Affecting Compliance: Fill rates rate of stretch > rate of stretch relaxation = ↑ P Ves. Bladder wall constituents o fibrosis / hypertophy alter plasticity Neurological mediation o to relax the detrusor (Edvarson 1968) o to actively inhibit contraction (De Groat & Booth 1980)
 o to actively inhibit contraction (De Groat & Booth 1980).")
38
Poor Compliance - may result from: Passsive viscoelasticity due to fibrotic bladder Active viscoelastic behavior giving increased active tonus ? Passive loss of compliance vs. hyperreflexia or ‘detrusor overactivity’

39
Poorly Compliant Bladder

40
Voiding Phase Hesitancy Pattern Pdet Max Pdet at Q Max Flow – continuous / interrupted Reflux / Bladder neck / Urethra Residual / Secondary filling Flow rate

41
Natural Filling Urodynamics No artificial bladder filling Bladder fills naturally from the upper tracts Bladder pressure / voiding monitored over several hours Applications When other methods fail to disclose problem Babies Research

43
Natural Fill Urodynamics

44
Ward Urodynamics (Artificial Fill CMG) Advantages: Pressure – Flow ♂ and ♀ Conducive Enviornment Disadvantage: No flouroscpic imaging Therefore no information Regarding VUR, BOO, or Secondary refilling
 Advantages: Pressure – Flow ♂ and ♀ Conducive Enviornment Disadvantage: No flouroscpic imaging Therefore no information Regarding VUR, BOO, or Secondary refilling")
45
VOID

46
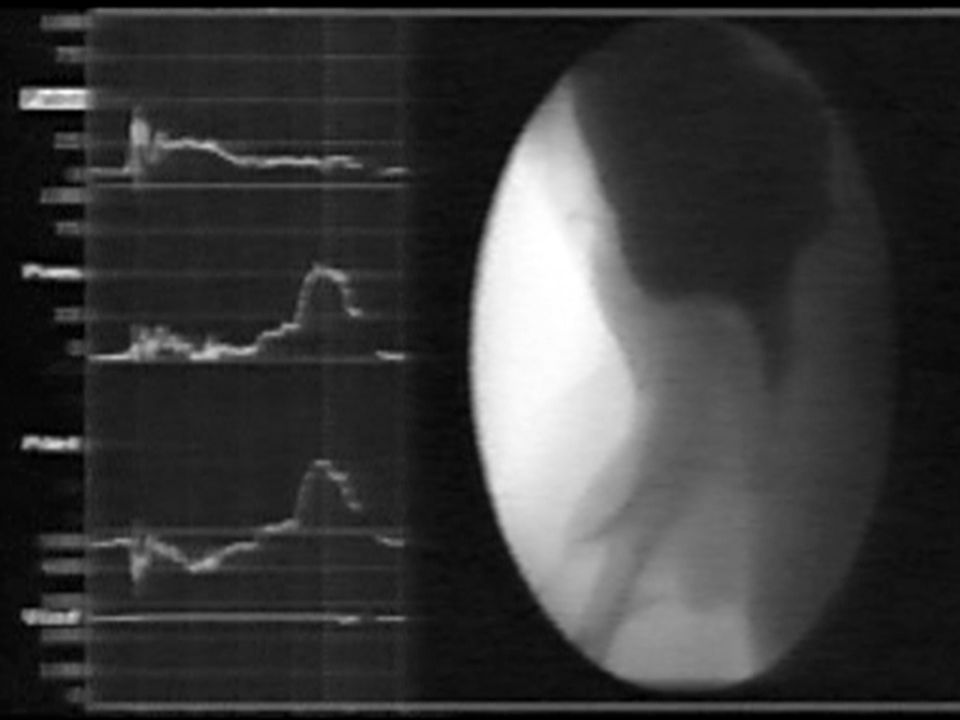
Video Urodynamics Anatomy plus Function Suspected bladder outflow obstruction Suspected neuropathology VUR? Inexplicable wetting o bladder base / neck o diverticulae o anatomical errors

47
Video Urodynamic Suite

49
Pitfalls Temperature of filling fluid Rate of Bladder Filling (Use of Pump) Vesico-ureteric reflux – Capacity/Compliance Residual Urine After Contraction Urethral Instrumentation
 Vesico-ureteric reflux – Capacity/Compliance Residual Urine After Contraction Urethral Instrumentation")
50
Conclusion Non-invasive assessment as baseline Tailor invasive urodynamics to suit individual cases Rapport essential to obtain useful information from these tests Anticipate and avoid pitfalls wherever possible Repeat investigation (? Different type) if results do not correlate with clinical history Correlate findings with results of other investigative modalities like ultrasound and isotope renography Tailor management to suit individual / family
 if results do not correlate with clinical history Correlate findings with results of other investigative modalities like ultrasound and isotope renography Tailor management to suit individual / family.")
Similar presentations

















,MRCGP,MRCPE.>")

