Download presentation
Presentation is loading. Please wait.

1
Management of vaginal bleeding in pregnancy

2
Vaginal bleeding is common in the first trimester, occurring.g in 20 to 40 percent of pregnant women.

3
The four major sources of nontraumatic bleeding in early pregnancy are: ●Ectopic pregnancy ●Miscarriage (threatened, inevitable, incomplete, complete) ●Implantation of the pregnancy ●Cervical, vaginal, or uterine pathology (eg, polyps, inflammation/infection, trophoblastic disease)
 ●Implantation of the pregnancy ●Cervical, vaginal, or uterine pathology (eg, polyps, inflammation/infection, trophoblastic disease)")
4
the goal of the evaluation is to make a definitive diagnosis when possible and exclude the presence of serious pathology in the remaining cases.

6
Gentle percussion is preferred to deep palpation since it causes less pain and guarding. Midline pain is more consistent with miscarriage, while lateral pain is more consistent with ectopic pregnancy.

7
If the cervix appears closed and there are no obvious bleeding lesions, the speculum is removed and a bimanual pelvic examination is performed. With an ectopic pregnancy, findings on pelvic examination may include adnexal, cervical motion, or abdominal tenderness; an adnexal mass; and mild uterine enlargement. However, the physical examination is often unremarkable in a woman with a small, unruptured ectopic pregnancy.

8
in bleeding patients in whom sonography has previously confirmed a viable singleton intrauterine pregnancy, another examination is not necessary to exclude ectopic pregnancy or to confirm fetal viability if fetal heart motion can be detected by a handheld Doppler device. Additionally, there is no value in checking hCG concentration once the presence of an intrauterine pregnancy has been established sonographically.

10
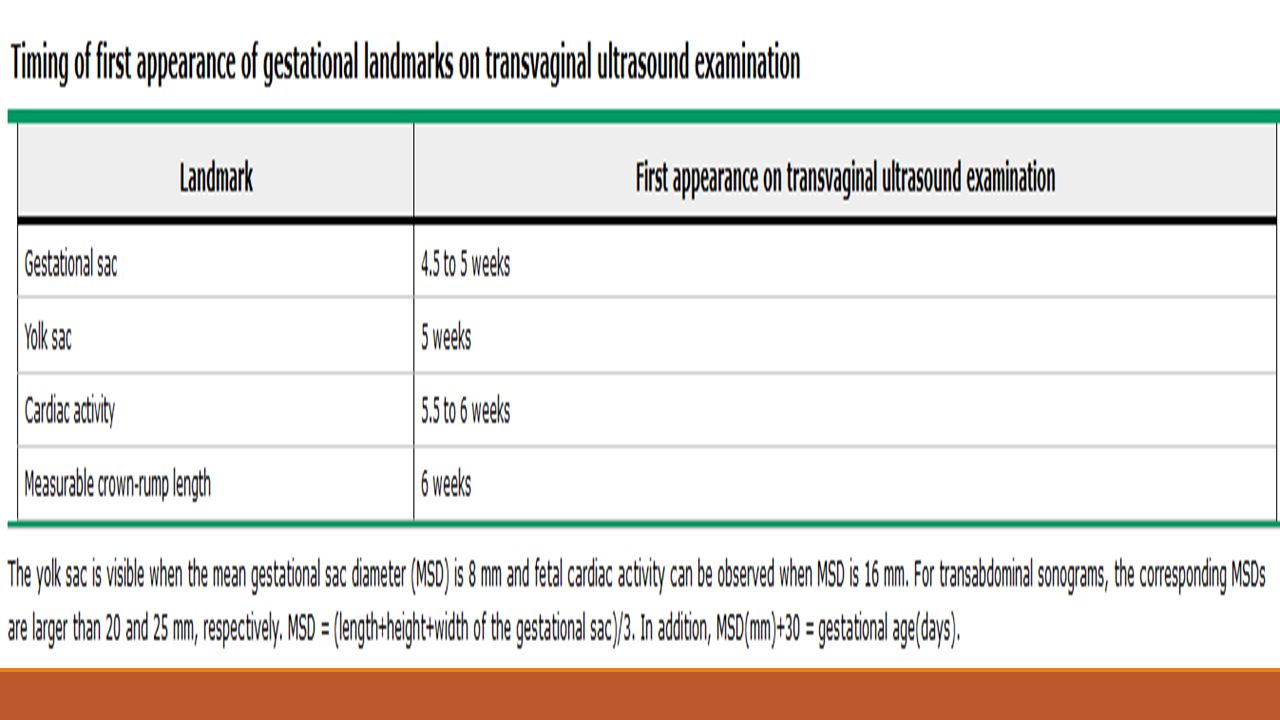
Transvaginal ultrasonography is the cornerstone of the evaluation of bleeding in early pregnancy. It is most useful in bleeding patients with a positive pregnancy test in whom an intrauterine pregnancy has not been previously confirmed by imaging studies. In these women, ultrasound examination is performed to determine whether the pregnancy is intrauterine or extrauterine (ectopic) and, if intrauterine, whether the pregnancy is viable (fetal cardiac activity present) or nonviable. The possibility of heterotopic pregnancy should always be considered.
 and, if intrauterine, whether the pregnancy is viable (fetal cardiac activity present) or nonviable. The possibility of heterotopic pregnancy should always be considered..")
11
Other imaging tests Magnetic resonance imaging is rarely indicated as a second-line imaging modality for further evaluation of limited and nondiagnostic ultrasound, unusual ectopic pregnancy, gestational trophoblastic disease, and differentiating causes of severe pelvic pain and adnexal masses. Computed tomography may be useful in pregnant patients with trauma or acute non-gynecologic pain, for staging of malignancy, or if magnetic resonance imaging is not possible.

12
Serial measurements of hCG are helpful during the first six weeks of pregnancy if ultrasonography is nondiagnostic, ie, the site and viability of the pregnancy are not revealed. Appropriately rising hCG levels are most consistent with a viable intrauterine pregnancy (99.9 percent of viable pregnancies display a rise in hCG greater than 35 percent over 48 hours, but 21 percent of ectopic pregnancies also display rising hCG levels.

13
Hemoglobin/hematocrit and coagulation studies should be obtained in all women who are hemodynamically unstable (hypotension, tachycardia, orthostasis, syncope). In hemodynamically stable patients, a baseline hemoglobin/hematocrit measurement can be useful in women with heavy vaginal bleeding, particularly if persistent, and in those with ruptured ectopic pregnancy.

14
Women with significant first trimester vaginal bleeding (ie, more than spotting) should have a red blood cell antibody screen checked. Those who are Rh(D) negative are given anti-D immunoglobulin to protect against Rh(D) isoimmunization, unless the vaginal bleeding is clearly due to a non-placental, nonfetal source, such as a vaginal laceration.
 negative are given anti-D immunoglobulin to protect against Rh(D) isoimmunization, unless the vaginal bleeding is clearly due to a non-placental, nonfetal source, such as a vaginal laceration..")
15
All women with early pregnancy bleeding and pain are assumed to have ectopic pregnancy until this diagnosis has been excluded by laboratory and imaging studies. Women with a history of ectopic pregnancy or other risk factors for the disorder are at highest risk, but many women with ectopic pregnancy have no risk factors.

16
However, the absence of a sonographically identifiable intrauterine pregnancy when the hCG concentration is greater than 2000 IU/L is not absolute proof of ectopic pregnancy. This threshold is somewhat institution- dependent and does not account for the possibility of a very early multiple gestation (hCG levels are higher in multiple gestations)
.")
17
90 to 96 percent of pregnancies with both fetal cardiac activity and vaginal bleeding at 7 to 11 weeks of gestation do not miscarry; the higher success rate is associated with bleeding at the later end of the gestational age range

18
Uterine bleeding in these cases is likely due to disruption of decidual vessels at the maternal-fetal interface. These separations generally cannot be visualized by ultrasound, but sometimes appear as a subchorionic hematoma. Management is expectant.

19
Inevitable miscarriage — When miscarriage is inevitable, the cervix is dilated, uterine bleeding is increasing, and painful uterine cramps/contractions are present. The gestational tissue often can be felt or seen through the cervical os; passage of this tissue typically occurs within a short time. Management may be expectant, or a medical or surgical intervention to complete the miscarriage can be undertaken.

20
Complete miscarriage — When a miscarriage occurs before 12 weeks of gestation, it is common for the entire contents of the uterus to be expelled, thereby resulting in a complete miscarriage. If this has occurred, the uterus is small on physical examination and well contracted with an open or closed cervix, scant vaginal bleeding, and only mild cramping. Ultrasound will reveal an empty uterus and no extrauterine gestation.

21
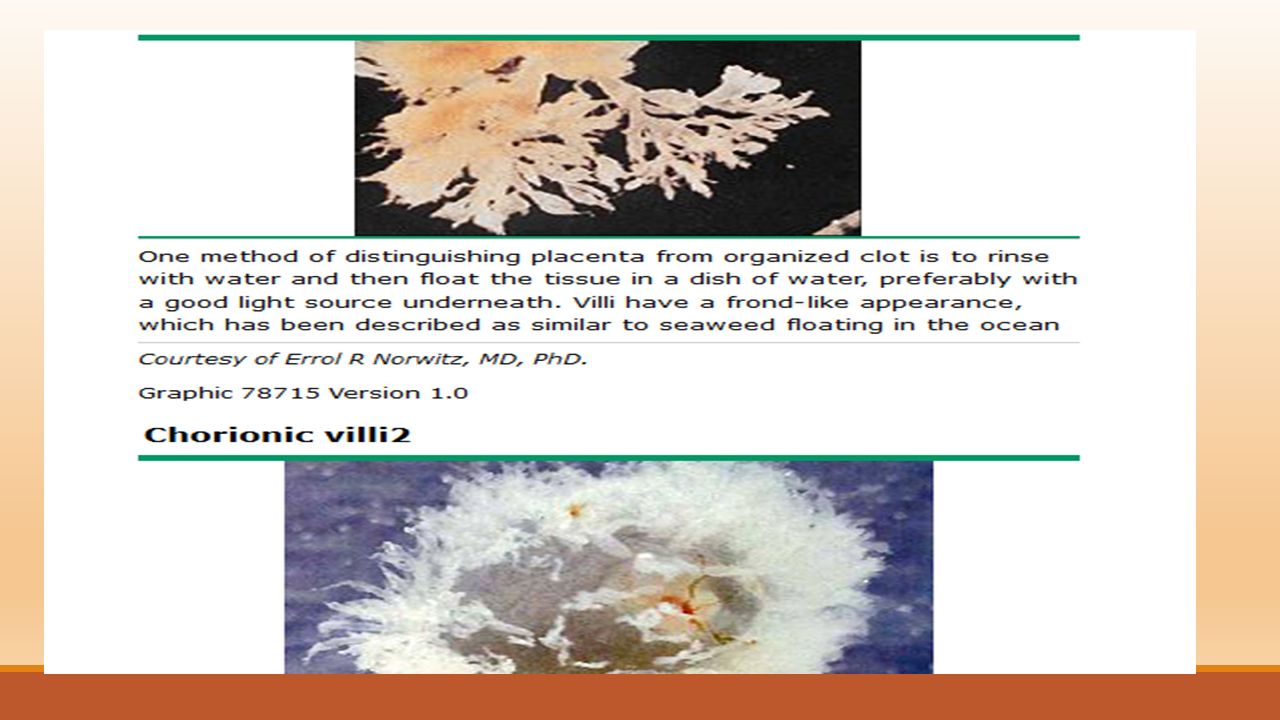
Incomplete miscarriage — The membranes may rupture and the fetus may be passed, but significant amounts of placental tissue can be retained, resulting in an incomplete miscarriage. This is most common in the late first trimester and early second trimester. On examination, the cervical os is open, gestational tissue may be observed in the cervix, and the uterine size is smaller than expected for gestational age, but not well contracted. The amount of bleeding varies, but can be severe enough to cause hypovolemic shock. Painful cramps/contractions are often present. Ultrasound reveals tissue in the uterus. Medical or surgical evacuation is generally performed.

22
Missed abortion — A missed abortion (also called a delayed miscarriage) refers to in-utero death of the embryo or fetus prior to the 20th week of gestation, with retention of the pregnancy for a prolonged period of time. Women may notice that symptoms associated with early pregnancy (eg, nausea, breast tenderness) have abated and they don't "feel pregnant" anymore. Vaginal bleeding may occur. The cervix usually remains closed. Ultrasound reveals an intrauterine gestational sac with or without an embryonic/fetal pole, but no embryonic/fetal cardiac activity. Management may be expectant or a medical or surgical intervention to complete the miscarriage can be undertaken.
 have abated and they don t feel pregnant anymore. Vaginal bleeding may occur. The cervix usually remains closed. Ultrasound reveals an intrauterine gestational sac with or without an embryonic/fetal pole, but no embryonic/fetal cardiac activity. Management may be expectant or a medical or surgical intervention to complete the miscarriage can be undertaken..")
23
Physiologic or implantation bleeding — This is a diagnosis of exclusion. It is characterized by a small amount of spotting or bleeding approximately 10 to 14 days after fertilization (at the time of the missed menstrual period), and is presumed to be related to implantation of the fertilized egg in the decidua (ie, lining of the uterus), although this hypothesis has been questioned. No intervention is indicated.
, and is presumed to be related to implantation of the fertilized egg in the decidua (ie, lining of the uterus), although this hypothesis has been questioned. No intervention is indicated..")
24
Studies consistently show an association between first trimester bleeding and adverse outcome (eg, miscarriage, preterm birth, premature rupture of membranes, fetal growth restriction) later in pregnancy. The prognosis is best when bleeding is light and limited to early pregnancy, ie, less than 6 weeks of gestation. The prognosis worsens when bleeding is heavy or extends into the second trimester. However, no change in pregnancy management is indicated for women with first trimester bleeding. There are no effective interventions, but women can be reassured of the low likelihood of adverse outcome. In particular, bedrest is unnecessary and will not affect outcome.

25
A retrospective registry-based study including over one million women found that, compared to women without bleeding, first trimester bleeding increased the risk of preterm birth at 28 to 31 weeks (0.9 versus 0.3 percent; OR 2.98, 95% CI 2.50-3.54) and at 32 to 36 weeks (6.1 versus 3.6 percent; OR 1.65, 95% CI 1.57-1.77), and increased the risk of placental abruption (1.4 versus 1.0 percent; OR 1.48; 95% CI 1.30-1.68)
 and at 32 to 36 weeks (6.1 versus 3.6 percent; OR 1.65, 95% CI ), and increased the risk of placental abruption (1.4 versus 1.0 percent; OR 1.48; 95% CI )")
26
SECOND AND THIRD TRIMESTER BLEEDING Bloody show associated with cervical insufficiency or labor (by definition, labor occurs after 20 weeks) ●Miscarriage (by definition, miscarriage occurs before 20 weeks) ●Placenta previa ●Abruptio placenta ●Uterine rupture ●Vasa previa
 ●Miscarriage (by definition, miscarriage occurs before 20 weeks) ●Placenta previa ●Abruptio placenta ●Uterine rupture ●Vasa previa")
27
Cervical insufficiency – The diagnosis of cervical insufficiency is clinical; the classic presentation is cervical dilatation and effacement in the second trimester with fetal membranes visible at or beyond the external os in the absence of contractions. Symptoms include one or more of the following: vaginal fullness or pressure; vaginal spotting or bleeding; an increased volume of watery, mucousy, or brown vaginal discharge; and vague discomfort in the lower abdomen or back. In asymptomatic patients, the sonographic finding of a short cervix in a woman with a previous preterm birth supports the diagnosis

28
The term antepartum bleeding typically refers to uterine bleeding after 20 weeks of gestation that is unrelated to labor and delivery. Antepartum bleeding complicates 4 to 5 percent of pregnancies. The major causes are: ●Placenta previa (20 percent) ●Abruptio placenta (30 percent) ●Uterine rupture (rare) ●Vasa previa (rare)
 ●Abruptio placenta (30 percent) ●Uterine rupture (rare) ●Vasa previa (rare).")
29
The risk of adverse outcome appears to depend on the degree of bleeding (worse outcome with heavier bleeding) and the cause (worse outcome with bleeding from non- previa source). Antepartum bleeding of unknown origin in the second half of pregnancy has been reported to increase the risk of preterm birth two- to three-fold.

30
Choosing a treatment method — Women with an incomplete, inevitable, or missed abortion can be managed with surgical (dilation and curettage) or medication (misoprostol) uterine evacuation or with expectant management. All three approaches have similar efficacy, and the choice of treatment method depends mainly upon patient preference.misoprostol

Similar presentations






 and abnormalities of the Third Stage Sept 12 – Dr. Z. Malewski.>")













