Download presentation
Presentation is loading. Please wait.

1
ECZEMA Dr. Sharon Crichlow Consultant Dermatologist Luton and Dunstable NHS Foundation Trust 22/02/2011

2
Definition Controversial but loosely thought to be synonymous with the term ‘dermatitis’. Strictly speaking dermatitis is inflammation of the skin (any cause).
..")
3
Classification Endogenous –Atopic –Seborrheic –Discoid (nummular) –Pompholyx –Gravitational (venous stasis) –Asteatotic –Neurodermatitis
 –Pompholyx –Gravitational (venous stasis) –Asteatotic –Neurodermatitis")
4
Classification Mainly exogenous –Irritant dermatitis –Allergic contact dermatitis –Photodermatitis

5
Atopic dermatitis- key features Chronic relapsing dermatitis associated with intense pruritus Can occur at any age but 70-95% of cases arise before the age of 5 years Typically infantile, childhood and adulthood; periods of acquiescence can occur between stages Aetiology and pathogenesis is still not fully elucidated Often associated with atopy Genetic basis with variable expression influenced by environmental factors

6
Immuno-aberration is evidenced by the common occurrence of serum IgE elevation and eosinophilia; the Th2 predominance in acute lesions evolves into a predominance of IFN gamma producing T-cells in chronic lesions. There is enhanced reactivity to irritants, self-proteins, allergens and infectious antigens and superantigens

11
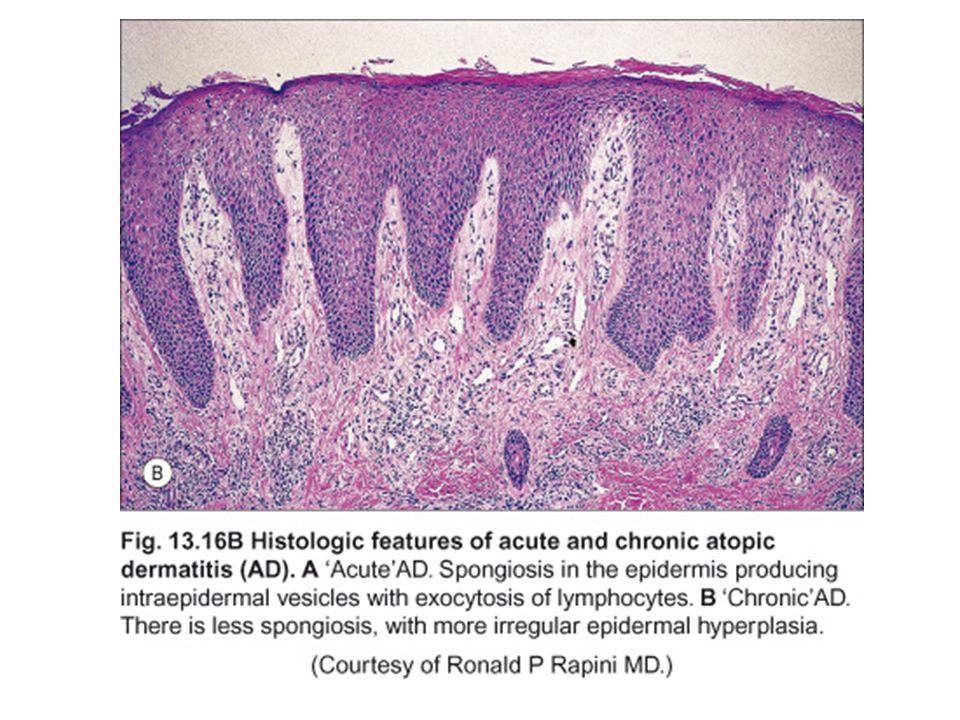
CLINICAL APPEARANCE Acute eczema- weeping and crusting blistering redness, papules and swelling- with an ill defined border scaling

12
Chronic eczema- May show all the above but Less vesicular and exudative More scaly, pigmented and thickened More likely to show lichenification More likely to fissure

13
ALL FORMS OF ECZEMA ARE ASSOCIATED WITH INTENSE PRURITUS IF IT DOES NOT ITCH IT’S PROBABLY NOT ECZEMA!!

15
DIFFERENTIAL DIAGNOSIS SCABIES FUNGAL INFECTION

16
INVESTIGATIONS USUALLY CLINICAL DIAGNOSIS PATCH TESTING- if ACD suspected SERUM TOTAL AND SPECIFIC IgE SWABS FOR STAPH AND CANDIDA MICROSCOPIC EXAMINATION OF SCALES AND FUNGAL CULTURE TO RULE OUT OTHER DIAGNOSES.

17
Infantile eczema

23
TREATMENT Acute weeping eczema- –Soaks with potassium permanganate. –Wet wrap dressings and/ or bandages such as icthopaste, viscopaste –Topical steroids and emollients –Tacrolimus/ pimecrolimus

24
Chronic eczema- –Steroids in an ointment base –Emollients –Systemic or topical antibiotics –Ichthammol and zinc pastes –Anti-histamines and other anti-itch preparations

25
SYSTEMIC TREATMENTS Prednisolone Cyclosporine Azathiaprine Tacrolimus/sirolimus Mycophenolate mofetil

27
Pompholyx eczema

28
Palmar/ plantar eczema

30
Varicose eczema

31
Treatment Elevate legs when sitting or standing Emollients such as hydrommol oint Mild topical steroids such as Betnovate RD ointment or Eumovate ointment Check ABPIs If suitable then compression stockings, above knee during daytime

32
Discoid eczema

33
Juvenile plantar dermatosis

34
Occurs in pre-pubertal children from age 3 onwards, rare in adults Worse in winter, boys more than girls Associated with sports shoes with plastic or rubber soles The humid environment leads to maceration of the keratin layer, which is then rubbed off with friction leading to a glazed and thinned appearance of the skin.

35
The balls of the feet are tender and dry with a shiny appearance, at times scaly May develop cracks and fissures Chronic but self-limiting Avoid wearing impermeable socks and shoes Emollients and keratolytics may be helpful

36
Seborrheic dermatitis

37
Treatment Daktacort/ Canesten HC ointments Tacrolimus/ pimecrolimus

Similar presentations


























 * Incidence has trebled over the last 30 years (Harper.>")



>")
 Prevent insensible water.>")


 -Dyshidrotic.>")



 that are commonly seen in the early acute stage of the.>")