Download presentation
Presentation is loading. Please wait.

1
UNIVERSITY OF MISSOURI Family & Community Medicine UNIVERSITY OF MISSOURI Family & Community Medicine See One, Do One, Teach One? A More Thoughtful Approach to Procedural Training in Family Medicine

2
Presenters Peter Koopman, MD Assistant Professor of Clinical Family and Community Medicine University of Missouri School of Medicine-Columbia And Erik J. Lindbloom, MD, MSPH Associate Professor of Family and Community Medicine University of Missouri School of Medicine-Columbia

3
UNIVERSITY OF MISSOURI Family & Community Medicine See One.

4
UNIVERSITY OF MISSOURI Family & Community Medicine Do One.

5
UNIVERSITY OF MISSOURI Family & Community Medicine Teach One.

6
UNIVERSITY OF MISSOURI Family & Community Medicine Why Change? Personal Story. Residents consistently give feedback that they would like better procedural training. Procedural precepting is different from much of the precepting we do in that it is both manual and cognitive. We have tools for cognitive precepting (One minute preceptor)-Why not procedural?
-Why not procedural .")
7
UNIVERSITY OF MISSOURI Family & Community Medicine Resident A More Thoughtful Approach To Resident Procedural Teaching Not So Random ACTS of Teaching A-Assess C-Confirm T-Teach S-Stand Back and Summarize

8
UNIVERSITY OF MISSOURI Family & Community Medicine DIAGNOSEASSESS TREATTEACH A-Assess

9
UNIVERSITY OF MISSOURI Family & Community Medicine A-Assess Assess resident’s familiarity and comfort with particular procedure. Assess if resident has seen, done or taught. Assess resident’s approach to procedure.

10
UNIVERSITY OF MISSOURI Family & Community Medicine C-Confirm Confirmation of manual aspects of procedure in question. Confirm with book or video resources. Confirm what tools and supplies?

11
UNIVERSITY OF MISSOURI Family & Community Medicine Video Resources-Free YouTube: www.youtube.comwww.youtube.com YouTube Downloader: http://youtubedownload.altervista.org/ http://youtubedownload.altervista.org/ Mediclips: http://medclip.com/http://medclip.com/ Medical Videos: http://www.medicalvideos.us/ http://www.medicalvideos.us/

12
UNIVERSITY OF MISSOURI Family & Community Medicine Video Resources-Free

13
UNIVERSITY OF MISSOURI Family & Community Medicine Video Resources-Free

14
UNIVERSITY OF MISSOURI Family & Community Medicine Video Resources-Free

15
UNIVERSITY OF MISSOURI Family & Community Medicine Video Resources-Pay Sites New England Journal: http://www.nejm.org/multimedia/medic al-videos http://www.nejm.org/multimedia/medic al-videos Elsevier: http://www.clinicalanswer.com/procedu res/ http://www.clinicalanswer.com/procedu res/

16
UNIVERSITY OF MISSOURI Family & Community Medicine Video Resources-Pay Sites

17
UNIVERSITY OF MISSOURI Family & Community Medicine Book Resources

18
UNIVERSITY OF MISSOURI Family & Community Medicine T-Teach Teach from your experiences. Teach what you have found helpful-OK to be anecdotal. Teach practical tips.

19
Sample Slides: This Is NOT About Lumber Puncture

20
UNIVERSITY OF MISSOURI Family & Community Medicine Overview CT/MRI have decreased the need for LP, but have also increased the safety of the procedure Indications, contraindications Equipment, prep, technique Complications Labs Billing

21
UNIVERSITY OF MISSOURI Family & Community Medicine Indications: Suspected… CNS infection (meningitis, encephalitis) Subarachnoid hemorrhage Multiple Sclerosis Guillain-Barré Acute demyelinating disorders (e.g. trans- verse myelinitis, encephalomyelinitis) Systemic lupus erythematosus Meningeal carcinomatosis
 Systemic lupus erythematosus Meningeal carcinomatosis.")
22
UNIVERSITY OF MISSOURI Family & Community Medicine Indications: Also… Unexplained altered level of consciousness, polyneuropathy Symptomatic relief (pseudotumor cerebri, normal pressure hydrocephalus) Spinal analgesia Intrathecal antibiotics, chemotherapeutics Imaging (e.g. myelography, cisternography)
.")
23
UNIVERSITY OF MISSOURI Family & Community Medicine Contraindications Local skin infection (absolute contraindication) Evidence of increased intracranial pressure on imaging (OK for pseudotumor cerebri and NPH) Supratentorial mass lesions Severe bleeding diathesis, coagulopathy, or anticoagulated (relative contraindication)
 Evidence of increased intracranial pressure on imaging (OK for pseudotumor cerebri and NPH) Supratentorial mass lesions Severe bleeding diathesis, coagulopathy, or anticoagulated (relative contraindication)")
24
UNIVERSITY OF MISSOURI Family & Community Medicine Equipment Spinal tray, which should include: (Pass around while listing) Also good to have an extra spinal needle ready to go Sterile gloves
 Also good to have an extra spinal needle ready to go Sterile gloves")
25
UNIVERSITY OF MISSOURI Family & Community Medicine Prep Hey, did you get consent? Pretty sure it’s infection? Get the antibiotics going! To image or not to image? Well…

26
UNIVERSITY OF MISSOURI Family & Community Medicine “It’s a really fine line between stupid and clever.” David St. Hubbins Risk of cerebral herniation and sudden death from an LP with no imaging and focal neuro signs as high as 40%. Papilledema, no focal neuro signs: 5% Documented increased pressure (greater than 20 cm H2O), no focal signs: 1.2% What would be considered “focal”? Good question. Get the imaging.
, no focal signs: 1.2% What would be considered focal . Good question. Get the imaging..")
27
UNIVERSITY OF MISSOURI Family & Community Medicine Landmarks: Aiming for L3-L4

28
UNIVERSITY OF MISSOURI Family & Community Medicine Landmarks

29
UNIVERSITY OF MISSOURI Family & Community Medicine Why the L3-L4 Interspace?

30
UNIVERSITY OF MISSOURI Family & Community Medicine Positioning Edge of bed in lateral recumbent (preferred for pressure measurement) or sitting position Slight flex of neck anteriorly and “roll up into a ball” with knees drawn to abdomen Shoulders and pelvis vertical without tilt! Landmarks clear? Mark if necessary.

31
UNIVERSITY OF MISSOURI Family & Community Medicine Positioning Open the tray, put on the gloves Assemble your manometer and stopcock Open the tubes and set them upright Prepare the skin at 3(!) interspaces and drape
 interspaces and drape")
32
Positioning

33
UNIVERSITY OF MISSOURI Family & Community Medicine The Sharp Stuff Using small syringe and tiny needle, raise a wheal with lidocaine, and then aim deeper with small amount (may obscure landmarks – did you mark?) Using posterior spinous process and umbilicus as landmarks, insert the spinal needle angled approx 15% cephalad
 Using posterior spinous process and umbilicus as landmarks, insert the spinal needle angled approx 15% cephalad")
34
UNIVERSITY OF MISSOURI Family & Community Medicine The Sharp Stuff Keep needle level with sagittal midplane, bevel cephalad If you hit bone, stop, withdraw needle slightly, change angle Advance for 3-4 cm for average patient Withdraw stylus and check hub for fluid No fluid? Replace stylus, advance needle a bit, recheck

35
UNIVERSITY OF MISSOURI Family & Community Medicine The Sharp Stuff Ideally feel a “pop” as needle penetrates Advance another 1-2 mm farther before withdrawing stylus Rotating needle sometimes helps Radiating pain down leg? Dry tap? Blood not fading? Stop, withdraw, regroup, try a different interspace Bloody CSF from subarachnoid hem won’t clot

36
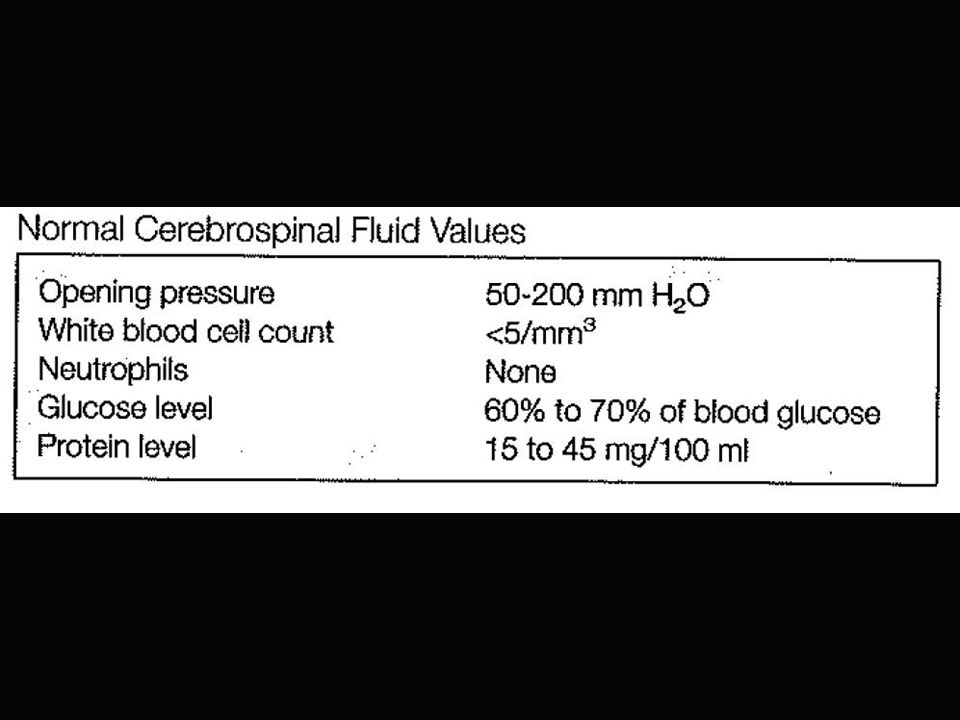
UNIVERSITY OF MISSOURI Family & Community Medicine Hooray! You have fluid dripping. Now what? Place stopcock with manometer onto needle hub Have patient relax position a bit Pressure can fluctuate a bit with pulse and respiration

37
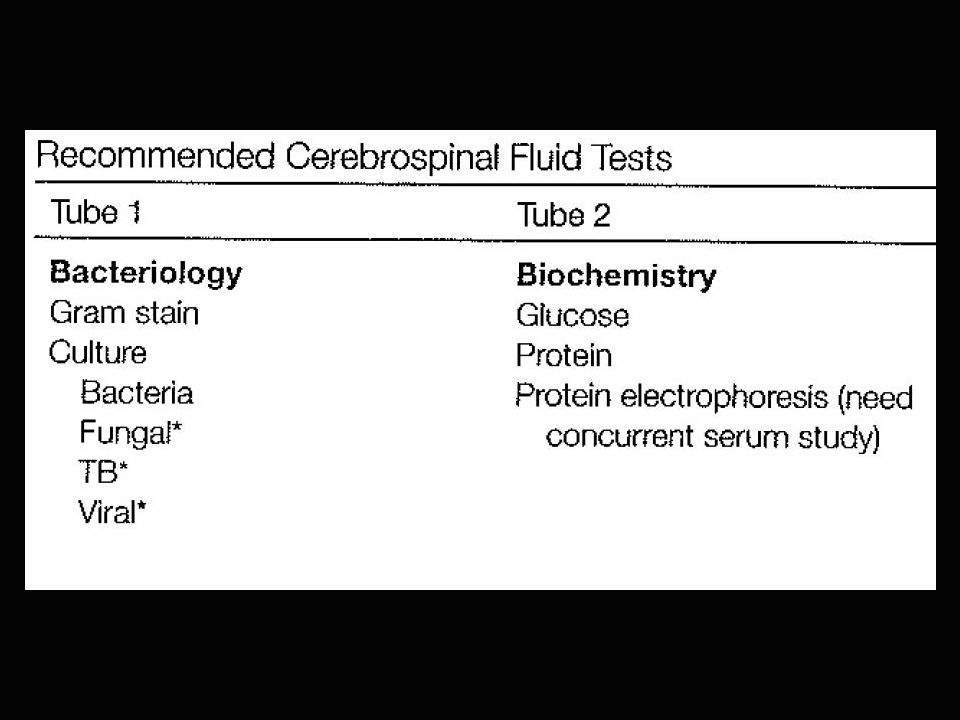
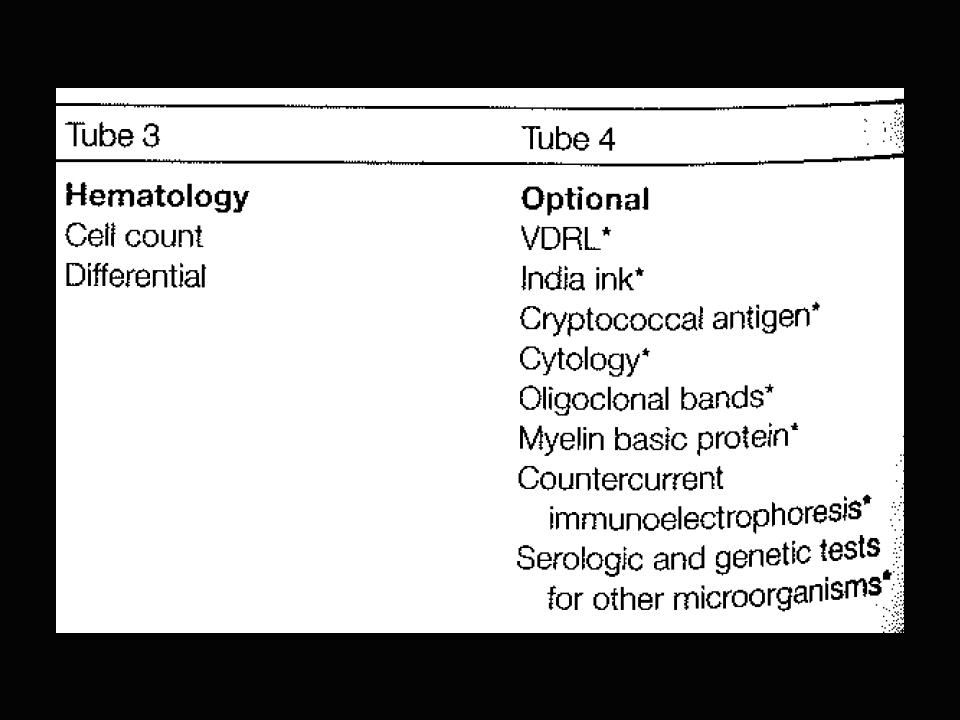
UNIVERSITY OF MISSOURI Family & Community Medicine Let it Flow Once opening pressure is noted, turn stopcock to allow flow to tubes 2-3 ml each of 3 tubes Fourth tube: specials or freezing Replace stylus, remove needle, cover site with dressing/Band-Aid, supine 2 hours(?)
")
38
UNIVERSITY OF MISSOURI Family & Community Medicine Or Really Let it Flow Therapeutic LP for pseudotumor: enough to reduce closing pressure to 10 cm H2O (usually 25-35 ml) Diagnostic LP for NPH: 35-50 ml with transient neuropsych improvement
 Diagnostic LP for NPH: ml with transient neuropsych improvement")
42
UNIVERSITY OF MISSOURI Family & Community Medicine Complications (…other than sudden death…) Post-LP headache in 10-25% Usually within 2 days, worse when sitting upright, self-resolves after a few days Can occur up to 12 days later, can last longer than a week and be debilitating Oral or IV caffeine (500mg) may help (x2) “Blood patch”: 15 ml of autologous blood into dural space; usual immediate relief. (Why?)
.")
43
UNIVERSITY OF MISSOURI Family & Community Medicine Complications (other than sudden death) Seizures Traumatic (“bloody”) tap: usually self- limited, but can lead to hematoma Meningitis Nerve root aspiration: remember to replace stylus when withdrawing needle Local pain Paresthesias: rarely chronic… but can be.
 Seizures Traumatic ( bloody ) tap: usually self- limited, but can lead to hematoma Meningitis Nerve root aspiration: remember to replace stylus when withdrawing needle Local pain Paresthesias: rarely chronic… but can be.")
44
UNIVERSITY OF MISSOURI Family & Community Medicine Peds Pearls It’s all in the hold Upright option: neonates/young infants Overflexion of neck can lead to resp arrest Topical anaesthetic with EMLA helps Less likely to feel “pop” Infants only need 1.5 inch needle Epidermoid tumors reported in neonatal period, after not using stylus

45
UNIVERSITY OF MISSOURI Family & Community Medicine Billing CPT: 62270 (spinal puncture, lumbar, diagnostic) 62272 (spinal puncture, therapeutic) ICD-9: 320.9 (322.9) Bacterial (suspected) meningitis 047.9 Aseptic meningitis 852.00 Subarachnoid hemorrhage 348.2 Pseudotumor cerebri 357.0 GBS 340 MS
 (spinal puncture, therapeutic) ICD-9: (322.9) Bacterial (suspected) meningitis Aseptic meningitis Subarachnoid hemorrhage Pseudotumor cerebri GBS 340 MS")
46
UNIVERSITY OF MISSOURI Family & Community Medicine Emphasis During Faculty Workshops(?) Indications, contraindications Technique pearls, perhaps “off book” Complications Labs Billing
 Indications, contraindications Technique pearls, perhaps off book Complications Labs Billing")
47
UNIVERSITY OF MISSOURI Family & Community Medicine S- Standback/Summarize Stand back –gloved-to provide support. Let resident do procedure unless assessment tells you otherwise. In hospital setting let senior resident teach and support their teaching Summarize procedure pluses and minuses at end and debrief. Give feedback.

48
UNIVERSITY OF MISSOURI Family & Community Medicine A Four Daughters Production

Similar presentations




 & Posterior.>")

, Dip.Diab. DCA, Dip. Software statistics PhD (physio) Mahatma Gandhi Medical college.>")



 中国医科大学护理学院 王健. Medications (three) PARENTERAL MEDICATIONS Nurses given parenteral medications intradermally (ID), subcutaneously (SC or SQ),>")








