Download presentation
Presentation is loading. Please wait.

1
Pharma Team Immunosuppressants Prof. Alhaider, 1432 H Definition
Clinical Uses (Organ transplants & Autoimmune diseases) Pre-requisite to understand immunosuppressive drugs (Basic immunology). Review of immune system (read Table 56-1, next slide) Cell mediated vs humoral immunity Importance of cytokines Immunophilins Calcineurin Pharma Team
 Pre-requisite to understand immunosuppressive drugs (Basic immunology). Review of immune system (read Table 56-1, next slide) Cell mediated vs humoral immunity. Importance of cytokines. Immunophilins. Calcineurin. Pharma Team.")
4
MOA: next slide

6
Classification of Immunosuppressant (Based on Mechanism of Action)
A) Antiprolifirative Agents I) Drugs Acting on Immunophilins: (most importanat ) a) Selective Inhibitors of Cytokine production (Calcineurin Inhibitors) e.g: Cyclosporine; Tacrolimus b) Inhibitor of cytokine function (e.g. Sirolimus). II) Antimetabolites (Azathioprine; Mycophenolate Mofetil) III ) Alkylating Agents (Cyclophosphamide) B) Lymphocyte Depleting Agents: Corticosteroids (Prednisone (orall) & Methylprednisolone (IV) ) Immunosuppressive Antibodies a) Polyclonal Antibodies (Antilymphocytic Globulins) b) Monoclonal Antibodies (Selective inhibitors of IL2 (Basiliximab; Daclizumab)
 Antiprolifirative Agents. I) Drugs Acting on Immunophilins: (most importanat ) a) Selective Inhibitors of Cytokine production (Calcineurin Inhibitors) e.g: Cyclosporine; Tacrolimus. b) Inhibitor of cytokine function (e.g. Sirolimus). II) Antimetabolites (Azathioprine; Mycophenolate Mofetil) III ) Alkylating Agents (Cyclophosphamide) B) Lymphocyte Depleting Agents: Corticosteroids (Prednisone (orall) & Methylprednisolone (IV) ) Immunosuppressive Antibodies. a) Polyclonal Antibodies (Antilymphocytic Globulins) b) Monoclonal Antibodies (Selective inhibitors of IL2 (Basiliximab; Daclizumab)")
8
Immunosuppressant Classes
Non-selective Corticosteroids Prednisone (PO) & Methylprednisolone (IV) Antimetabolite (DNA synthesis inhibitors) Azathioprine & Myclophenolate mofetil Immunoglobulins Anti-lymphocyte antibodies Selective Calcineurin Inhibitors Cyclosporine Tacrolimus (Rapamycin) Selective IL-2 Receptor antagonists Basiliximab, Daclizumab & Infliximab Mamalian target of Rapamycin (mTOR) inhibitors Sirolimus
 & Methylprednisolone (IV) Antimetabolite (DNA synthesis inhibitors) Azathioprine & Myclophenolate mofetil. Immunoglobulins. Anti-lymphocyte antibodies. Selective. Calcineurin Inhibitors. Cyclosporine. Tacrolimus (Rapamycin) Selective IL-2 Receptor antagonists. Basiliximab, Daclizumab & Infliximab. Mamalian target of Rapamycin (mTOR) inhibitors. Sirolimus.")
10
1) Cyclosporine (CsA) (Cyclic peptide from Soil Fungus (1971)
Selective Inhibitors of Cytokine Production (Drugs Acting on Immunophilins) 1) Cyclosporine (CsA) (Cyclic peptide from Soil Fungus (1971) MOA: (See slide 5) CsA binds to cyclophillin forming a comlex Bind to Calcineurin dephosphorylation NFATc * Synthesis of IL cell-mediated immune response (proliferation of T cells) Thus, decreases the level of IL-2, the primary chemical stimulus for increasing the number of T lymphocytes. Note: Suppress only cell-mediated immunity with no effect on B lymphocytes/humoral immunity. *NFATc = cytosolic nuclear factor of activated T cells
 1) Cyclosporine (CsA) (Cyclic peptide from Soil Fungus (1971) MOA: (See slide 5) CsA binds to cyclophillin forming a comlex Bind to Calcineurin dephosphorylation NFATc * Synthesis of IL-2 cell-mediated immune response (proliferation of T cells) Thus, decreases the level of IL-2, the primary chemical stimulus for increasing the number of T lymphocytes. Note: Suppress only cell-mediated immunity with no effect on B lymphocytes/humoral immunity. *NFATc = cytosolic nuclear factor of activated T cells.")
11
PK CsA available as oral (capsule) or parentral (i.v)
Oral bioavailability (20-50%), It undergoes extensive hepatic metabolism by Cyt P450 (CYP3A4) (Affected by drugs affecting the microenzymes cimetidine, rifampin, cefaporazone) Mainly excreted in the bile.
, It undergoes extensive hepatic metabolism by Cyt P450 (CYP3A4) (Affected by drugs affecting the microenzymes cimetidine, rifampin, cefaporazone) Mainly excreted in the bile.")
12
Clinical Uses of Cyclosporine:
1) Drug of choice for preventing organ transplant rejection in combination with steroids and other immunosuppressants. 2) Severe active rheumatoid arthritis, as an alternative for methotrexate 3) Lower doses (7.5 mg/kg/d) for autoimmune diseases (Uveitis; RA; early Rx of DM 1) 3) Psoriasis and asthma ? Not used anymore
 Drug of choice for preventing organ transplant rejection in combination with steroids and other immunosuppressants. 2) Severe active rheumatoid arthritis, as an alternative for methotrexate. 3) Lower doses (7.5 mg/kg/d) for autoimmune diseases (Uveitis; RA; early Rx of DM 1) 3) Psoriasis and asthma Not used anymore.")
13
Side Effects (remember: most immunosuppressant are very toxic)
Dose-dependent nephrotoxicity ( Risk of Rejection); enhanced when given with other nephrotoxic drugs (Aminoglycosides; NSIADs, amphotericin B) Hepatotoxicity Neurotoxicity as tremor and hallucination Infection, opportunistic Lymphoma and cancer How? immunity Hypertension; hyperlipidemia; Hyperkalemia; DM; osteoporosis, hirsutism, and gum hyperplasia (So What? don’t prescribe it to female patints)
; enhanced when given with other nephrotoxic drugs (Aminoglycosides; NSIADs, amphotericin B) Hepatotoxicity. Neurotoxicity as tremor and hallucination. Infection, opportunistic. Lymphoma and cancer How immunity. Hypertension; hyperlipidemia; Hyperkalemia; DM; osteoporosis, hirsutism, and gum hyperplasia (So What don’t prescribe it to female patints)")
14
2. Tacrolimus (FK 506): More potent than Cyclosporine
MOA: Similar to Cyclosporine (Calcineurin Antagonist) but it bind to a different immunophilin (FKBP) slide 14 PK: Almost Similar to Cyclosporine Side Effects: differ from Cyclosporine, that it has no hirsutism or gum hyperplasia but may show more hyperglycemia than cyclosporine. Note: It is like cyclosporine, could lead to nephrotoxicity and hyperglycemia (more hyperglycemia than cyclosporine) , and hyperlipidemia.
 but it bind to a different immunophilin (FKBP) slide 14. PK: Almost Similar to Cyclosporine. Side Effects: differ from Cyclosporine, that it has no hirsutism or gum hyperplasia but may show more hyperglycemia than cyclosporine. Note: It is like cyclosporine, could lead to nephrotoxicity and hyperglycemia (more hyperglycemia than cyclosporine) , and hyperlipidemia.")
16
Preferred over CsA for:
Clinical uses of Tacrolimus: Preferred over CsA for: Its greater potency ( times more potent than cyclosporine) lower rejection episodes lower doses of glucocorticoids are used with lower side effects Better first choice for women, can you tell why? Less hirsutism and gum hyperplasia Severe refractory atopic dermatitis, local application of an ointment An ointment for psoriasis.
 lower rejection episodes. lower doses of glucocorticoids are used with lower side effects. Better first choice for women, can you tell why Less hirsutism and gum hyperplasia. Severe refractory atopic dermatitis, local application of an ointment. An ointment for psoriasis.")
17
Five year renal allograft survival in patients with cyclosporin or tacrolimus

18
3. Sirolimus (Rapamycin Macrolides)
MOA: see next slide 1) Binds to the same immunophilin Tacrolimus binds to but does not form a complex with calcineurin. Instead, it binds to mTOR (Mammalian Target of Rapamycin) which is essential for many cellular functions (See Figure 40.6) 2) Sirolimus does not affect IL-2 production, unlike CsA & Tac, rather inhibits T-cells response to IL-2 (Blocks cytokine-stimulated cell proliferation) 3) Potent inhibitor of B-cell proliferation and immunoglobulin production (decreases the humoral immunity)
 Binds to the same immunophilin Tacrolimus binds to but does not form a complex with calcineurin. Instead, it binds to mTOR (Mammalian Target of Rapamycin) which is essential for many cellular functions (See Figure 40.6) 2) Sirolimus does not affect IL-2 production, unlike CsA & Tac, rather inhibits T-cells response to IL-2 (Blocks cytokine-stimulated cell proliferation) 3) Potent inhibitor of B-cell proliferation and immunoglobulin production (decreases the humoral immunity)")
20
Uses of Sirolimus: Side Effects:
1) can be used together with cyclosporine to increases the activity of cyclosporine for organ transplantion. Why not tacrolimus? Because it shares the same MOA. 2) As replacement of cyclosporine if transplanted patient developed cancer of skin or lips. 3) Used in cardiac catheter stint to prevent stenosis?? 4) As an ointment for atopic dermatitis and psoriasis Side Effects: 1) Pneumonitis 2) Hyperlipidemia (even more than calcineurin- antagonists)
 can be used together with cyclosporine to increases the activity of cyclosporine for organ transplantion. Why not tacrolimus Because it shares the same MOA. 2) As replacement of cyclosporine if transplanted patient developed cancer of skin or lips. 3) Used in cardiac catheter stint to prevent stenosis 4) As an ointment for atopic dermatitis and psoriasis. Side Effects: 1) Pneumonitis. 2) Hyperlipidemia (even more than calcineurin- antagonists)")
21
Antiproliferatives (Continue…) 2. Antimetabolites (Cytotoxic Drugs)
1) Azathioprine: is a prodrug of mercaptopurine. Cytotoxic, rarely used as chemotherapeutic drug, but commonly used for immunosuppression. It is a prodrug, converted in the body to the active metabolite, 6-mercaptopurine and thioinosinic acid. MOA: (see next slide Figure) It inhibits purine synthesis (antimetabolite), thus interfering with nucleic acid metabolism of leukocytes and lymphocytes leading to the inhibition of proliferation. Why it is considered as cytotoxic agent? Because the purine analog of Azathioprine can destroy lymphoids cells. Why is it very important to know the structure of azathioprine?.
 Azathioprine: is a prodrug of mercaptopurine. Cytotoxic, rarely used as chemotherapeutic drug, but commonly used for immunosuppression. It is a prodrug, converted in the body to the active metabolite, 6-mercaptopurine and thioinosinic acid. MOA: (see next slide Figure) It inhibits purine synthesis (antimetabolite), thus interfering with nucleic acid metabolism of leukocytes and lymphocytes leading to the inhibition of proliferation. Why it is considered as cytotoxic agent Because the purine analog of Azathioprine can destroy lymphoids cells. Why is it very important to know the structure of azathioprine .")
22
Metabolic pathway for azathioprine
6-thiouracil (-) Xanthine Allopurinol Oxidase Nonenzymatic HPRT AZA MP thioiosinic acid thioguanine (TIMP) ( 6-TG) TPMT TPMT 6-MMP MMP ribonucleides
 Xanthine Allopurinol. Oxidase. Nonenzymatic HPRT. AZA 6-MP thioiosinic acid 6-thioguanine. (TIMP) ( 6-TG) TPMT TPMT. 6-MMP 6-MMP. ribonucleides.")
23
Cliniclal Uses of Azathioprine (ImuranR)
1) Maintenance of renal allograft and other transplants together with steroids and cyclosporine. 2) Can be used for glomerulonephtitis and SLE; RA; Crohn’s disease and multiple sclerosis (MS). PK:It can be given both orally and IV Side Effects: 1) Like cyclosporine, is not teratogenic (Unlike TAC and Siro) but carcinogenic if given together with alkylating agents. Here, higher doses are used for immunosuppression as compared to its use in autoimmune diseases. 2) Strong bone marrow suppression (Leukopenia; anemia; thrombocytopenia How? 3) Hepatic dysfunction as increase ALP and mild jaundice. 4) Hypersensitivity reactions (as rashes, fever, diarrhea) Why?.
 Maintenance of renal allograft and other transplants together with steroids and cyclosporine. 2) Can be used for glomerulonephtitis and SLE; RA; Crohn’s disease and multiple sclerosis (MS). PK:It can be given both orally and IV. Side Effects: 1) Like cyclosporine, is not teratogenic (Unlike TAC and Siro) but carcinogenic if given together with alkylating agents. Here, higher doses are used for immunosuppression as compared to its use in autoimmune diseases. 2) Strong bone marrow suppression (Leukopenia; anemia; thrombocytopenia How 3) Hepatic dysfunction as increase ALP and mild jaundice. 4) Hypersensitivity reactions (as rashes, fever, diarrhea) Why .")
24
Drug interactions: Combination with ACEIs or cotrimoxazole can cause severe leukopenia in renal transplants

25
2) Mycophenolate Mofetil (CellceptR)
The most important discovery among the immunosuppressant agents. MOA: (See Figure in the coming 2nd slide) Mycophenolic acid acts as non-competitive, selective 7 reversible inhibitor of inosine monophosphate dehydrogenase (IMD) Decreases GMP, which is a key enzyme in the de novo pathway of purine synthesis. This leads to suppression of both B and T lymphocyte activation. PK: Good oral absorption; Side Effects: Less than azathioprine, Reversible bone marrow suppresion (leukopenia and anemia); N/V and diarrhea (decresed by Enteric-coated form). Unlike azathioprine it is teratogenic.
 Mycophenolic acid acts as non-competitive, selective 7 reversible inhibitor of inosine monophosphate dehydrogenase (IMD) Decreases GMP, which is a key enzyme in the de novo pathway of purine synthesis. This leads to suppression of both B and T lymphocyte activation. PK: Good oral absorption; Side Effects: Less than azathioprine, Reversible bone marrow suppresion (leukopenia and anemia); N/V and diarrhea (decresed by Enteric-coated form). Unlike azathioprine it is teratogenic.")
26
Note: in renal or liver transplant, patients may take the followings:
Clinical Uses 1) Drug of choice for preventing vasculopathy in cardiac transplants 2)As a replacement for the more cytotoxic drug, azathioprine in renal allograft patients as well as liver, heart et act. Why? As replacement of azathioprine or cyclophosphamide for autoimmune diseases (RA, SLE (especially before lupus nephritis); Glomerulonephritis Has good oral bioavailability Note: in renal or liver transplant, patients may take the followings: Corticosteriods as prednisolone (Low dose) + cyclosporine or Tac + Mycophenolate Mofetil
 Drug of choice for preventing vasculopathy in cardiac transplants. 2)As a replacement for the more cytotoxic drug, azathioprine in renal allograft patients as well as liver, heart et act. Why As replacement of azathioprine or cyclophosphamide for autoimmune diseases (RA, SLE (especially before lupus nephritis); Glomerulonephritis. Has good oral bioavailability. Note: in renal or liver transplant, patients may take the followings: Corticosteriods as prednisolone (Low dose) + cyclosporine or Tac + Mycophenolate Mofetil.")
28
3. Lefunomide: - A Prodrug of an inhibitor of PYRIMIDINE synthesis rather than purine-like azathioprine and mycophenolate mofetil. Orally active used only for RA Side effects: Alopecia; raised LFT, nephrotoxicity, teratogenicity.

29
3. Alkylating Agents e.g. Cyclophosphamide
The most potent immunosuppressant Destroys proliferating lymphoid cells (cytotoxic agent) also alkylates some resting cellsvery toxic Clinical Uses: Before the discovery of Mycophenolate, cyclophosphamide was the drug of choice for treatment of many autoimmune diseases like: SLE, autoimmune hemolytic diseases, and RA. Side Effects: Pancytopenia Hemorrhagic cystitis a unique Adverse effect Infertility Teratogenic
 also alkylates some resting cellsvery toxic. Clinical Uses: Before the discovery of Mycophenolate, cyclophosphamide was the drug of choice for treatment of many autoimmune diseases like: SLE, autoimmune hemolytic diseases, and RA. Side Effects: Pancytopenia. Hemorrhagic cystitis a unique Adverse effect. Infertility. Teratogenic.")
30
B) Lymphocyte Depleting Agents:
1. Corticosteroids: The most commonly used immunosuppressant MOA: At the biochemical level: act on gene expression, which leads to decrease synthesis of PGs; Leukotrienes, cytokines, and other signaling molecules which participate in the immune response. At the cellular level: they inhibit the proliferation of T lymphocytes (cell mediated) and slightly dampen humoral immunity (by increasing the catabolism of immunoglobulins). At immunosuppressive doses, Corticosteroids are cytotoxic and continuous uses causes lowering of IgGs.
 and slightly dampen humoral immunity (by increasing the catabolism of immunoglobulins). At immunosuppressive doses, Corticosteroids are cytotoxic and continuous uses causes lowering of IgGs.")
31
Uses: In combination with other immunossppressants for transplanted patients (To prepare the patients as well as maintenance). To treat acute rejection episodes (high doses) To treat undesirable immunoreactions (to drugs or asthma). For autoimmune diseases (idiopathic thrompocytopenic purpura; inflammatory bowel diease; rheumatoid arthritis; systemic lupus erythematosus; and glomerulonephritis)
 To treat undesirable immunoreactions (to drugs or asthma). For autoimmune diseases (idiopathic thrompocytopenic purpura; inflammatory bowel diease; rheumatoid arthritis; systemic lupus erythematosus; and glomerulonephritis)")
32
Adverse effects: Increased blood pressure How? By their aldostrone-like moiety hyperglycemia due to increased gluconeogenesis, insulin resistance, and impaired glucose tolerance ("steroid diabetes"); Osteoporosis Visceral and truncal fat deposition (central obesity) and appetite stimulation Weight gain (water & salt retention) How? Answered above! Muscle breakdown (proteolysis), weakness; reduced muscle mass and repair Increased skin fragility, easy bruising Cataracts Adrenal cortex suppression (Avoid abrupt withdrawl) Increase tendency to infections
; Osteoporosis. Visceral and truncal fat deposition (central obesity) and appetite stimulation. Weight gain (water & salt retention) How Answered above! Muscle breakdown (proteolysis), weakness; reduced muscle mass and repair. Increased skin fragility, easy bruising. Cataracts. Adrenal cortex suppression (Avoid abrupt withdrawl) Increase tendency to infections.")
33
2. Immunosuppressive Antibodies
a) Polyclonal Antibodies (Antilymphocyte Globulins) Definition: Thymocytes are considered as T-cell precursors. What are the differences between polyclonal and monoclonal antibodies? 1) Antithymocyte (Antilymphocyte) Globulins (ALG): this antisera can be obtained by immunization of large animals (e.g.rabbits) with human lymphoid cells. MOA: Antibodies bind to the surface of circulating T lymphocytes forming a comlex. This complex will be phagocytosed in the liver or spleen leading to destruction or inactivation of T cells. ALG mainly affects the cellular immunity with no effect on humoral, resulting in antibodies against these foreign proteins.
 Polyclonal Antibodies (Antilymphocyte Globulins) Definition: Thymocytes are considered as T-cell precursors. What are the differences between polyclonal and monoclonal antibodies 1) Antithymocyte (Antilymphocyte) Globulins (ALG): this antisera can be obtained by immunization of large animals (e.g.rabbits) with human lymphoid cells. MOA: Antibodies bind to the surface of circulating T lymphocytes forming a comlex. This complex will be phagocytosed in the liver or spleen leading to destruction or inactivation of T cells. ALG mainly affects the cellular immunity with no effect on humoral, resulting in antibodies against these foreign proteins.")
34
PK: Administered by IM or slow IV infusion with long half-life of: 3-9 days
Side Effects: 1) Mainly result from the introduction of foreign proteins obtained from heterogeneous serum (Anaphylactic and serum sickness reactions; Local pain and erythema at the site of injection). 2) Chills & fever and Leukopenia & thrombocytopenia 3) Viral infections and skin rashes 4) Lymphoma and cancer
 Mainly result from the introduction of foreign proteins obtained from heterogeneous serum (Anaphylactic and serum sickness reactions; Local pain and erythema at the site of injection). 2) Chills & fever and Leukopenia & thrombocytopenia. 3) Viral infections and skin rashes. 4) Lymphoma and cancer.")
35
Polyclonal Antibodies (continue…)
Clinical Uses of ALG: 1) Rx of hyperacute phase of allograft rejection 2) To prepare the patient undergoing bone marrow translpant (Give large doses of ALG for 7 days) 2) Immune globulin Intravenous (IGIV): - Prepared from a pool of thousands of healthy donors. Uses: 1) Refractory Idipathic Thrombocutopenic Purpura Advantages: Has no antigenicity
 Rx of hyperacute phase of allograft rejection. 2) To prepare the patient undergoing bone marrow. translpant (Give large doses of ALG for 7 days) 2) Immune globulin Intravenous (IGIV): - Prepared from a pool of thousands of healthy donors. Uses: 1) Refractory Idipathic Thrombocutopenic Purpura. Advantages: Has no antigenicity.")
36
1) Muromonab-CD3 (IL-2-antagonist):
B) Monoclonal Antibodies (Muromonab; Basiliximab; Abciximab; Daclizumab. 1) Muromonab-CD3 (IL-2-antagonist): From its name, it is murine monoclonal antibody prepared by hybridoma technology and directed against the glycoprotien CD3 antigen of human T cells. Used mainly for cases of acute allograft rejections of the kidney, heart, and liver. It is also used to deplete T cells from donor bone marrow before transplantation. Advantage over ALG: More specific and T lymphocytes return to normal within 24 hours. Side Effects: 1) Cytokine release syndrome (Anaphylactoid reactions); and seizure (contraindication) Therefore, it is less used nowadays.
 Monoclonal Antibodies (Muromonab; Basiliximab; Abciximab; Daclizumab. 1) Muromonab-CD3 (IL-2-antagonist): From its name, it is murine monoclonal antibody prepared by hybridoma technology and directed against the glycoprotien CD3 antigen of human T cells. Used mainly for cases of acute allograft rejections of the kidney, heart, and liver. It is also used to deplete T cells from donor bone marrow before transplantation. Advantage over ALG: More specific and T lymphocytes return to normal within 24 hours. Side Effects: 1) Cytokine release syndrome (Anaphylactoid reactions); and seizure (contraindication) Therefore, it is less used nowadays.")
37
Side Effect of Muromonab
Its use has been declined much because of multiple side effects and the emergence of newer and more selective antibodies therapy Anaphylaxis may occur Cytokine release syndrome, flu-like to dangerous shock-like reactions can occur, & high fever CNS: Seizures, encephalopathy, cerebral edema & headache Infection like CMV Contraindicated with pregnancy, breast feeding, history of seizures, uncompensated heart failure

38
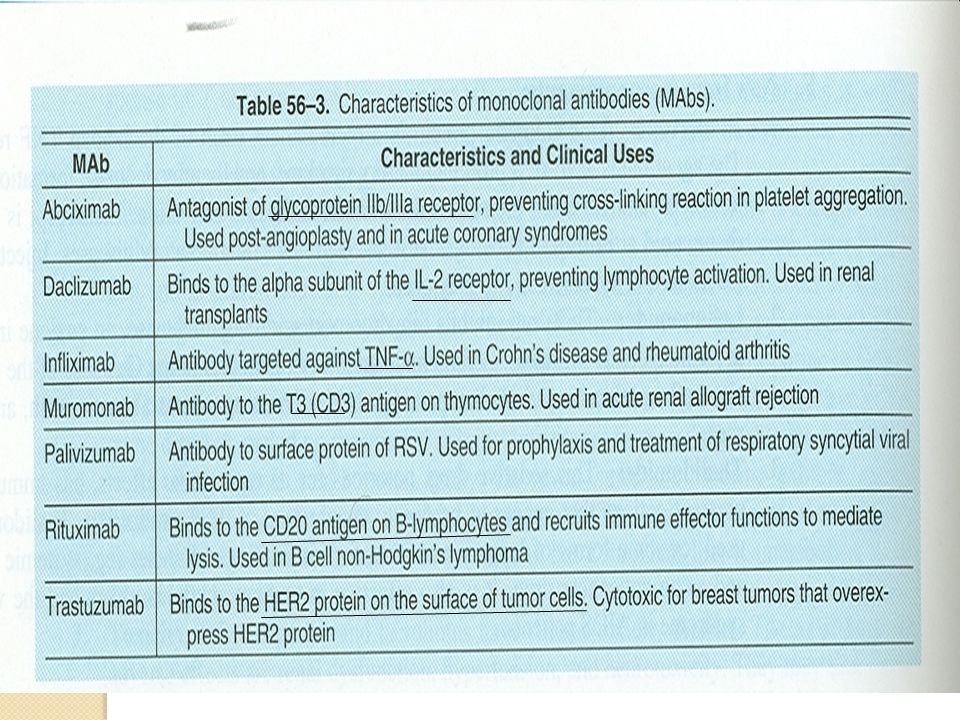
2) Modified Types of monoclonal antibodies (e
2) Modified Types of monoclonal antibodies (e.g: Selective Inhibitors of IL-2): Note: Monoclonal Antibodies are not limited for immunosuppression but could be utilized for other purposes (See Table 56-3) By using the genetic engineering, most murine amino acids of Muromonab have been replaced by human a.a.; producing humanized designated monoclonal antibodies (e.g. Daclizumab; Transtuzumab). While the chimeric (Mixed) antibodies contain XI in their name (e.g. Abciximab; Infliximab; Rutuximab). Clinical Uses: See Table 56-3 Advantages over polyclonal antibodies Are less immunoantigenic.
 Modified Types of monoclonal antibodies (e.g: Selective Inhibitors of IL-2): Note: Monoclonal Antibodies are not limited for immunosuppression but could be utilized for other purposes (See Table 56-3) By using the genetic engineering, most murine amino acids of Muromonab have been replaced by human a.a.; producing humanized designated monoclonal antibodies (e.g. Daclizumab; Transtuzumab). While the chimeric (Mixed) antibodies contain XI in their name (e.g. Abciximab; Infliximab; Rutuximab). Clinical Uses: See Table Advantages over polyclonal antibodies Are less immunoantigenic.")
41
B- Selective IL-2 Receptor Antagonists Basiliximab & Daclizumab
Basiliximab is a chimeric antibody composed of 25% murine & 75% human protein. Blocks IL-2 of activated lymphocytes Daclizumab is humanized antibody composed of 90% human protein Therapeutic Use: Prophylaxis against acute rejection of kidney transplantation Used in combination with steroids and CsA

42
Selective IL-2 Receptor Antagonists Basiliximab & Daclizumab (Continue…)
Mechanism of action: They are anti-CD25 and IL-2 antibodies They bind to the -chain of the IL-2 R (CD25 or TAC subunit) on the activated T-cells Then, IL-2 binding to IL-2R is prohibited & T-cell activation and proliferation are suppressed
 on the activated T-cells. Then, IL-2 binding to IL-2R is prohibited & T-cell activation and proliferation are suppressed.")
43
Pharmacokinetics: Given by IV route
VI- Selective IL-2 Receptor Antagonists Basiliximab & Daclizumab (Continue...) Pharmacokinetics: Given by IV route Daclizumab has serum half-life of 20 days & receptor blockade for 120 days Administered in 5 doses; the first 24 hours before transplantation and next 4 doses at 14- days intervals Basiliximab has serum half-life of 7 days Administered in two doses; the first at 2-hours before transplantation & the second at 4 days after surgery
 Pharmacokinetics: Given by IV route. Daclizumab has serum half-life of 20 days & receptor blockade for 120 days. Administered in 5 doses; the first 24 hours before transplantation and next 4 doses at 14- days intervals. Basiliximab has serum half-life of 7 days. Administered in two doses; the first at 2-hours before transplantation & the second at 4 days after surgery.")
44
Both are well-tolerated Gastrointestinal toxicity is the major one
Selective IL-2 Receptor Antagonists Contiue..)) Basiliximab & Daclizumab Adverse Effects: Both are well-tolerated Gastrointestinal toxicity is the major one NO antibodies, of clinical relevance, to the antibodies are produced Infection & malignancy were not reported
) Basiliximab & Daclizumab. Adverse Effects: Both are well-tolerated. Gastrointestinal toxicity is the major one. NO antibodies, of clinical relevance, to the antibodies are produced. Infection & malignancy were not reported.")
45
Alemtuzumab: Humanized monoclonal antibody directed against CD-52, and produces profound depletion of T cells. Used for refractory B-cell chronic lymphocytic leukemia. However, it is currently used in organ transplantation.

47
3- RhoD Immunoglobulin Rho(D) Immune Globulin (Rhogam)
Rhogam is an immunoglobulin that recognizes the Rho(D) antigen Prepared from pooled sera from Rho-negative volunteers immunized with D+ erythrocytes It prevents erythroblastosis fetalis (hemolytic disease of the newborn) When a Rho(D)-negative mother carries a Rho(D)- positive fetus, the mother becomes sensitized Subsequent pregnancies can strengthen response increasing chance of Ab transfer to the fetus in the last trimester
 antigen. Prepared from pooled sera from Rho-negative volunteers immunized with D+ erythrocytes. It prevents erythroblastosis fetalis (hemolytic disease of the newborn) When a Rho(D)-negative mother carries a Rho(D)- positive fetus, the mother becomes sensitized. Subsequent pregnancies can strengthen response increasing chance of Ab transfer to the fetus in the last trimester.")
48
How Does Rho(immunoglobulin work)
The potion is a solution of IgG anti-D (anti- RhD) antibodies that bind to, and lead to the destruction of, fetal Rh D positive red blood cells that have passed from the fetal circulation to the maternal circulation. Therefore, Rho in a Rhesus negative mother it can prevent sensitization of the maternal immune system to Rh D antigens, which can cause rhesus disease in the current or in subsequent pregnancies. Note: With the widespread use of Rho (D) Immune Globulin, Rh disease of the fetus and newborn has almost disappeared.
 antibodies that bind to, and lead to the destruction of, fetal Rh D positive red blood cells that have passed from the fetal circulation to the maternal circulation. Therefore, Rho in a Rhesus negative mother it can prevent sensitization of the maternal immune system to Rh D antigens, which can cause rhesus disease in the current or in subsequent pregnancies. Note: With the widespread use of Rho (D) Immune Globulin, Rh disease of the fetus and newborn has almost disappeared.")
49
RhoD Immunoglobulin It is usually given to the mother within 72 hours after the birth of any of the Rh- positive babies she has. This would prevent hemolytic anemia that may occur in subsequent pregnancies Adverse Effects: Chills Fever Anaphylaxis (rare)
")
Similar presentations















 Adjuvants (nonspecific.>")




>")





 Dr. Kaukab Azim.>")

