Download presentation
Presentation is loading. Please wait.

1
UNIVERSITY OF KERBALA COLLEGE OF MEDICINE Department of Pharmacology Immunosuppressant Drugs Dr. Haidar Al-Muthaffar MBChB, MSc, PhD Head of Pharmacology Department

2
INTRODUCTION The immune system is important in protecting the body against invading pathogens. However, in some instances, this protection can result in serious problems. For example, the immune response can cause rejection of transplanted tissues. Suppression of immune system can results in serious adverse effects (most important is increased liability of infections e.g. opportunistic infections) Old drugs were nonselective, and patients frequently had infection.
 Old drugs were nonselective, and patients frequently had infection..")
3
INTRODUCTION Today, the principal approach to immunosuppressive therapy is to alter lymphocyte function using drugs or antibodies against immune proteins preventing the serious adverse effects. Because of their severe toxicities, a combination of immunosuppressive agents, usually at lower doses, is generally employed.

4
CLASSIFICATION OF ISD 1.Selective inhibitors of cytokine production and function 2.Immunosuppressive antimetabolites 3.Monoclonal antibodies 4.Corticosteroids

5
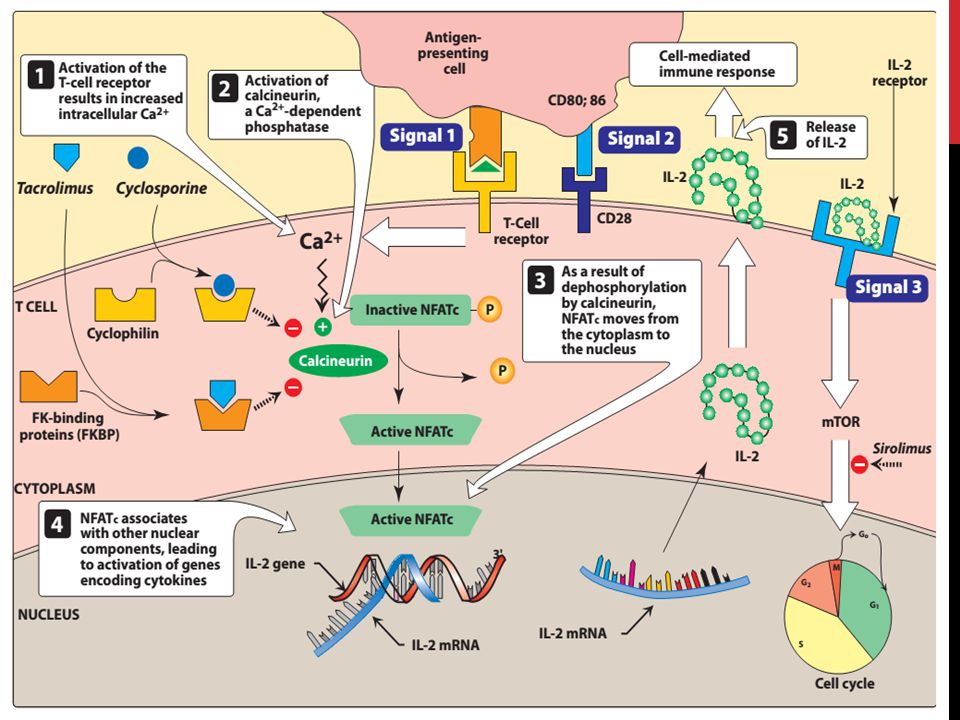
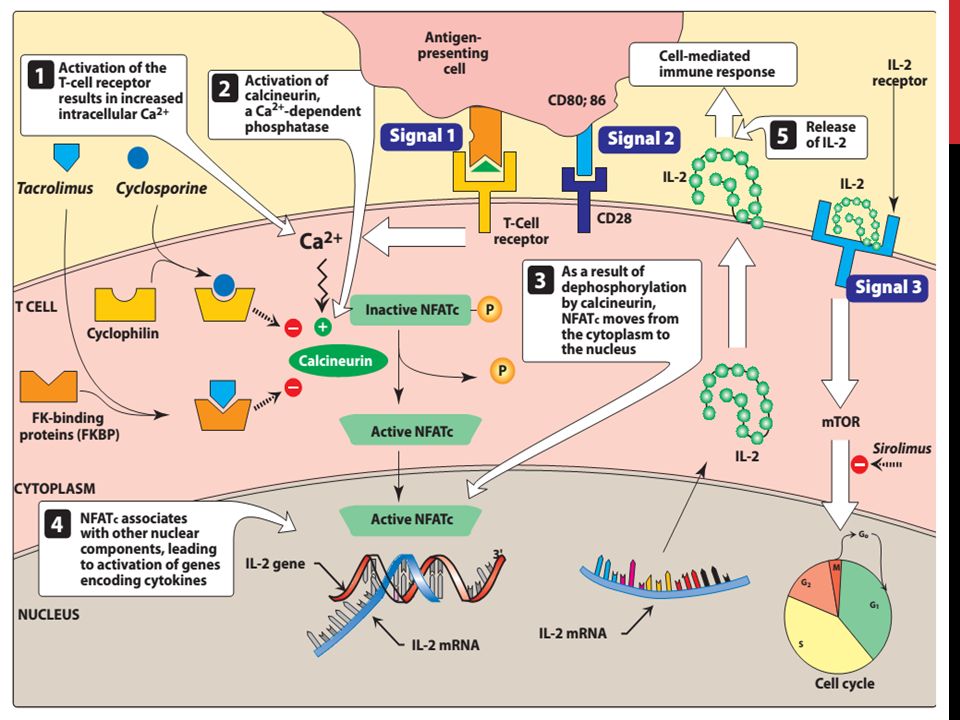
Selective inhibitors of cytokine production and function Cytokines are soluble signaling proteins that bind to cell surface receptors on a variety of cells. Cytokines include interleukins (ILs), interferons (IFNs), tumor necrosis factors (TNFs), transforming growth factors, and colony-stimulating factors. IL-2 stimulates the proliferation of T-helper cells, which subsequently produce more IL-2, IFN-γ, and TNF-α that activate NK cells, macrophages, and cytotoxic T lymphocytes. Drugs that interfere with the production or activity of IL-2, such as cyclosporine, will significantly suppress the immune response.
, interferons (IFNs), tumor necrosis factors (TNFs), transforming growth factors, and colony-stimulating factors. IL-2 stimulates the proliferation of T-helper cells, which subsequently produce more IL-2, IFN-γ, and TNF-α that activate NK cells, macrophages, and cytotoxic T lymphocytes. Drugs that interfere with the production or activity of IL-2, such as cyclosporine, will significantly suppress the immune response..")
6
CYCLOSPORINE Polypeptide (of 11 aa) extracted from the a soil fungus. Clinical use: To prevent rejection of kidney, liver, and cardiac transplants (mostly effective in preventing acute rejection of transplanted organs when combined with corticosteroids and an antimetabolite such as mycophenolate mofetil) It is alternative to methotrexate for the treatment of severe, active rheumatoid arthritis. Treatment of patients with psoriasis that does not respond to other therapies. It is also used for xerophthalmia.
 It is alternative to methotrexate for the treatment of severe, active rheumatoid arthritis. Treatment of patients with psoriasis that does not respond to other therapies. It is also used for xerophthalmia..")
7
CYCLOSPORINE Mechanism of action: It suppresses cell-mediated immune reactions, whereas humoral immunity is less affected. It inhibit the synthesis of IL-2 cytokine, by the following mechanism: After diffusing into the T cell, cyclosporine binds to a cyclophilin (called immunophilin) to form a complex that binds to calcineurin. Calcineurin is responsible for dephosphorylating (activating) cytosolic NFATc (Nuclear Factor of Activated T-cells). The cyclosporine-immunophilin-calcineurin complex cannot activate the NFATc which subsequently cannot enter the nucleus to promote the synthesis of a number of cytokines, including IL-2. The end result is a decrease in IL-2, which is the primary chemical stimulus for T lymphocytes proliferation.
 to form a complex that binds to calcineurin. Calcineurin is responsible for dephosphorylating (activating) cytosolic NFATc (Nuclear Factor of Activated T-cells). The cyclosporine-immunophilin-calcineurin complex cannot activate the NFATc which subsequently cannot enter the nucleus to promote the synthesis of a number of cytokines, including IL-2. The end result is a decrease in IL-2, which is the primary chemical stimulus for T lymphocytes proliferation..")
9
CYCLOSPORINE Pharmacokinetics: Cyclosporine may be given orally or by i.v. infusion. Oral absorption is variable due to variability in metabolism by cytochrome P450 (CYP3A4) in the GIT. Also cyclosporine is a substrate for P-glycoprotein (a drug efflux pump) which limits cyclosporine absorption by transporting it back into the gut lumen. Due to Interpatient absorption variability, cyclosporine plasma level should monitored for each patient. Cyclosporine is extensively metabolized, primarily by hepatic CYP3A4 (inhibitors or inducers of this enzyme can significantly alter plasma levels) Excretion of metabolites is through the bile, with only a small fraction of the parent drug appearing in urine.
 in the GIT. Also cyclosporine is a substrate for P-glycoprotein (a drug efflux pump) which limits cyclosporine absorption by transporting it back into the gut lumen. Due to Interpatient absorption variability, cyclosporine plasma level should monitored for each patient. Cyclosporine is extensively metabolized, primarily by hepatic CYP3A4 (inhibitors or inducers of this enzyme can significantly alter plasma levels) Excretion of metabolites is through the bile, with only a small fraction of the parent drug appearing in urine..")
10
CYCLOSPORINE Adverse effects: Many adverse effects are dose dependent. 1- Nephrotoxicity: is the most common and important side effect. Dose reduction, can result in reversal of nephrotoxicity in most cases, although it may be irreversible in 15 % of patients. Co-administration of nephrotoxic drugs (like, aminoglycoside antibiotics & NSAIDs) can increase nephrotoxicity. 2- Hepatotoxicity: (Less common than nephrotoxicity)
 can increase nephrotoxicity. 2- Hepatotoxicity: (Less common than nephrotoxicity).")
11
CYCLOSPORINE Adverse effects: 3- Infections are common and may be life-threatening. Viral infections due to the herpes group and CMV are prevalent. 4- Lymphoma may occur in all transplanted patients. 5- Anaphylactic reactions can occur on parenteral administration. 6- Other SE include hypertension, hyperlipidemia, hyperkalemia, tremor, hirsutism, glucose intolerance, and gum hyperplasia.

12
TACROLIMUS It is a macrolide (originally called FK-506) isolated from a soil fungus. Clinical use: 1- Prevention of rejection of liver and kidney transplants: It is usually given with a corticosteroid and/or an antimetabolite. It is superior to cyclosporine because of its higher potency, decreased episodes of rejection and lower doses of corticosteroids can be used (reducing the steroid-associated adverse effects). 2- A topical preparation has been approved for moderate-severe atopic dermatitis that does not respond to conventional therapies.
. 2- A topical preparation has been approved for moderate-severe atopic dermatitis that does not respond to conventional therapies..")
13
TACROLIMUS Mechanism of action: Tacrolimus exerts its immunosuppressive effect in the same manner as cyclosporine, except that it binds to a different cyclophilin called FKBP (FK-binding protein)
")
15
TACROLIMUS Pharmacokinetics: Tacrolimus may be administered orally or i.v. Tacrolimus is from 10-100 fold more potent than cyclosporine. The drug is metabolized by the liver CYP3A4/5 iso-enzyme, and the same drug interactions (as cyclosporine) can occur. Renal excretion is very low, and most of the drug and its metabolites are excreted with bile.
 can occur. Renal excretion is very low, and most of the drug and its metabolites are excreted with bile..")
16
TACROLIMUS Adverse effects: 1- Nephrotoxicity and neurotoxicity (tremor, seizures, and hallucinations) are more severe than those produced by cyclosporine, but dose adjustment can minimize this problem. 2- Post-transplant, insulin-dependent DM 3- Other SE are the same as those for cyclosporine, except that tacrolimus does not cause hirsutism or gingival hyperplasia and both hypertension and hyperlipidemia are less.

17
SIROLIMUS It is a macrolide (originally called rapamycin) obtained from fermentations of a soil fungus. Clinical use: 1- Renal transplantation (used together with cyclosporine and corticosteroids). The combination of sirolimus and cyclosporine is synergistic. 2- In cardiology, sirolimus-coated stents inserted into the cardiac vasculature inhibit restenosis of the blood vessels by reducing proliferation of the endothelial cells.
. The combination of sirolimus and cyclosporine is synergistic. 2- In cardiology, sirolimus-coated stents inserted into the cardiac vasculature inhibit restenosis of the blood vessels by reducing proliferation of the endothelial cells..")
18
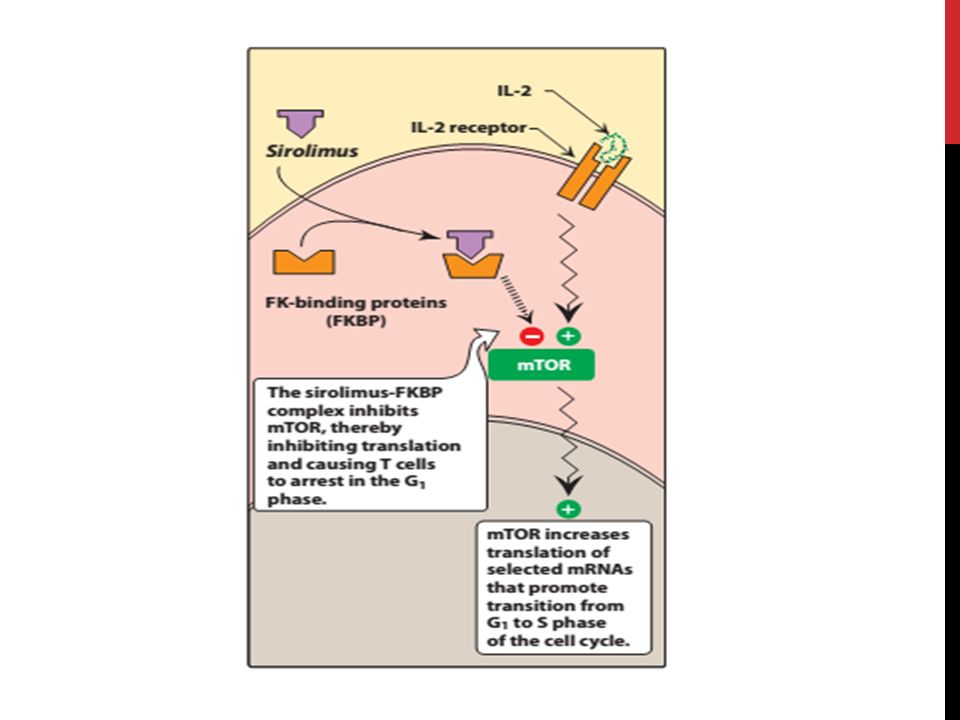
SIROLIMUS Mechanism of action: Sirolimus and tacrolimus bind to the same cytoplasmic FK- binding protein, but instead of forming a complex with calcineurin, sirolimus binds to mTOR (mammalian target of rapamycin), interfering with Signal 3. Binding of sirolimus to mTOR blocks the progression of activated T cells from the G1 to the S phase of the cell cycle and, consequently, the proliferation of these cells. Unlike cyclosporine and tacrolimus, sirolimus does not affect IL-2 production but, rather, inhibit the cellular responses to IL-2.

20
CELL CYCLE

21
SIROLIMUS Pharmacokinetics: The drug is available only as oral preparations. Sirolimus has a long half-life (57 to 62 hours) allowing once daily dosing. Like both cyclosporine and tacrolimus, sirolimus is metabolized by the CYP3A4 iso-enzyme and interacts with the same drugs as do cyclosporine and tacrolimus.
 allowing once daily dosing. Like both cyclosporine and tacrolimus, sirolimus is metabolized by the CYP3A4 iso-enzyme and interacts with the same drugs as do cyclosporine and tacrolimus..")
22
SIROLIMUS Adverse effects: 1- hyperlipidemia (elevated cholesterol and triglycerides) is common side effect of sirolimus which can require treatment. 2- The combination of cyclosporine and sirolimus is more nephrotoxic than cyclosporine alone. 3- Other untoward problems are headache, nausea & diarrhea, leukopenia, and thrombocytopenia. 4- Impaired wound healing has been noted with sirolimus in obese patients and those with diabetes.

23
EVEROLIMUS Recently approved by FDA for use in renal transplantation in combination with cyclosporine and corticosteroids. It was originally approved for treatment of advanced renal cell carcinoma. It has the same mechanism of action of sirolimus. Everolimus has similar side effects to sirolimus, including hyperlipidemia, impaired or delayed wound healing following transplantation, and enhanced nephrotoxicity in combination with higher doses of cyclosporine. An additional adverse effect noted is angioedema

24
Immunosuppressive Antimetabolites Immunosuppressive antimetabolite agents are generally used in combination with corticosteroids and the calcineurin inhibitors, cyclosporine and tacrolimus.

25
AZATHIOPRINE It is a prodrug that is converted to 6-mercaptopurine (6- MP) and then to the corresponding nucleotide, thioinosinic acid. The immunosuppressive effects of azathioprine are due to this nucleotide analog. Lymphocytes are affected by the cytotoxic effects of azathioprine because of their rapid proliferation in the immune response and their dependence on the de novo synthesis of purines required for cell division, Its major toxicity is bone marrow suppression in addition to nausea & vomiting Allopurinol, an agent used to treat gout, significantly inhibits the metabolism of azathioprine (dose reduction is required).
..")
26
MYCOPHENOLATE MOFETIL Mycophenolate mofetil has replaced azathioprine because of its safety and efficacy. It has been successfully used in heart, kidney, and liver transplants. The drug is rapidly hydrolyzed in the GIT to mycophenolic acid which is a potent inhibitor of inosine monophosphate dehydrogenase, that blocks the de novo formation of guanosine phosphate. Thus, like 6-MP, it deprives the rapidly proliferating T and B cells of a key component of nucleic acids. The most common adverse effects include diarrhea, nausea, vomiting, abdominal pain (enteric coated MPM has less effects), leukopenia, and anemia. Higher doses of mycophenolate mofetil were associated with a higher risk of CMV infection
, leukopenia, and anemia. Higher doses of mycophenolate mofetil were associated with a higher risk of CMV infection.")
27
Mechanism of action of Mycophenolate mofetil

28
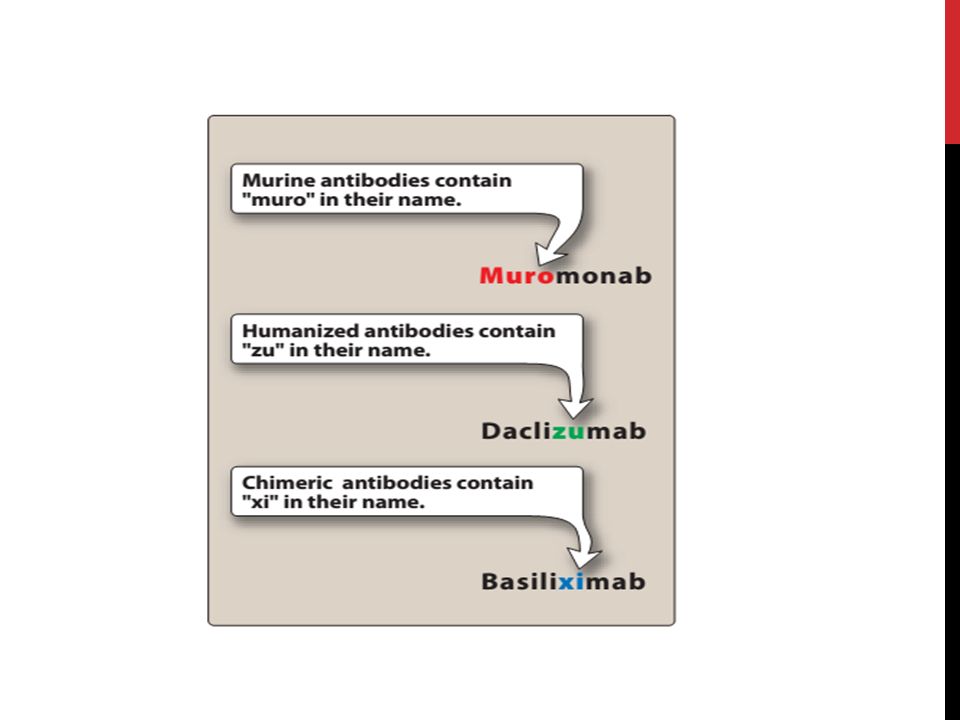
MONOCLONAL ANTIBODIES Drugs developed by hybridoma technology (Hybridomas are produced by fusing mouse antibody-producing cells with, malignant plasma cells) Recombinant DNA technology is used to replace part of the mouse gene sequence with human genetic material, thus “humanizing” the antibodies produced, making them less antigenic. The names of monoclonal antibodies conventionally contain “muro” if they are from a murine (mouse) source “xi” if they are chimerized (mixed murine and human) or “zu” if they are humanized. The suffix “mab” (monoclonal antibody) identifies the category of the drug So monoclonal antibodies are biological drugs produced against specific antigens (drug targets)
 source xi if they are chimerized (mixed murine and human) or zu if they are humanized. The suffix mab (monoclonal antibody) identifies the category of the drug So monoclonal antibodies are biological drugs produced against specific antigens (drug targets).")
30
MUROMONAB Murine monoclonal antibody that is synthesized by hybridoma technology and directed against the glycoprotein CD3 antigen of human T cells. It is used i.v. for treatment of acute rejection of renal, cardiac, and hepatic transplant patients. Binding of muromonab to the CD3 protein results in a disruption of T-lymphocyte function, because access of antigen to the recognition site is blocked. T cells usually return to normal within 48 hours of discontinuation of therapy. Adverse effects: o Anaphylactoid reactions o Cytokine release syndrome follow the first dose o Infections

31
IL-2-RECEPTOR ANTAGONISTS Basiliximab & Daclizumab Both compounds are anti-CD25 antibodies and bind to the α chain of the IL-2 receptor on activated T cells. They thus interfere with the proliferation of these cells. Both drugs approved for prophylaxis of acute rejection in renal transplantation. Basiliximab is about 10-fold more potent than daclizumab as a blocker of IL-2 stimulated T-cell replication. Both antibodies are given IV. The serum half-life of daclizumab is about 20 days (7 days for basiliximab). The major SE of both drugs is on the GIT
. The major SE of both drugs is on the GIT.")
32
ALEMTUZUMAB humanized monoclonal antibody directed against CD52, exerts its effects by causing profound depletion of T-cells from the peripheral circulation. This effect may last for up to 1 year. Alemtuzumab is currently approved for the treatment of chronic lymphocytic leukemia (CLL). Adverse effects include neutropenia, anemia, and, rarely, pancytopenia.
. Adverse effects include neutropenia, anemia, and, rarely, pancytopenia..")
33
CORTICOSTEROIDS The corticosteroids were the first pharmacological agents to be used as immunosuppressive both in transplantation and in various autoimmune disorders. Most common agents are methylprednisolone, prednisone and prednisolone they bind to the glucocorticoid receptor and rapidly reduce lymphocyte populations They are effective against a wide variety of autoimmune conditions, including refractory rheumatoid arthritis, SLE, temporal arthritis, and asthma. The use of these agents is associated with numerous adverse effects. For example, they are diabetogenic and can cause hypercholesterolemia, cataracts, osteoporosis, and hypertension with prolonged use.

34
THANK YOU

Similar presentations




 Adjuvants (nonspecific.>")



>")


 Slow Acting Anti-inflammatory Drugs.>")







 Dr. Kaukab Azim.>")