Download presentation
Presentation is loading. Please wait.

1
RHEUMATOID ARTHRITIS Melanie Laine, PharmD PGY1 Pharmacy Resident University of Kentucky HealthCare April 22, 2015

2
LEARNING OBJECTIVES Recognize the symptoms and characteristics of rheumatoid arthritis (RA) Compare and contrast available pharmacologic therapies for RA Design individualized therapeutic regimens and monitoring plans for patients with RA
 Compare and contrast available pharmacologic therapies for RA Design individualized therapeutic regimens and monitoring plans for patients with RA")
3
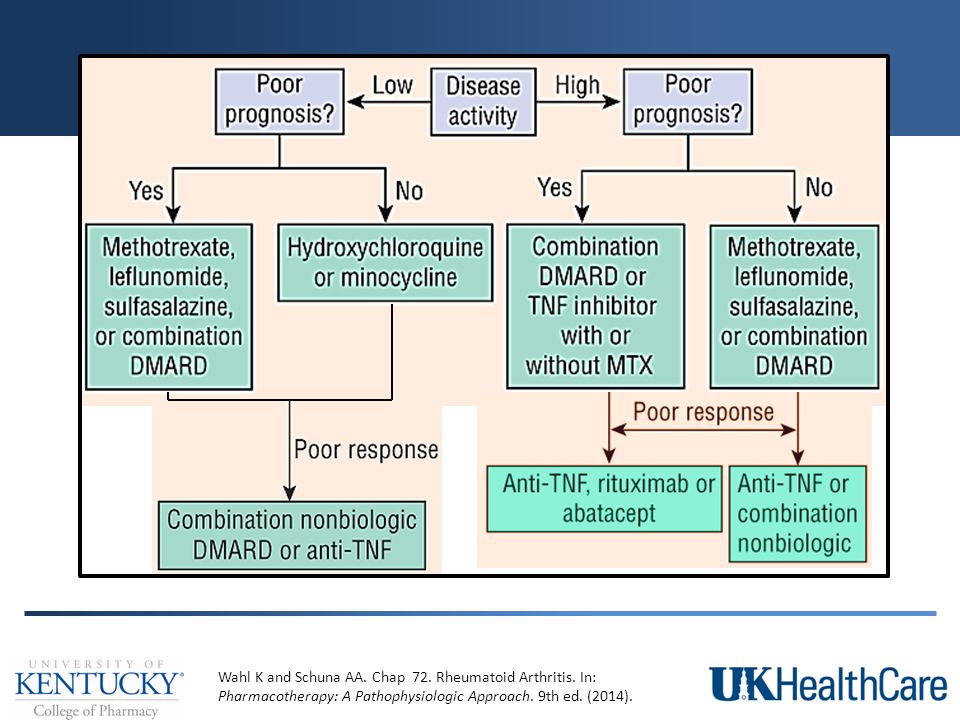
RHEUMATOID ARTHRITIS Chronic, systemic inflammatory disease Autoimmune Characterized by symmetrical inflammation of joints Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
4
EPIDEMIOLOGY Most common systemic inflammatory disease Prevalence: 1-2% Occurrence: Any age 3:1 in females Unknown etiology Interplay between genetic predisposition and environmental triggers Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). McInnes IB and Schett G. New Engl J Med. 2011; 365 (23): 2205-19.
. McInnes IB and Schett G. New Engl J Med. 2011; 365 (23):")
5
PATHOPHYSIOLOGY Autoimmune disease Lack of differentiation between self and non-self tissues Destruction of synovial and connective tissues Pannus Inflamed, proliferating synovium Invades cartilage and bone surface joint destruction Characteristic of RA Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
6
Vollenhoven RF. Nat Rev Rheumatol. 2009; 5 (10): 531-41. Drug Targets: TNF α IL-1 IL-6 B cells JAK
: Drug Targets: TNF α IL-1 IL-6 B cells JAK")
7
PATHOPHYSIOLOGY Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). LYMPHOCYTES PRO-INFLAMMATORY CYTOKINES B LymphocytesT LymphocytesTNF α, IL-1, IL-6, IL-17 Origin: bone marrow Produce rheumatoid factor and anticyclic citrullinated peptide Attract neutrophils to sites of injury Act an APCs to stimulate T cells and activate the immune process Origin: thymus Produce cytokines and cytotoxins Further promote inflammation and tissue destruction Stimulate macrophages to release prostaglandins and cytotoxins Initiate and continue inflammatory process Stimulate osteoclast formation Suppress osteoblasts and bone formation APCs = antigen-presenting cells
. LYMPHOCYTES PRO-INFLAMMATORY CYTOKINES B LymphocytesT LymphocytesTNF α, IL-1, IL-6, IL-17 Origin: bone marrow Produce rheumatoid factor and anticyclic citrullinated peptide Attract neutrophils to sites of injury Act an APCs to stimulate T cells and activate the immune process Origin: thymus Produce cytokines and cytotoxins Further promote inflammation and tissue destruction Stimulate macrophages to release prostaglandins and cytotoxins Initiate and continue inflammatory process Stimulate osteoclast formation Suppress osteoblasts and bone formation APCs = antigen-presenting cells.")
8
CLINICAL PRESENTATION Develop over several weeks to months Constitutional symptoms: fever, fatigue, weakness, loss of appetite Tenderness, warmth, and swelling over affected joints Muscle aches and stiffness Joint deformity (late disease) Symmetrical joint involvement Joint pain and stiffness > 6 weeks Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
9
CLINICAL PRESENTATION Morning stiffness > 30 minutes Decreased range of motion and grip strength Stenosing flexor tenosynovitis (trigger fingers) Extraarticular involvement Laboratory abnormalities Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
10
EXTRAARTICULAR INVOLVEMENT Rheumatoid nodules Vasculitis Pulmonary complications Ocular involvement Keratoconjunctivitis sicca Sjogren’s syndrome Cardiac involvement Felty’s syndrome Splenomegaly Neutropenia Thrombocytopenia Lymphadenopathy Rare complications Kidney injury Amyloidosis Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
11
LABORATORY FINDINGS ↑ erythrocyte sedimentation rate (ESR) ↑ C-reactive protein (CRP) (+) Rheumatoid factor (RF) (+) Anticyclic citrullinated peptide (anti-CCP) Synovial fluid: turbid with many leukocytes Radiographic imaging Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
12
2010 ACR CLASSIFICATION CRITERIA Aletaha D et al. Arthritis Rheum. 2010; 62 (9): 2569-81. > 6/10 for classification of definite RASCORE Joint involvement1 large joint0 2-10 large joints1 1-3 small joints2 4-10 small joints3 > 10 joints (at least one small)5 Serology (> 1)Negative RF and negative anti-CCP Abs0 Low-positive RF or low-positive anti-CCP Abs2 High-positive RF or high-positive anti-CCP Abs3 Acute phase reactantsNormal ESR and normal CRP0 Abnormal ESR or abnormal CRP1 Symptom duration< 6 weeks0 > 6 weeks1 Large joints = shoulders, elbows, hips, knees, ankles Small joints = metacarpophalangeal joints, proximal interphalangeal joints, metatarsophalangeal joints, thumb, wrists
: > 6/10 for classification of definite RASCORE Joint involvement1 large joint large joints1 1-3 small joints small joints3 > 10 joints (at least one small)5 Serology (> 1)Negative RF and negative anti-CCP Abs0 Low-positive RF or low-positive anti-CCP Abs2 High-positive RF or high-positive anti-CCP Abs3 Acute phase reactantsNormal ESR and normal CRP0 Abnormal ESR or abnormal CRP1 Symptom duration< 6 weeks0 > 6 weeks1 Large joints = shoulders, elbows, hips, knees, ankles Small joints = metacarpophalangeal joints, proximal interphalangeal joints, metatarsophalangeal joints, thumb, wrists.")
13
RA VERSUS OSTEOARTHRITIS RHEUMATOID ARTHRITIS Morning stiffness > one hour, worse with activity ↑ incidence females (3:1) ~ Age ↑ ESR Systemic symptoms ~ Obesity Wrists, hands, feet Symmetrical OSTEOARTHRITIS Morning stiffness < 30 minutes, resolves with activity Equal gender prevalence ↑ Age Normal ESR Local symptoms ↑ Obesity Hands, knees, hips, spine Asymmetrical Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
14
PREDICTORS OF WORSE OUTCOME Older age Female gender Genotype (HLA-DRB1) Worse physical functioning Cigarette smoking Saag KG et al. Arthritis Rheum. 2008; 59 (6): 762-84.
:")
15
PROGNOSTIC FACTORS Functional limitation Extraarticular disease RF and/or anti-CCP antibody positivity Bony erosions on radiographic imaging Management of comorbidities Disease duration and activity are also important when assessing prognosis Saag KG et al. Arthritis Rheum. 2008; 59 (6): 762-84.
:")
16
COMORBIDITIES Must be addressed in order to decrease morbidity and mortality Comorbidities with greatest impact: Infection Osteoporosis Cardiovascular disease O’Dell JR. New Engl J Med. 2004; 350 (25): 2591-602.
:")
17
PATIENT CASE #1 MJ is a 36 year old female who presents to her PCP c/o joint pain in her hands and wrists (~6 joints) that has persisted for the past 2 months. She receives little relief from OTC NSAIDs, and on examination, the joints on both hands appear red and swollen. Laboratory testing shows positive RF and anti-CCP antibodies (high-positive) and ↑ ESR. What signs and symptoms are indicative of RA? What is MJ’s score using the 2010 ACR classification criteria for definite RA?
 and ↑ ESR. What signs and symptoms are indicative of RA. What is MJ’s score using the 2010 ACR classification criteria for definite RA .")
18
GOALS OF TREATMENT Control disease activity and joint pain Maintain function in daily activities Slow destructive joint damage Achieve and maintain disease remission Improve or maintain functional status and quality of life Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). O’Dell JR. New Engl J Med. 2004; 350 (25): 2591-602.
. O’Dell JR. New Engl J Med. 2004; 350 (25):")
19
TREATMENT OVERVIEW Non-pharmacologic therapy Pharmacologic therapy Non-disease modifying drugs NSAIDs Corticosteroids Disease-modifying antirheumatic drugs (DMARDs) Non-biologic Biologic
 Non-biologic Biologic")
20
NON-PHARMACOLOGIC Rest Physical and occupational therapy Assistive devices Weight reduction Surgery Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
21
Non-disease modifying drugs PHARMACOLOGIC THERAPY

22
NSAIDs Analgesic and anti-inflammatory properties Rapid symptomatic relief for pain and stiffness Adverse effects: ulcers and GI bleeding, renal impairment, hypertension, fluid retention Helpful during the first few weeks until definitive diagnosis is made Adjunct to DMARD therapy Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). O’Dell JR. New Engl J Med. 2004; 350 (25): 2591-602.
. O’Dell JR. New Engl J Med. 2004; 350 (25):")
23
CORTICOSTEROIDS Suppress inflammatory response Bridge to effective DMARD therapy Rapid symptomatic relief Dose: Prednisone < 10mg PO daily Adverse effects: hypertension, hyperlipidemia, hyperglycemia, fat redistribution, cataracts, osteoporosis, etc. Adjunct to DMARD therapy LexiComp Online. online.lexi.com. Accessed April 12, 2015. O’Dell JR. New Engl J Med. 2004; 350 (25): 2591-602.
:")
24
DMARDs PHARMACOLOGIC THERAPY

25
DMARDs Retard or halt the progression of RA Sustained suppression of inflammation Initiate < 3 months of symptom onset Improve outcomes Reduce mortality All patients except those with limited disease Slow onset with regard to symptom management Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). O’Dell JR. New Engl J Med. 2004; 350 (25): 2591-602.
. O’Dell JR. New Engl J Med. 2004; 350 (25):")
26
NON-BIOLOGIC DMARDs Methotrexate Leflunomide Hydroxychloroquine Sulfasalazine Minocycline

27
METHOTREXATE Folate antimetabolite inhibits purine synthesis May inhibit cytokine production and stimulate adenosine release Initial therapy of choice: most likely to induce long-term response Dose: 7.5-15mg PO once weekly Onset: 2-3 weeks Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). O’Dell JR. New Engl J Med. 2004; 350 (25): 2591-60. LexiComp Online. online.lexi.com. Accessed April 12, 2015.
. O’Dell JR. New Engl J Med. 2004; 350 (25): LexiComp Online. online.lexi.com. Accessed April 12,")
28
METHOTREXATE Adverse effects: diarrhea, N/V, stomatitis, thrombocytopenia > leukopenia, ↑ LFTs* Folic acid 1-3mg PO daily Decreases toxic effects without compromising efficacy Contraindications: Pregnancy Liver or kidney disease Alcohol use Blood dyscrasias Effusions Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). LexiComp Online. online.lexi.com. Accessed April 12, 2015. *Discontinue therapy if sustained increase > 2x ULN
. LexiComp Online. online.lexi.com. Accessed April 12, *Discontinue therapy if sustained increase > 2x ULN.")
29
LEFLUNOMIDE Inhibits pyrimidine synthesis decreased lymphocyte proliferation Similar long-term efficacy to MTX Dose: 100mg PO daily x 3 days, then 20mg daily Onset: 4 weeks Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
30
LEFLUNOMIDE Adverse effects: ↑ LFTs, pancytopenia Enterohepatic recycling prolongs elimination half life Cholestyramine can rapidly decrease plasma levels Contraindications: Pregnancy Pre-existing liver disease Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). LexiComp Online. online.lexi.com. Accessed April 12, 2015. *Discontinue therapy if sustained increase > 3x ULN
. LexiComp Online. online.lexi.com. Accessed April 12, *Discontinue therapy if sustained increase > 3x ULN.")
31
HYDROXYCHLOROQUINE Inhibits PMN migration and eosinophil chemotaxis; impairs Ag-Ab reactions Least potent, but best tolerated Recommended for patients without poor prognostic factors, low disease activity, duration < 24 months Dose: 200-300mg PO BID x 1-2 months, then can decrease to 200mg daily or BID Onset: 6 weeks Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). LexiComp Online. online.lexi.com. Accessed April 12, 2015.
. LexiComp Online. online.lexi.com. Accessed April 12,")
32
HYDROXYCHLOROQUINE Adverse effects: diarrhea, N/V, ocular toxicity, rash, alopecia Limited monitoring Contraindications: Vision changes from therapy Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). LexiComp Online. online.lexi.com. Accessed April 12, 2015.
. LexiComp Online. online.lexi.com. Accessed April 12,")
33
SULFASALAZINE Prodrug 5-aminosalicylic and sulfapyridine MOA unknown First DMARD: similar efficacy to MTX Dose: 500mg-1000mg PO daily initially, then 1000mg PO BID (max 3000mg daily) Onset: 8 weeks Use limited by adverse effects Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). O’Dell JR. New Engl J Med. 2004; 350 (25): 2591-60. LexiComp Online. online.lexi.com. Accessed April 12, 2015.
. O’Dell JR. New Engl J Med. 2004; 350 (25): LexiComp Online. online.lexi.com. Accessed April 12,")
34
SULFASALAZINE Adverse effects: diarrhea, N/V, anorexia, rash urticaria, serum sickness*, alopecia, stomatitis, ↑ LFTs, myelosuppression Contraindications: sulfa allergy Drug interactions Antibiotics Iron supplements Warfarin Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). LexiComp Online. online.lexi.com. Accessed April 12, 2015. *Treat with antihistamines ± corticosteroids
. LexiComp Online. online.lexi.com. Accessed April 12, *Treat with antihistamines ± corticosteroids.")
35
MINOCYCLINE Tetracycline antibiotic; may inhibit metalloproteinases Mild disease without poor prognostic factors Limited data Dose: 100-200mg PO daily Adverse reactions: minimal Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
36
PATIENT CASE #1 MJ is diagnosed with RA. After diagnosis, she is referred to a rheumatologist who wishes to start her on a DMARD as soon as possible. She does not have any pertinent PMH and has a sulfa allergy. She also mentions that she and her husband are trying to get pregnant. Out of the non-biologic DMARDs, what is the best option for initial therapy for MJ?

37
SUMMARY: NON-BIOLOGICS Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). LexiComp Online. online.lexi.com. Accessed April 12, 2015. DRUGDOSEMONITORING MethotrexatePO/IM: 7.5-15mg weekly Baseline LFTs, CBC, SCr/BUN, hepatitis panel CBC, AST/ALT, albumin q1-2 months Leflunomide PO: 100mg daily x 3 days, then 10-20 daily OR 10-20 mg daily w/o LD Baseline LFTs, CBC CBC, AST/ALT monthly, then q6-8 weeks Hydroxychloroquine PO: 200-300mg BID x 1-2 months, then can ↓ to 200mg daily or BID Baseline eye exam Ophthalmoscopy q9-12 months Sulfasalazine PO: 500mg BID, then ↑ to 1000mg BID Baseline CBC CBC weekly x 1 month, then q1-2 months MinocyclinePO: 100-200mg daily LFTs, BUN/SCr with long-term treatment
. LexiComp Online. online.lexi.com. Accessed April 12, DRUGDOSEMONITORING MethotrexatePO/IM: mg weekly Baseline LFTs, CBC, SCr/BUN, hepatitis panel CBC, AST/ALT, albumin q1-2 months Leflunomide PO: 100mg daily x 3 days, then daily OR mg daily w/o LD Baseline LFTs, CBC CBC, AST/ALT monthly, then q6-8 weeks Hydroxychloroquine PO: mg BID x 1-2 months, then can ↓ to 200mg daily or BID Baseline eye exam Ophthalmoscopy q9-12 months Sulfasalazine PO: 500mg BID, then ↑ to 1000mg BID Baseline CBC CBC weekly x 1 month, then q1-2 months MinocyclinePO: mg daily LFTs, BUN/SCr with long-term treatment.")
38
BIOLOGIC DMARDs Infliximab Etanercept Adalimumab Golimumab Certolizumab Anakinra Abatacept Ritubimab Toclizumab Tofacitinib

39
Vollenhoven RF. Nat Rev Rheumatol. 2009; 5 (10): 531-41. Drug Targets: TNF α IL-1 IL-6 B cells JAK
: Drug Targets: TNF α IL-1 IL-6 B cells JAK")
40
BIOLOGIC DMARDs Genetically engineered protein molecules that target pro-inflammatory cytokines or lymphocytes Not considered first line therapy High disease activity with poor prognostic factors May be effective when non-biologic DMARDs have failed Expensive Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). Singh JA et al. Arthrit Care Res. 2012; 64 (5): 625-39.
. Singh JA et al. Arthrit Care Res. 2012; 64 (5):")
41
TNF α INHIBITORS Inactivate TNF α, preventing interaction with receptor and inhibiting immune cell activation Increased infection risk Tuberculosis: must test prior to initiation Avoid live vaccines Multiple sclerosis-like illness Increased risk for lymphoma and other cancers Contraindication: NYHA class III-IV heart failure Saag KG et al. Arthritis Rheum. 2008; 59 (6): 762-84. LexiComp Online. online.lexi.com. Accessed April 12, 2015.
: LexiComp Online. online.lexi.com. Accessed April 12,")
42
TNF α INHIBITORS Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). Singh JA et al. Arthrit Care Res. 2012; 64 (5): 625-39. LexiComp Online. online.lexi.com. Accessed April 12, 2015. DRUGDOSEADVERSE REACTIONSCOMMENTS InfliximabIV: 3 mg/kg at 0, 2, & 6 weeks, then q8 weeks Infusion reactions: flu-like symptoms Given with MTX to prevent Ab formation (superior to monotherapy) EtanerceptSQ: 50mg once weekly OR 25mg two times a week Local injection-site reactions Avoid in MS Preferred with HCV May slow erosive disease > MTX AdalimumabSQ: 40mg every 2 weeksLocal injection-site reactions Less antigenic than infliximab GolimumabSQ: 50mg once a month IV: 2 mg/kg at 0 & 4 weeks, then q8 weeks Local injection site reactions Given in combination with MTX CertolizumabSQ: 200mg at 0, 2, & 4 weeks, then every 2 weeks Local injection site reactions Nausea Given as monotherapy or in combination with MTX
. Singh JA et al. Arthrit Care Res. 2012; 64 (5): LexiComp Online. online.lexi.com. Accessed April 12, DRUGDOSEADVERSE REACTIONSCOMMENTS InfliximabIV: 3 mg/kg at 0, 2, & 6 weeks, then q8 weeks Infusion reactions: flu-like symptoms Given with MTX to prevent Ab formation (superior to monotherapy) EtanerceptSQ: 50mg once weekly OR 25mg two times a week Local injection-site reactions Avoid in MS Preferred with HCV May slow erosive disease > MTX AdalimumabSQ: 40mg every 2 weeksLocal injection-site reactions Less antigenic than infliximab GolimumabSQ: 50mg once a month IV: 2 mg/kg at 0 & 4 weeks, then q8 weeks Local injection site reactions Given in combination with MTX CertolizumabSQ: 200mg at 0, 2, & 4 weeks, then every 2 weeks Local injection site reactions Nausea Given as monotherapy or in combination with MTX.")
43
B CELL DEPLETING AGENT Rituximab Depletes peripheral B cells by binding CD20 Recovery takes several months – intermittent therapy For patients who have failed MTX therapy or TNF α inhibitors (second line) Also preferred in recently treated solid malignancy and PMH of treated lymphoma or skin melanoma Better outcomes when given with MTX Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). Singh JA et al. Arthrit Care Res. 2012; 64 (5): 625-39.
. Singh JA et al. Arthrit Care Res. 2012; 64 (5):")
44
B CELL DEPLETING AGENT Dose: 1000mg IV at 0 and 2 weeks Adverse reactions: Infusion reactions – pre-medicate* HBV reactivation – screen prior to initiation Black box warning for fatal infusion reactions Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). LexiComp Online. online.lexi.com. Accessed April 12, 2015. *Acetaminophen, diphenhydramine, and methylprednisolone 30 minutes prior to infusion
. LexiComp Online. online.lexi.com. Accessed April 12, *Acetaminophen, diphenhydramine, and methylprednisolone 30 minutes prior to infusion.")
45
CD80/CD86 CO-STIMULATOR MODULATOR Abatacept Binds to antigen-presenting cells, preventing interaction with T cells and subsequent T cell activation For patients who have failed MTX therapy or TNF α inhibitors Response rate of 50% in clinical trials Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). Singh JA et al. Arthrit Care Res. 2012; 64 (5): 625-39.
. Singh JA et al. Arthrit Care Res. 2012; 64 (5):")
46
CD80/CD86 CO-STIMULATOR MODULATOR Weight-based dosing: IV infusion at 0, 2, & 4 weeks, then q4 weeks < 60kg: 500mg 60-100kg: 750mg > 100kg: 1000mg Alternative: 125mg SQ weekly Adverse reactions: headache, nausea, nasopharyngitis, infection, infusion reactions Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). LexiComp Online. online.lexi.com. Accessed April 12, 2015.
. LexiComp Online. online.lexi.com. Accessed April 12,")
47
INTERLEUKIN-6 INHIBITOR Tocilizumab IL-6 receptor antagonist, reducing production of cytokines and acute phase reactants For patients who have failed MTX therapy or TNF α inhibitors Can be as monotherapy or in combination with MTX Singh JA et al. Arthrit Care Res. 2012; 64 (5): 625-39. LexiComp Online. online.lexi.com. Accessed April 12, 2015.
: LexiComp Online. online.lexi.com. Accessed April 12,")
48
INTERLEUKIN-6 INHIBITOR Dose: IV: 4-8 mg/kg q4 weeks (max dose 800mg) SQ: 162mg every other week ( 100kg) Adverse reactions: infusion reactions, hyperlipidemia, ↑ LFTs*, infection Monitoring: baseline and periodic CBC and LFTs LexiComp Online. online.lexi.com. Accessed April 12, 2015. *Discontinue therapy if sustained increase > 5x ULN

49
INTERLEUKIN-1 INHIBITOR Anakinra IL-1 receptor antagonist, preventing migration of inflammatory leukocytes to tissues Literature suggests less efficacy No longer included in guideline recommendations Patients who fail MTX and TNF α inhibitors Should not be used with TNF α inhibitors Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
50
INTERLEUKIN-1 INHIBITOR Dose: 100mcg SQ daily Adverse reactions: local injection-site reactions, headache, arthralgias, neutropenia (rare), infection Monitoring: Baseline: TB test, PMN count PMN count monthly x 3 months, then q3 months for one year Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014). LexiComp Online. online.lexi.com. Accessed April 12, 2015.
. LexiComp Online. online.lexi.com. Accessed April 12,")
51
JANUS KINASE (JAK) INHIBITOR Xeljanz (tofacitinib) FDA approved in 2012 Moderate to severe RA refractory to MTX Versus placebo and MTX: significantly less symptoms and improved physical function Dose: 5mg PO BID LexiComp Online. online.lexi.com. Accessed April 12, 2015. Pfizer Laboratories, Inc. Xeljanz (tofacitinib) Package Insert. Fleischmann R et al. New Engl J Med. 2012; 367 (6): 495-507. Lee EB et al. New Engl J Med. 2014; 370 (25): 2377-86.
 Package Insert. Fleischmann R et al. New Engl J Med. 2012; 367 (6): Lee EB et al. New Engl J Med. 2014; 370 (25):")
52
JANUS KINASE (JAK) INHIBITOR Adverse effects: diarrhea, headache, infections, malignancy Must test for tuberculosis and hepatitis B/C prior to therapy initiation Monitoring: Baseline: hepatitis panel, TB test, LFTs, CBC, Hgb/Hct Lipids in 4-8 weeks then periodically CBC, Hgb/Hct q3 months LexiComp Online. online.lexi.com. Accessed April 12, 2015. Pfizer Laboratories, Inc. Xeljanz (tofacitinib) Package Insert.
 Package Insert..")
53
OTHER AGENTS Gold salts, azathioprine, D-penicillamine, cyclosporine, and cyclophosphamide Infrequently used or not recommended Toxicity Lack of long-term benefit Both Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
54
COMBINATION THERAPY Typically effective when monotherapy fails May be appropriate initially in moderate to high disease activity Biologics in combination with MTX may be more effective than biologic monotherapy Combination therapy with > one biologic is not recommended Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
56
PATIENT CASE #2 JF is a 63 year old female who was recently diagnosed with RA. PMH significant for osteoporosis. She reports difficulty performing her daily activities and painful, swollen joints that keep her up at night. She has high disease activity with the presence of bony erosions on imaging. What RA treatments would you consider for JF? What other recommendations might you make?

57
EVALUATION OF THERAPY Clinical signs and symptoms of RA Swelling, warmth, and tenderness Pain, stiffness, and functional limitations Radiographic imaging Adverse effects and other drug monitoring American College of Rheumatology Improvement Criteria ACR20: 20% improvement in disease activity ACR50: 50% improvement in disease activity Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
..")
58
REFERENCES 1)Aletaha D et al. Arthritis Rheum. 2010; 62 (9): 2569-81. 2)Fleischmann R et al. New Engl J Med. 2012; 367 (6): 495-507. 3)Lee EB et al. New Engl J Med. 2014; 370 (25): 2377-86. 4)LexiComp Online. online.lexi.com. 5)McInnes IB and Schett G. New Engl J Med. 2011; 365 (23): 2205-19. 6)O’Dell JR. New Engl J Med. 2004; 350 (25): 2591-602. 7)Pfizer Laboratories, Inc. Xeljanz (tofacitinib) Package Insert. 8)Saag KG et al. Arthritis Rheum. 2008; 59 (6): 762-84. 9)Singh JA et al. Arthrit Care Res. 2012; 64 (5): 625-39. 10)Vollenhoven RF. Nat Rev Rheumatol. 2009; 5 (10): 531-41. 11)Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014).
Fleischmann R et al. New Engl J Med. 2012; 367 (6): )Lee EB et al. New Engl J Med. 2014; 370 (25): )LexiComp Online. online.lexi.com. 5)McInnes IB and Schett G. New Engl J Med. 2011; 365 (23): )O’Dell JR. New Engl J Med. 2004; 350 (25): )Pfizer Laboratories, Inc. Xeljanz (tofacitinib) Package Insert. 8)Saag KG et al. Arthritis Rheum. 2008; 59 (6): )Singh JA et al. Arthrit Care Res. 2012; 64 (5): )Vollenhoven RF. Nat Rev Rheumatol. 2009; 5 (10): )Wahl K and Schuna AA. Chap 72. Rheumatoid Arthritis. In: Pharmacotherapy: A Pathophysiologic Approach. 9th ed. (2014)..")
59
RHEUMATOID ARTHRITIS melanie.laine@uky.edu

Similar presentations

 Immunomodulatory and immunosuppresive Xenobiotic – Gold salts – Azathioprine – Methotrexate Biological.>")



 25 th Nov 2013.>")

, an Interleukin-6 receptor antagonist, for the treatment of rheumatoid arthritis in Methotrexate Refractory patients.>")










 Slow Acting Anti-inflammatory Drugs.>")
