Download presentation
Presentation is loading. Please wait.

1
UNC Hospitals Sepsis Mortality Reduction Initiative Code Sepsis

2
UNC’s Mortality Index is ranked 65 th out of 73 Academic Hospitals with 500 or more beds in 2014.

3
Sepsis is a VERY common cause of inpatient deaths Hospital Deaths in Patients with Sepsis from Two Independent Cohorts Liu et al JAMA May 18, 2014 All Sepsis 52% All Sepsis 44% National Sample data shows that coding doesn’t catch all sepsis cases, UNC rates are likely higher than reported.

4
If UNC's performance was consistent with the UHC Top Ten, there would have been 218 fewer inpatient deaths in the last two years.

5
MORTALITY REDUCTION STRATEGY Healthcare Acquired Conditions Appropriate Palliative Care Failure to Rescue SEPSIS Improve Early Warning Systems and Response Systems Implement Early Suspicion and Accurate Recognition Sepsis Implement Prompt and Accurate Sepsis First Hour Treatment Implement Antibiotic Stewardship in Sepsis Program

6
UNC Sepsis Implementation Goal: to reduce the raw mortality rate by 10% at UNC Hospitals by June 2016 when compared to 2013 baseline – Scope: Children’s Hospital, ED, ICU’s and all areas of ARRT activation – Phase I: Children’s Hospital implementation complete by June 30, 2015 – paper go live for General ED and Children’s Hospital JUNE 2! – Phases II-IV: ED, Critical Care Units, Inpatient Units

7
Air care – Pediatric Team Pediatric ED MD’s Pediatric Rapid Response Pediatric Hem/Onc Air care – Pediatric Team Pediatric ED MD’s Pediatric Rapid Response Pediatric Hem/Onc Phase I: Feb/Mar 2015 Phase II: April 2015 Phase III: April/May 2015 UNC Children’s Hospital Implementation Team Training Timeline Children’s Hospital and General ED Go-Live June 2 nd !

8
Step 1 Pediatric Rapid Response System Refresher

9
If you are concerned, please call 4-4111 and ask for the Pediatric Rapid Response Team Calling criteria: – Staff or family member is worried about the patient – Acute change in heart rate – Acute change in systolic BP – Acute change in respiratory rate – Acute change in O2 saturation – Mental status changes – New or prolonged seizure – Patient with difficult to control pain or agitation *The criteria for calling the pediatric code team has not been changed Suspect Patient Has Sepsis?

10
Re-engage the Culture There should never be a negative response to this call nor should we second guess the caller of the Pediatric Rapid Response Team. There are no False Alarms We must partner to engage the culture where it is easier to call for help Since 2005 when we started our PRRT, our non-ICU cardiac arrest rate has decreased by 70% and has been sustained to date

11
Goals Prevent cardiac arrests Improve recognition of instability Improve communication Eliminate delay with chain of command Create system-wide safety culture Ideal state would get the care and hands needed to keep patient on wards Transfer to ICU may be needed but don’t wait to call until too late

12
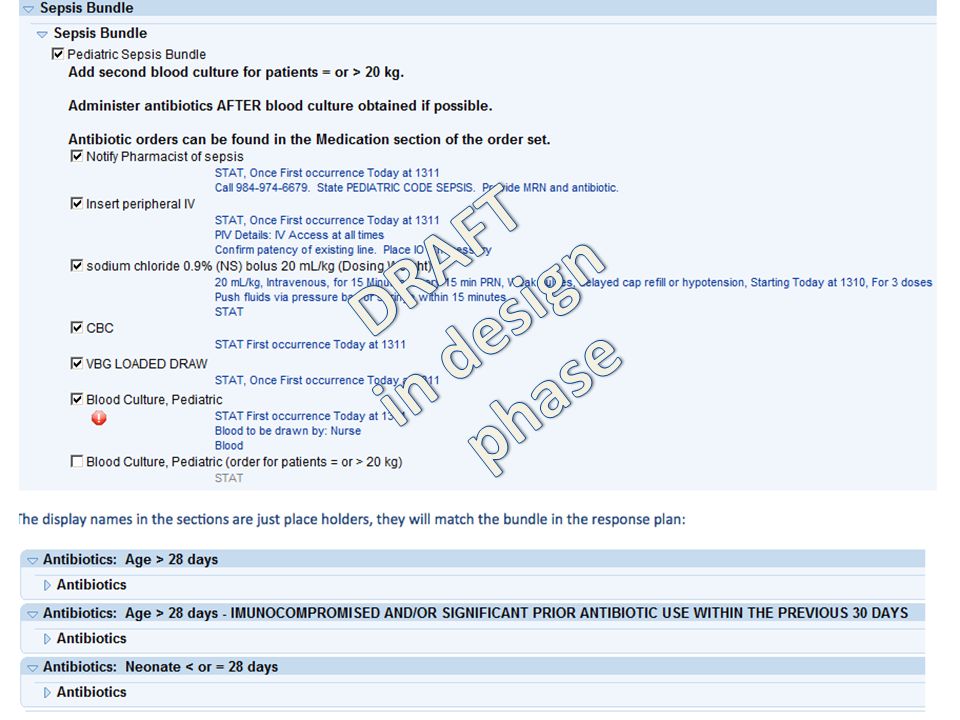
Step 2 Screen and Confirm Sepsis and Complete the Pediatric Code Sepsis Bundle

13
<1 month 6-12 years 1-2 years >1 month-<1 years 13-18 years 180 > 120 > 160 160 > 100 Does patient have > 2 of the following: Abnormal HR or RR + UNC PEDIATRIC Sepsis Screen PEDIATRIC Sepsis Response Team Assess to confirm sepsis Resuscitation Access (may need PIVs in addition to port or PICC), Fluids, use syringes or pressure bags (no infusion pumps), Monitor, and O 2 Labs Drawn (Blood Culture BEFORE abx, CBC with Diff, loaded gas) Alert Pharmacy of sepsis for faster antibiotic delivery - use closed loop communication Initial dose of antibiotic (even if no blood culture is available) see pediatric sepsis antibiotic algorithm COMPLETE BUNDLE IN < 60 MINUTES & notify primary team: Transfer decision (ICU if 60ml/kg needed or otherwise indicated) Then Trigger “PEDS SEPSIS” Response - in design > 60 > 40 > 30 > 16 2-5 years> 140> 34 Suspected Infection Abnormal HRAbnormal RR Temp 38 in 0 -3 months Temp 38.5 in 3 months to adult (home temp also valid) WBC count >12,000 or < 5000 High Risk* (see next page)
, Fluids, use syringes or pressure bags (no infusion pumps), Monitor, and O 2 Labs Drawn (Blood Culture BEFORE abx, CBC with Diff, loaded gas) Alert Pharmacy of sepsis for faster antibiotic delivery - use closed loop communication Initial dose of antibiotic (even if no blood culture is available) see pediatric sepsis antibiotic algorithm COMPLETE BUNDLE IN < 60 MINUTES & notify primary team: Transfer decision (ICU if 60ml/kg needed or otherwise indicated) Then Trigger PEDS SEPSIS Response - in design > 60 > 40 > 30 > years> 140> 34 Suspected Infection Abnormal HRAbnormal RR Temp 38 in 0 -3 months Temp 38.5 in 3 months to adult (home temp also valid) WBC count >12,000 or < 5000 High Risk* (see next page)")
14
PEDIATRIC Sepsis HIGH RISK* Patients Bone Marrow Transplant Other Immunocompromise Solid Organ Transplant Complex Urogenital Anatomy/Repair Asplenia (including Sickle Cell Disease) Malignancy Central Line/PICC/Port Chronic Steroid Dependence (asthma, autoimmune disease) Severe Neurologic Impairment or technology dependence
 Malignancy Central Line/PICC/Port Chronic Steroid Dependence (asthma, autoimmune disease) Severe Neurologic Impairment or technology dependence")
15
What About Patients In the ED?

16
WORKING DRAFT

17
Phase I: March/April 2015 Air care ED advanced care team ARRT –primary and secondary Hem/Onc Responders Phase II: June/July 2015 ED Care Team Inpatient Care Areas Phase III: August 2015 All Medical Center staff UNC Adult Implementation Team Training Timeline Children’s Hospital and General ED Go-Live June 2 nd !

18
WORKING DRAFT

19
What about adult inpatients? For now the Adult Rapid Response Team is using the bundle for cases of sepsis Larger screening is in pilot phases to bring the rapid response team to the septic patient sooner MEWS pilot testing in 2014 EPIC foundation Same culture challenges for adult rapid response team as pediatric Empower staff to call the rapid response team MEWS may not find all patients that need the rapid response team

20
Does patient have > 2 of the following: Respiratory Rate >20 + UNC Adult Early Sepsis Screen ADULT Sepsis Response Team Assess to confirm sepsis COMPLETE BUNDLE IN < 60 MINUTES & notify primary team: Then Trigger Sepsis Response - in design Suspected Infection Core Temp 38 (home temp also valid) WBC count 12 High Risk* (see next page) Heart Rate >90 Altered Mental State Measure Lactate Level Obtain Blood Culture (attempt 2 sets prior to antibiotic) Alert Pharmacy of sepsis for faster antibiotic delivery - use closed loop communication Initial dose of antibiotic (even if no blood culture is available) see adult sepsis antibiotic algorithm Consider transfer to higher level care if inadequate response to fluid resuscitation or based on clinical status Fluid Resuscitation 30 ml/kg or 2L in the first hour
 WBC count 12 High Risk* (see next page) Heart Rate >90 Altered Mental State Measure Lactate Level Obtain Blood Culture (attempt 2 sets prior to antibiotic) Alert Pharmacy of sepsis for faster antibiotic delivery - use closed loop communication Initial dose of antibiotic (even if no blood culture is available) see adult sepsis antibiotic algorithm Consider transfer to higher level care if inadequate response to fluid resuscitation or based on clinical status Fluid Resuscitation 30 ml/kg or 2L in the first hour")
21
ADULT Sepsis HIGH RISK* Patients Immunocompromised Diabetes Indwelling medical device Transplant (BMT or Solid Organ) Recent surgery/invasive procedure Burn Patients Congestive Heart Failure Cancer Geriatric
 Recent surgery/invasive procedure Burn Patients Congestive Heart Failure Cancer Geriatric")
23
Presentation In Hospital Adult Patient Pt. admitted for a major surgical procedure and able to transfer out of ICU to floor on POD#2 On POD#8 at 0900, nursing begins charting that pt. is confused/somnolent/hallucinating after having been alert and oriented for the six days prior. – VS at 0900 – HR 106, RR 18, SBP 107, Temp 36.9 *In new system Pt would have had a Early Warning Score (MEWS) score of 2 which may have prompted a physician notification of change and a rapid response consult POD#8 at 1500, pt. continues to be confused/somnolent – VS at 1500 - HR 113, RR 18, SBP 89, Temp 35.3 – * Pt would have had a MEWS score of 5 based which may have triggered a rapid response, potential sepsis screening and Q 1 hr monitoring No rapid response called and pt. remains on the floor
 score of 2 which may have prompted a physician notification of change and a rapid response consult POD#8 at 1500, pt. continues to be confused/somnolent – VS at HR 113, RR 18, SBP 89, Temp 35.3 – * Pt would have had a MEWS score of 5 based which may have triggered a rapid response, potential sepsis screening and Q 1 hr monitoring No rapid response called and pt. remains on the floor.")
24
20 hrs later, at 1100 on POD#9, nurse charts that pt. was extremely confused and hallucinating – VS at 1100 – HR 120, RR 18, SBP 81, Temp 35.6 – No urine output since POD#8 at 2200 – Elevated MEWS score along with staff concern could have triggered a rapid response activation POD#9 MD note states that sepsis suspected – Blood culture ordered at 1210 – 2250ml of Albumin 5% given between 1225 and 1809 Pt. weighed 81.6 kg – Zosyn ordered and first dose given at 1326 – Vanc ordered and first dose given at 1830 Pt. transferred to SICU at 1458 on POD#9 First lactate not drawn until POD#10 at 1530 Pt. died 1 month post procedure Adult Patient - cont’d

25
Pediatric ED Code Sepsis Pilot Phase 0853 – High Risk Chronic Illness Pediatric Patient and mother arrive in ED 0855 – Triage nurse notes mother’s reports that pt. had Tmax of 106.5 and HR in 200s and immediately notifies physician and nurse to take pt. back. 0855 - ED physician assessment – Vitals reviewed, initial exam – Infection suspected and code sepsis initiated 0900 - Pt. placed on full cardiac monitoring 0908 - First set of vitals in ED: HR 170, RR 42, Temp 36.3 temporal (rectal temp 10 min. later was 38.4), Sats 89% on 2 L NC
, Sats 89% on 2 L NC.")
26
Pediatric ED Code Sepsis Pilot Phase 0911 - MD ordered ceftriaxone and vancomycin and called pharmacist who started preparing abx 0917 – Blood culture drawn 0920 – VBG and lactate drawn (lactate 2.2) 0922 – first 20ml/kg NS bolus given over 11 min. 0931 – IV ceftriaxone given 0943 – second 20 ml/kg NS bolus given over 14 min. 1005 – IV vancomycin given Patient discharged home after several week hospitalization

27
Content: Background Resources Sepsis Toolkit FAQs Need Help? Content: Background Resources Sepsis Toolkit FAQs Need Help? sepsisfeedbackunch@unchealth.unc.edu

Similar presentations















 Surgery Nursing House supervisor ACLS trained nurse from CCU/CTICU.>")


 Innovation Poster Session HRT1215 – Innovation Awards Sydney.>")
