Download presentation
Presentation is loading. Please wait.

1
Nosocomial Infections Emergence of Antimicrobial Resistance Mazen Kherallah, MD, FCCP King Faisal Specialist Hospital & Research Center

2
Impact of Antibiotic Restriction on Resistance Neurosurgical Intensive Care Unit in London 1968 1969 1970 All antibiotics stopped Price. Lancet. 1970

3
Rate of Device-Related Infections in ICU

4
Decrease in Hospital-acquired ICU Infection Rates, NNIS, 1990-1999

5
Possible Explanation for Decrease in Infection Rate Efforts to prevent infections: new research findings, prevention guidelines Shift of health care from hospital-based care True decrease secondary to adhesion to infection control policies

6
Antimicrobial Resistance: A Global Problem ICAAC 1998 Antimicrobial Resistance Symposium: 200 attendees Infectious disease physicians (25%), microbiologist (25%), other physicians, pharmacists, etc. (50%) 80% agreed that antimicrobal resistance is increasing70% believed resistant pathogens cause greater mortality
 80% agreed that antimicrobal resistance is increasing70% believed resistant pathogens cause greater mortality.")
7
Antimicrobial Resistance: A Global Problem

8
Rates of Resistance Among Nosocomial Infections Reported in Intensive Care Patients, Comparison of 1999 (January- July) with Historical Data January-July 1999 1993-1998
 with Historical Data January-July")
9
Percentage of Resistance KFSH&RC Jeddah

10
Emerging Pathogens Methicillin-resistant Staphylococcus aureus (MRSA) Methicillin-resistant Staphylococcus epidermitis (MRSE) Vancomycin-resistant enterococci (VRE) Vancomycin-intermediate Staphylococcus aureus (VISA) Extended-spectrum beta-lactamase (ESBL)- producing gram-negative organisms Multidrug-resistant Acinetobacter spp.
 Methicillin-resistant Staphylococcus epidermitis (MRSE) Vancomycin-resistant enterococci (VRE) Vancomycin-intermediate Staphylococcus aureus (VISA) Extended-spectrum beta-lactamase (ESBL)- producing gram-negative organisms Multidrug-resistant Acinetobacter spp.")
12
Percentage of Nosocomial Staphylococcus aureus Reported as Resistant to Methicillin, by year National Nosocomial Infections Surveillance (NNIS), 1989-1998: system Data
, : system Data")
13
Methicillin Resistant Staphylococci by setting Fridkin. Clin Infect Dis.1999

14
Secular Trend in MRSA Infections INSPEAR, 1990-1997 International Network for Surveillance and Prevention of Emerging Antimicrobial Resistance (INSPEAR)
")
15
Methicillin-Resistant Staphylococcus aureus: Current Status Endemic beginning 1980 in hospitals Increasing reports of community infections: –Pediatric outpatients in Chicago –Alaskan natives –4 Pediatric deaths: MMWR 1998

16
Epidemiology of VRE Present in all 50 states in the United States Number of isolated continues to grow Recognized in Europe, Japan, Central and South America Resistance to alternate antibiotic therapy continues to be a problem

17
Progression of Vancomycin Resistance Enterococci Mortone. WJ. Infect Control Hosp Epidemiol. 1998 NNIS Antimicrobial Resistance Surveillance Report 1999

18
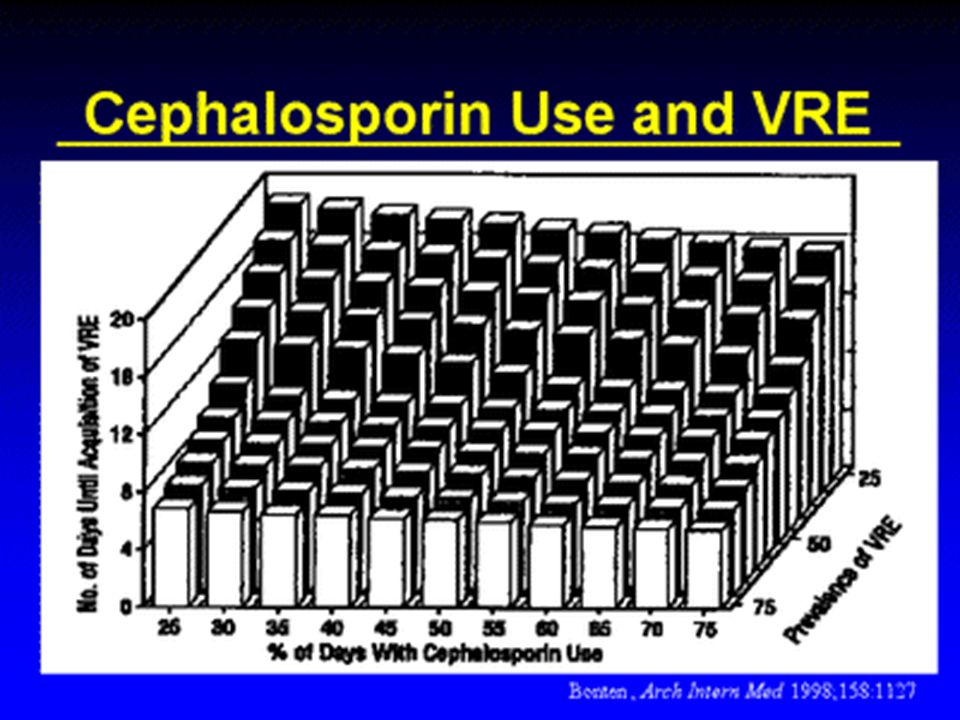
Risk Factors for VRE Prior broad spectrum antibiotics (especially cephalosporins and vancomycin) Prolonged hospitalization Immunocompromised host Neutropenia Admission to an intensive care unit Renal failure requiring dialysis Noskin. J Lab Clin Med. 1997

19
Antibiotics and Colonization with VRE Ostrowsky. Arch Intern Med. 1999

20
Use of Vancomycin in US and Rate of VRE Kirsl et al. Historical usage of vancomycin. Antimicrob Agent Chemo 1998 National Nosocomial Infection Surveillance System (CDC)
.")
21
Independent Predictors of Vancomycin-Resistant Enterococci in Adult Intensive Care Units NNIS

23
Enterococcal Resistance by Species Jones. Diagn. Microbiol Infect Dis. 1998

24
Outcome of Enterococcus faecium Bacteremia Stosor. Arch Intern Med. 1998

25
Impact of Formulary Change on VRE Empiric therapy for febrile neutropenia Lisgaris. IDSA (abstract). 2000
")
26
Bradley. JAC. 1999 Prevention of GRE Therapy for Febrile Neutropenia Purpose: reduce glycopeptide resistant enterococci (GRE) Situation: 50% colonization rate in oncology units Methods: –Phase 1: no intervention (ceftazidime) –Phase 2a and 2b: replace ceftazidime with piperacillin/tazobactam –Phase 3: return to ceftazidime
 Situation: 50% colonization rate in oncology units Methods: –Phase 1: no intervention (ceftazidime) –Phase 2a and 2b: replace ceftazidime with piperacillin/tazobactam –Phase 3: return to ceftazidime.")
27
Results Phase 1 vs 2b (P<0.001) Bradley. JAC. 1999
 Bradley. JAC. 1999")
28
Impact of CDC Guidelines on Endemic VRE M. Montecalvo et al. Ann Int Med. 1999 J Morris et al. Ann Int Med. 1995 E Jochimsen et al. ICHE 1999

29
Emergence of Vancmycin-Intermediate Staphylococcus aureus (VISA) in the World First episode reported in Japan, 1996 Predicted risk factors: –MRSA colonization/infection –Frequent/sustained vancomycin exposure Predicted high risk population –ESRD on hemodialysis –Long-term CVCs –Rehab/skilled nursing facility patients –Prolonged ICU stay
 in the World First episode reported in Japan, 1996 Predicted risk factors: –MRSA colonization/infection –Frequent/sustained vancomycin exposure Predicted high risk population –ESRD on hemodialysis –Long-term CVCs –Rehab/skilled nursing facility patients –Prolonged ICU stay")
30
Extended Spectrum -lactamases ESBLs 1983: first reported in Europe 1988:: reported in the United States 1990’s: increased prevalence globally: –ICU’s –Acute care –Extended care 2000: Problematic nosocomial pathogen

31
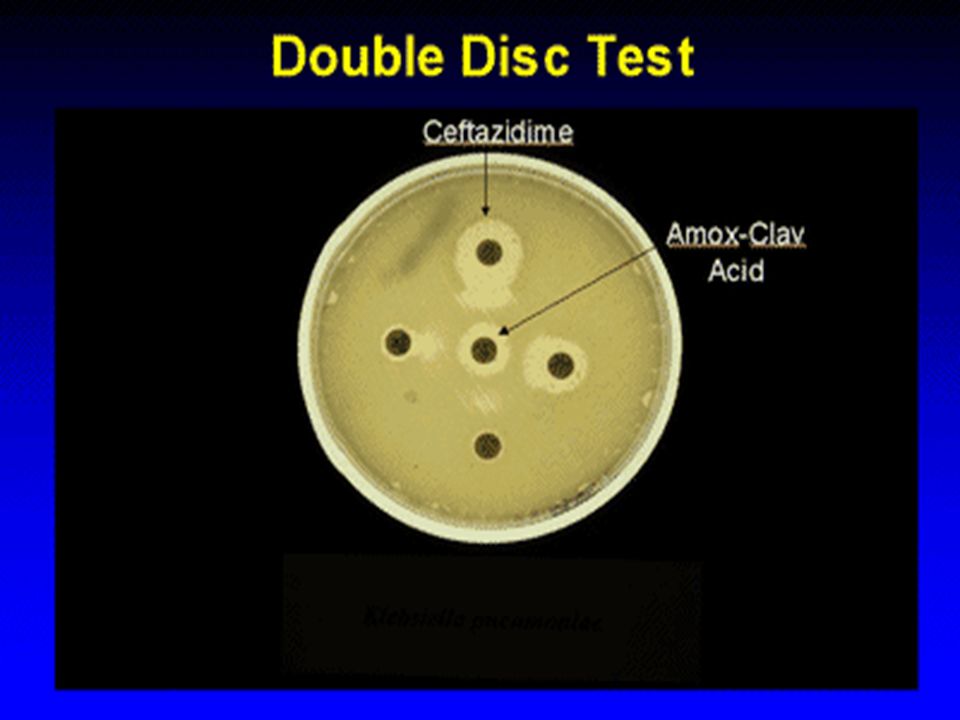
Extended Spectrum -lactamases ESBLs ESBL inactivates oxyamino beta-lactams and fourth-generation cephalosporins (to some extent) and aztreonam Large plasmids encoding multiple antibiotic resistance determinants including aminoglycoside modifying enzymes Strains producing ESBL are typically sensitive to cephamycins and carbapenems Common ESBL-producers: K. pneumoniae, and less common other Enterobactericae

34
Epidemiology of ESBL K. pneumoniae First reported in Germany (1983) Incidence in Europe ranging from 0% to 39% Large plasmids encoding multiple antibiotic resistance determinants including aminoglycoside modifying enzymes Nosocomial outbreaks in ICU’s, long-term care centers Risk Factors: –Instrumentation –Prolonged hospital stay –Prior antibiotic therapy (oxyamino-betalactams)
 Incidence in Europe ranging from 0% to 39% Large plasmids encoding multiple antibiotic resistance determinants including aminoglycoside modifying enzymes Nosocomial outbreaks in ICU’s, long-term care centers Risk Factors: –Instrumentation –Prolonged hospital stay –Prior antibiotic therapy (oxyamino-betalactams).")
35
Klebsiella pneumoniae Resistance to third-generation cephalosporins CDC Fridkin and Gaynes. Clin Chest Med. 1999

36
K. pneumoniae Resistant to Extended- Spectrum -lactam (ESBL) at NNIS Evidence of Inter-hospital Transmission Infect Control Hosp Epidemiolo Mannel DL, et al. Infect Control Hosp Epidemiolo 1997
 at NNIS Evidence of Inter-hospital Transmission Infect Control Hosp Epidemiolo Mannel DL, et al. Infect Control Hosp Epidemiolo")
37
Emergence of Carbapenem- resistant Acinetobacter spp. Frequent use of aminoglycosides, fluroquinolones, ureidopenicillins and third generation cephalosporins Reported from South America, Europe, Far East, Middle East, and United States Numerous outbreaks (some strains susceptible only to polymyxin B) High mortality rates Endemic in some hospitals
 High mortality rates Endemic in some hospitals.")
38
Endemic Carbapenem-Resistant Acinetobacter spp. In Brooklyn, New York 15 hospitals November 1997, all aerobic bacteria collected Acinetobacter spp. (233) accounted for 10% of the gram negative bacilli Carbapenem resistance ranged from 0-100% 10% of isolated were susceptible only to polymyxin Risk factors –Use of third generation cephalosporins plus aztreonam –Environment and healthcare worker hands contamination documented –PFGE documented inter- and intra-hospital spread VM Manikal et al. CID. 2000
 accounted for 10% of the gram negative bacilli Carbapenem resistance ranged from 0-100% 10% of isolated were susceptible only to polymyxin Risk factors –Use of third generation cephalosporins plus aztreonam –Environment and healthcare worker hands contamination documented –PFGE documented inter- and intra-hospital spread VM Manikal et al. CID")
39
Antimicrobial Susceptibility of 233 Acinetobacter spp., 15 Hospital, Brooklyn, New York VM Manikal et al. CID. 2000

40
Control Measures Barrier precautions Oxyamino beta-lactam restriction Selective bowel decontamination

41
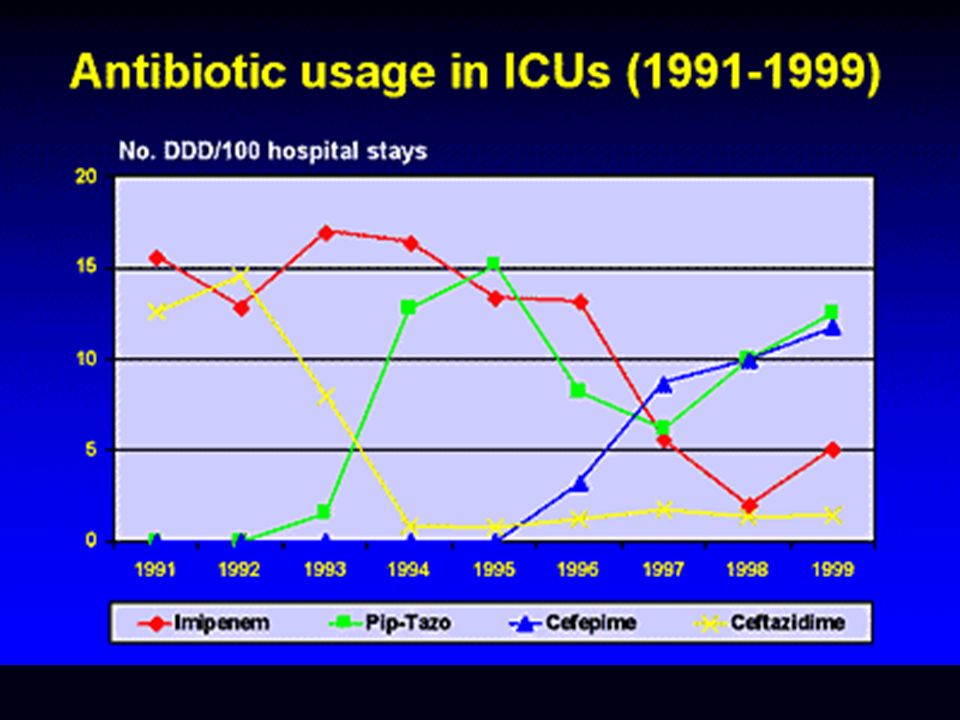
Antimicrobial Utilization and Resistance Interdisciplinary team in Indianapolis to control resistant organisms Interventions: –Reduce third generation cephalosporin use –Reduce imipenem use –Encourage use of ampicillin/sulbactam and piperacillin/tazobactam –Enhance compliance with infection control –Education regarding antimicrobial resistance

42
Antimicrobial Utilization and Resistance Piperacillin/tazobactam resistant Smith. Pharmacotherapy 1999

43
Impact of Formulary Changes on MRSA and Ceftazidime Resistant K. Pneumoniae Reduce usage of cephalosporins, imipenem, clindamycin and vancomycin Increased use of - lactam/ -lactamase inhibitors Landman. Clin. Infect Dis. 1999

44
Ceftazidime Resistant K. pneumoniae Cleveland VA Medical Center

45
Cephalosporin Use and ESBL KP in ICUs Indianapolis VA

46
Impact of a Rotating Empiric Antibiotic Schedule on Infectious Mortality in an Intensive Care Unit Raymond DP. Crit Care Med 01-Jun-2001, 29(6);1101-8
;")
47
Impact of a Rotating Empiric Antibiotic Schedule on Infectious Mortality in an Intensive Care Unit Raymond DP. Crit Care Med 01-Jun-2001, 29(6);1101-8
;")
49
Conclusion Epidemiology of resistance in gram-negative and gram-positive organisms is complex, and is influenced, in part, by selective antimicrobial pressure Control measures for emerging resistance include: –Traditional infection control measures: contact isolation

50
Conclusion Judicious Use of Antimicrobial Decrease cephalosporin use Increase extended-spectrum penicillin/beta- lactamase inhibitor use Limit carbapenem and vancomycin use to desired therapy

51
Handwashing compared to Alcohol Hand

Similar presentations