Download presentation
Presentation is loading. Please wait.

1
DIABETES INSTITUTE JOURNAL CLUB CARINA SIGNORI, D.O., M.P.H. DECEMBER 15, 2011 Atherothrombosis intervention in metabolic syndrome with low HDL/High Triglycerides: Impact on Global Health Outcomes

2
Introduction LDL and HDL → Risk of coronary artery disease (CAD) Elevated LDL has been found to be a predictor for risk of CAD. Low HDL is also an independent predictor for risk of CAD. Statin therapy lowers LDL and has been shown to reduce cardiovascular (CV) events (25-35%). HDL seems to have a prognostic value independent of LDL levels → when LDL lowered to <70, those with HDL in the highest quintile had 25% decrease in CV events compared to those with lowest quintile (Treating To New Targets trial). AIM-HIGH trial tested whether extended release (ER) niacin plus intensive statin therapy (vs statin alone) reduced risk of CV events in patients with atherosclerotic CV disease and dyslipidemia. Age ≥ 45 yo plus established CAD, cerebrovascular, carotid, PA disease = ↓ HDL, ↑ TG, ↑ small dense LDL
 events (25-35%). HDL seems to have a prognostic value independent of LDL levels → when LDL lowered to <70, those with HDL in the highest quintile had 25% decrease in CV events compared to those with lowest quintile (Treating To New Targets trial). AIM-HIGH trial tested whether extended release (ER) niacin plus intensive statin therapy (vs statin alone) reduced risk of CV events in patients with atherosclerotic CV disease and dyslipidemia. Age ≥ 45 yo plus established CAD, cerebrovascular, carotid, PA disease = ↓ HDL, ↑ TG, ↑ small dense LDL.")
3
Methods Patients were recruited at 92 clinical centers in U.S. and Canada. Eligible patients 1 st entered a 4-8 week open-label phase: Received simvastatin 40mg daily plus ER niacin at doses that were escalated weekly (500mg to 2000mg daily). Those who could tolerate niacin 1500mg daily were randomly assigned to niacin or matching placebo. Groups: Placebo = 50mg immediate release niacin (in each 500 or 1000 mg tablet) Niacin group = ER niacin 1500-2000 mg/d plus simvastatin (dose adjusted to achieve LDL 40-80 mg/dL). Each group could receive zetia 10mg/d to achieve target LDL.
. Those who could tolerate niacin 1500mg daily were randomly assigned to niacin or matching placebo. Groups: Placebo = 50mg immediate release niacin (in each 500 or 1000 mg tablet) Niacin group = ER niacin mg/d plus simvastatin (dose adjusted to achieve LDL mg/dL). Each group could receive zetia 10mg/d to achieve target LDL..")
4
8162 screened Eligible, enrolled and began open label phase N=4273 Up titrate weekly niaspan by 500mg Tolerated ≥ 1500mg niaspan (randomized 1:1) N=3414 Niaspan + simvastatin N= 1718 Placebo + simvastatin N= 1606 Did not tolerate niaspan: Flushing N=304 Pruritus N=253 Other N=374
 N=3414 Niaspan + simvastatin N= 1718 Placebo + simvastatin N= 1606 Did not tolerate niaspan: Flushing N=304 Pruritus N=253 Other N=374")
5
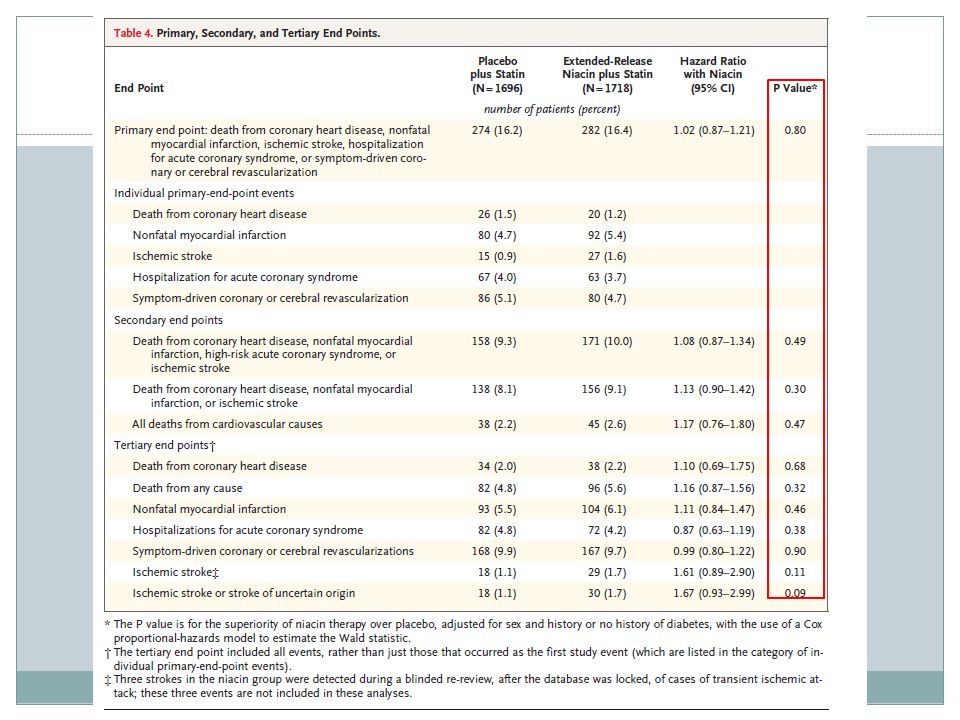
End Points Primary End Point: Composite of the 1 st event of: Death from CAD, nonfatal MI, CVA, hospitalization for ACS or symptom-driven coronary or cerebral revascularization. Secondary composite end points: Death from CAD, nonfatal MI, CVA or hospitalization for a high risk ACS, death from cardiac cause. Tertiary end points: Death from any cause, individual components of the primary end point and prespecified subgroups according to sex, history of diabetes or presence of metabolic syndrome.

6
Subject Demographics

7
Results At 2 years, HDL increased by 25% in niacin group, and 9.8% in placebo (P<0.001). TG decreased 28.6% in niacin group and 8.1% in placebo (P<0.001). LDL decreased 12.0% in niacin group and 5.5% in placebo group.
. LDL decreased 12.0% in niacin group and 5.5% in placebo group..")
9
Primary Endpoint Primary endpoint occurred in 282 patients in niacin group (16.4%) and 274 in the placebo group (16.2%) (hazard ratio with niacin, 1.02;95% CI 0.87-1.21;P=0.80). There was a nonsignificant trend in niacin group to have higher rates of CVA compared to placebo (29 patients vs 18 patients; hazard ratio, 1.61; 5% CI, 0.89-2.9;P=0.11).
..")
11
Discussion The study population was patients with established nonacute CVD and low baseline levels of HDL who achieved LDL <70 mg/dL with intensive statin treatment. In this group, extended release niacin plus simvastatin versus simvastatin alone: Decreased TG and increased HDL. However had no significant reduction on primary composite end point of CV events.

12
Previous studies of niacin have shown benefits in surrogate outcome measures (carotid intima media thickness and regression of angiographic coronary artery stenosis) and clinical outcomes. Limitations: Niacin at a low dose was given with placebo. Subjects had lower LDLs than prior niacin studies had achieved which may have impacted results. The niacin group had higher rates of stroke but no prior study has shown this with niacin. This finding will be studied further by the authors.

13
Questions

Similar presentations


>")






 The LIPID Study Group N Engl J Med 1998;339:1349-57.>")



>")



 Trial MEGA Trial Presented at The American Heart Association.>")

 Trial Overview Large international randomized controlled trial in patients with.>")
 The Lancet, Vol 344, November 19, 1994.>")