Download presentation
Presentation is loading. Please wait.

1
Hodgkin’s Disease Mark D. Browning, M.D. February 22, 2016

2
Hodgkin’s Disease* Epidemiology HD is uncommon, 9,200 new cases/yr with 1,180 deaths/year in 2014 Incidence demonstrates a bimodal distribution – peak ages 15-35 and second smaller peak after age 50

3
Pathology/Clinical Staging* The characteristic malignant cell is the CD30+ Reed- Sternberg cell, thought to be an antigen presenting cell in the lymph node HD starts in the nodes and spreads predominantly via the lymphatics to adjacent nodes(unlike NHL, it does not spread through the blood)…Contiguous Spread Stage I- single node region, Stage II- 2 or more nodal groups on the same side of the diaphragm, Stage III- nodes on both sides of the diaphragm involved, Stage IV- any extra-lymphatic involvement (e.g. liver, marrow)
.")
4
Presentation* Lymphadenopathy B symptoms (night sweats, weight loss, fever). These represent a worse prognosis, and are added to the staging

5
Treatment* Typically very responsive to treatment, so have very good long term survival (Cure!) Local radiation alone can be curative for stage I Chemotherapy(+/- Radiation) for Stage II-IV Radiation and/or chemotherapy can cure > 75% of all HD If relapsed, autologous stem cell transplantation can cure up to 45% of those relapses.

6
Individuals in World with Hodgkin’s Disease Paul Allen(Microsoft) 1983…NHL 2009 Howard Carter…died of Hodgkin’s Disease in 1939…Egyptologist…discovered Tutankhamun’s Tomb Mario Lemieux…Hockey Star Prithviraj Kapoor…Indian Hindi Film Industry …died 1972 of Hodgkin’s Dis.
 1983…NHL 2009 Howard Carter…died of Hodgkin’s Disease in 1939…Egyptologist…discovered Tutankhamun’s Tomb Mario Lemieux…Hockey Star Prithviraj Kapoor…Indian Hindi Film Industry …died 1972 of Hodgkin’s Dis.")
7
Hodgkin’s Lymphoma 0.6% of All Cancers in USA

8
New Cases by Age

9
5 Year Survival

10
% of Deaths by Age Group

11
*Hodgkin’s Disease Incidence & Epidemiology 2.7 per 100,000 in USA (2002-08 SEER data) 9,190 new cases per year in USA in 2014 5100 men and 4090 women 5100 men and 4090 women Deaths in 2014 were 1,180 Lifetime Risk 0.2% or 1/429 individuals Prevalence Rate…185,793 in USA in 2014 Median age is 26-31
 9,190 new cases per year in USA in men and 4090 women 5100 men and 4090 women Deaths in 2014 were 1,180 Lifetime Risk 0.2% or 1/429 individuals Prevalence Rate…185,793 in USA in 2014 Median age is 26-31")
12
New Cases, Deaths, & 5 Year Survival Rates

13
Hodgkin’s Disease Thomas Hodgkin/1832..clinical…Carl Sternberg/1898 Dorothy Reed/1902..pathology Radiation palliated large lymph nodes in the first two decades of the 20 th century Few patients survived more than 5 years Early stage patients were not usually treated with Radiation therapy prior to 1960 Henry Kaplan/Vince DeVita..1960s Rad/chemo cured early and advanced stages of disease respectively…MODERN THERAPY OF CANCER BEGAN!!!!!!!

14
*Hodgkin’s Disease Tissue Types Nodular Sclerosis Mixed Cellularity Lymphocyte Predominant Lymphocyte Depleted Diagnosis: Reed-Sternberg Cells

15
*Reed-Sternberg Cell

16
*Hodgkin’s Disease Immunohistochemical Markers Reed Sternberg Cells CD15 & *CD30 +…CD20 negative Nodular Lymphocyte Predominant CD20 + Normal Mature B-cell Markers CD 15 & *CD 30 negative

21
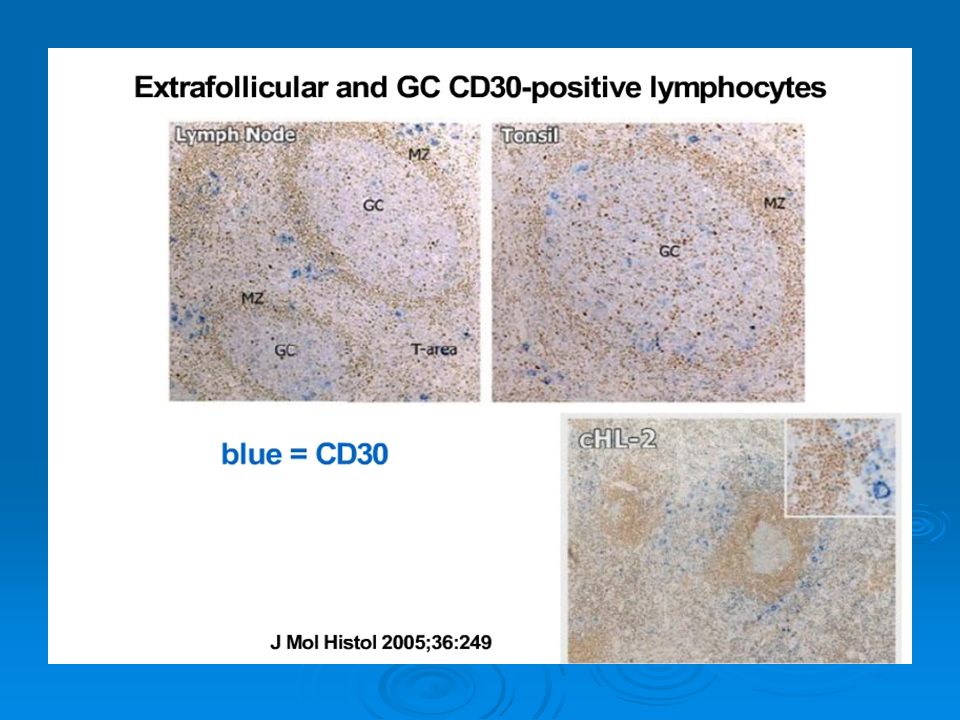
*Hodgkin Lymphoma (HL) >95% of HL is CD30-positive 1 Lymphoid neoplasm defined by the presence of Reed- Sternberg (RS) cells in a reactive infiltrate 2,3 Estimated 8,830 new cases in the US in 2012 4 Reproduced with permission from Mani H et al, 2009 5 References: 1. Diehl V et al. In: DeVita VT Jr et al, eds. Cancer: Principles and Practice of Oncology. Vol 2. 8th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2008:2167-2220. 2. Pileri SA et al. J Clin Pathol. 2002;55(3):162-176. 3. Stein H et al. In: Swerdlow SH et al, eds. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. Lyon, France: IARC; 2008:326-329. 4. American Cancer Society. Cancer Facts & Figures 2011. Atlanta, GA: American Cancer Society; 2011. 5. Mani H et al. Clin Lymphoma Myeloma. 2009;9(3):206-216. 21
: Stein H et al. In: Swerdlow SH et al, eds. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed. Lyon, France: IARC; 2008: American Cancer Society. Cancer Facts & Figures Atlanta, GA: American Cancer Society; Mani H et al. Clin Lymphoma Myeloma. 2009;9(3):")
22
*Hodgkin’s Disease

23
Hodgkin’s Disease Incidence Males 1.4 fold more than females Male predominance ages 50 Female predominance ages 10 - 40 Small family size High standard of living in childhood High level of maternal school education

24
*Hodgkin’s Disease Increased Risk Factors Immunocompromised State HIV, S/P Organ Transplant HIV, S/P Organ Transplant Past Epstein-Barr infection Brother or Sister with disease (genetics) Environmental exposure Herbicides, Woodworking, Meat processing & Livestock Herbicides, Woodworking, Meat processing & Livestock Geography USA, Canada & Northern Europe….less in Asia USA, Canada & Northern Europe….less in Asia
 Environmental exposure Herbicides, Woodworking, Meat processing & Livestock Herbicides, Woodworking, Meat processing & Livestock Geography USA, Canada & Northern Europe….less in Asia USA, Canada & Northern Europe….less in Asia")
25
*Hodgkin’s Disease Clinical Manifestations 90% of time supradiaphragmatic Lymph nodes including mediastinum Lymph nodes including mediastinum Dry cough, substernal discomfort, enlarged lymph nodes Fever, weight loss or night sweats

26
Lymphadenopathy

27
Nodular Sclerosing Hodgkin’s Disease…Mediastional Mass

28
*Nodular Sclerosing Hodgkin’s Disease---Lymph Node Biopsy

29
*Reed-Sternberg Cell

30
*Hodgkin’s Disease Staging Tests Biopsy Reviewed (Tissue is the Issue) Hx & PE CBC, LFTs, ESR, CXR CT of Neck, chest, abdomen & pelvis PET/CT scan Bilateral bone marrow aspirates and biopsies Staging laparotomy …none since 1990
 Hx & PE CBC, LFTs, ESR, CXR CT of Neck, chest, abdomen & pelvis PET/CT scan Bilateral bone marrow aspirates and biopsies Staging laparotomy …none since 1990")
31
*Evaluation Tests PET/CT Beginning of Therapy & The End of Therapy If PET scan negative after 2 cycles..prognosis is excellent despite prognostic variables Standard CT scan serially to evaluate response

32
*Young Patient Population Counseling Fertility Sperm, Ova or Embryo cryopresevation Cardiovascular Risks Increase Advise against smoking Breast Cancer Risk Increased if Radiation Therapy Used in Treatment

33
Hodgkin’s Disease

34
*Hodgkin’s Disease Staging

35
*Hodgkin’s Prognosis Survival at 5 years…2012 Favorable I/II92-97% Advanced Stage81-93% Poor Prognosis Advanced78%

36
*Historical Outcomes Bulk of Disease Age Number of nodal sites Sedimentation Rate (ESR) IPS in Early & Advanced HL
 IPS in Early & Advanced HL")
37
*International Prognostic Score 7 Variables (5141 Patients from 25 Centers 1983-1992) Albumin <4 Hgb <10.5 Male gender >45 years of age Stage IV WBC >15,000 Lymphocyte Count < 600 or <8%
 Albumin <4 Hgb <10.5 Male gender >45 years of age Stage IV WBC >15,000 Lymphocyte Count < 600 or <8%")
38
*IPS Re-examined in Canada 1990 thru 2008 with 579 Patients All Groups Survival Improved by 5% Transplantation Salvage Therapy Options Reduction in second malignancies Improved Supportive Care Early Recognition of Toxicity Freedom From Progression (FFP) Improved Accurate staging, increased intensity with decreased delays or dose reductions
 Improved Accurate staging, increased intensity with decreased delays or dose reductions")
39
Therapy Results: Surveillance Epidemiology & End Results (SEER) 80-84 vs 2000-2004 Prognosis Significantly better in 2000- 2004 Abandoned splenectomy Radiation Fields/Doses Decreased MOPP eliminated from first line therapy Results of Stem Cell Transplants for Relapsed patients improved Indirect evidence to reduce intensity of first line therapy has not resulted in worse survival
 vs Prognosis Significantly better in Abandoned splenectomy Radiation Fields/Doses Decreased MOPP eliminated from first line therapy Results of Stem Cell Transplants for Relapsed patients improved Indirect evidence to reduce intensity of first line therapy has not resulted in worse survival")
40
Prognostic Studies

41
*Earlier Survival Studies with therapy

42
*Hodgkin’s Disease Chemotherapy Options…ABVD is USA Standard

43
*Hodgkin’s Therapy Radiation Therapy for pathologic I & IIA non- bulky disease Mantle or Mini-mantle +/Chemo Mantle or Mini-mantle +/Chemo Periaortic, splenic bed infrequently in 2011 Periaortic, splenic bed infrequently in 2011 Good prognosis IA & IIA patients without a Lap Rad +/- chemo Rad +/- chemo Radiation therapy -- total nodal III A1 disease…rarely done today III A1 disease…rarely done today Chemotherapy -- ABVD, MOPPABV III A1/2, IIIB, & IV A or B +/-Rad Rx for Bulk III A1/2, IIIB, & IV A or B +/-Rad Rx for Bulk

44
*Hodgkin’s Disease…Radiation Therapy Options

45
*Hodgkin’s Therapy…2011 Oliver Press,MD,PhD…Lymphoma Research Chair Early Stage Disease…Favorable Prognosis…New Standard (2011) 2 cycles of ABVD 20 Gy of Involved Field Radiation Therapy Engert, NEJM,2010
 2 cycles of ABVD 20 Gy of Involved Field Radiation Therapy Engert, NEJM,2010")
46
*Optimal Therapy Early-Stage with PET(Favorable: young,low esr, limited nodal sites) ABVD x2 + IFRT ABVD x2 …interim PET/CT PET negative…2 to 4 additional cycles PET positive…2 additional cylces of ABVD & IFRT OR alternate chemotherapy + IFRT
 ABVD x2 + IFRT ABVD x2 …interim PET/CT PET negative…2 to 4 additional cycles PET positive…2 additional cylces of ABVD & IFRT OR alternate chemotherapy + IFRT")
47
*Optimal Therapy Non-bulky Stage I/II with Unfavorable features: ( > 40, Increased ESR, >2/3 LN Areas) ABVD x 4 + IFRT ABVD x 2 followed by interim PET/CT If PET negative, 2 to 4 additional cycles of ABVD If PET positive, 2 additional cycles of ABVD + IFRT or alternative chemotherapy + IFRT
 ABVD x 4 + IFRT ABVD x 2 followed by interim PET/CT If PET negative, 2 to 4 additional cycles of ABVD If PET positive, 2 additional cycles of ABVD + IFRT or alternative chemotherapy + IFRT")
48
*Optimal Therapy…Bulky stage I/II ABVD x 4-6 cycles 30 Gy IFRT MC…30 yo female

49
Hodgkin’s Therapy Early Stage Disease Unfavorable 4 cycles of ABVD + 20/30Gy IF Rad Rx 4 cylces of BEACOPP + 20/30Gy IF Rad Rx

50
Hodgkin’s Therapy Advanced Favorable Prognosis ABVD x 6 to 8 cycles (68% PFS/84% OS) ABVD x 6 to 8 cycles + IF Radiation Therapy BEACOPP Superior PFS (81%) & Expected Improved Overall Survival (92%) in indirect comparisons
 ABVD x 6 to 8 cycles + IF Radiation Therapy BEACOPP Superior PFS (81%) & Expected Improved Overall Survival (92%) in indirect comparisons")
51
Hodgkin’s Therapy Advanced Unfavorable Prognosis ABVD for 6 to 8 cycles BEACOPP (Escalated)
")
52
Advanced Stage Hodgkin’s Disease

53
ABVD vs Stanford V

55
Prognosis: Alternative Frontline Regimens BEACOPP or escalated BEACOPP may be used for advanced disease 1 5-year OS: 87% with BEACOPP 87% with BEACOPP 92% with escalated BEACOPP 92% with escalated BEACOPP Stanford V is an alternative for locally extensive or advanced disease 2 5-year OS: 92% 92% BEACOPP: bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine and prednisone Stanford V: nitrogen mustard, doxorubicin, bleomycin, vincristine, vinblastine, etoposide and prednisone References: 1. Engert A et al. J Clin Oncol. 2009;27(27):4548-4554. 2. Hoskin PJ et al. J Clin Oncol. 2009;27(32):5390-5396. 55
: Hoskin PJ et al. J Clin Oncol. 2009;27(32):")
56
Prognosis: Frontline ABVD, developed in the 1970s, remains the preferred treatment regimen 1 5-year overall survival (OS): >90% in early-stage HL 2 >90% in early-stage HL 2 90% in advanced disease 3 90% in advanced disease 3 However, no new frontline therapies have been approved for HL for over 30 years 4 ABVD: doxorubicin, bleomycin, vinblastine and dacarbazine References: 1. National Comprehensive Cancer Network (NCCN). NCCN clinical practice guidelines in oncology: Hodgkin lymphoma (version 2.2011). Fort Washington, PA: NCCN; 2011. 2. Bonadonna G et al. J Clin Oncol. 2004;22(14):2835-2841. 3. Hoskin PJ et al. J Clin Oncol. 2009;27(32):5390-5396. 4. Younes A. Hematology Am Soc Hematol Educ Program. 2009:507-519. 56
. NCCN clinical practice guidelines in oncology: Hodgkin lymphoma (version ). Fort Washington, PA: NCCN; Bonadonna G et al. J Clin Oncol. 2004;22(14): Hoskin PJ et al. J Clin Oncol. 2009;27(32): Younes A. Hematology Am Soc Hematol Educ Program. 2009:")
57
*Late Complications of Therapy 57 Patients treated for HL before age 21: Are nearly 14 times more likely than the general population to die from cardiovascular disease Are nearly 14 times more likely than the general population to die from cardiovascular disease Are nearly 15 times more likely to die from solid tumors Are nearly 15 times more likely to die from solid tumors Reference: 1. Aleman BM et al. J Clin Oncol. 2003;21(18):3431-3439. Mortality risk due to HL plateaus after 10 years, whereas risks due to second malignancy, cardiovascular disease and other causes increase continually following treatment Mortality by cause of death
: Mortality risk due to HL plateaus after 10 years, whereas risks due to second malignancy, cardiovascular disease and other causes increase continually following treatment Mortality by cause of death.")
58
Hodgkin’s Salvage Therapy Chemo if only radiation therapy in past Change in Chemo Anti-CD30 antibody…approved fall 2011 Autologous marrow transplant

59
*Therapy Results Lethal Disease prior to 1963 Radiation Rx &/or Chemo changed the prognosis 90% cure for early stage and 80% for advanced stage patients in 2011 Future Therapy Ensure patients a future without therapy- induced sequelae…PET may be beneficial

60
ASCT for R/R HL More than half of patients with R/R HL relapse after autologous stem cell transplantation (ASCT) 1,2 References: 1. Sureda A et al. Ann Oncol. 2005;16(4):625-633. 2. Majhail NS et al. Biol Blood Marrow Transplant. 2006;12(10):1065 ‑ 1072. 3. Martinez C et al. J Clin Oncol. 2010;28(15)(suppl):8060. 60 2 years55% 5 years32% Overall survival among those who relapse following ASCT 3
: Majhail NS et al. Biol Blood Marrow Transplant. 2006;12(10):1065 ‑ Martinez C et al. J Clin Oncol. 2010;28(15)(suppl): years55% 5 years32% Overall survival among those who relapse following ASCT 3.")
61
Cytotoxic agent The synthetic microtubule-disrupting agent, monomethyl auristatin E (MMAE, vedotin), that induces target cell death ADCETRIS is a CD30-Directed Antibody-Drug Conjugate ADCETRIS consists of three components: Linker A synthetic protease- cleavable linker that covalently attaches MMAE to the CD30-directed antibody and releases the agent within the target cell Antibody The antibody, brentuximab, specific for CD30 Reference: ADCETRIS [Prescribing Information]. Bothell, WA: Seattle Genetics Inc; 2012.
![Cytotoxic agent The synthetic microtubule-disrupting agent, monomethyl auristatin E (MMAE, vedotin), that induces target cell death ADCETRIS is a CD30-Directed Antibody-Drug Conjugate ADCETRIS consists of three components: Linker A synthetic protease- cleavable linker that covalently attaches MMAE to the CD30-directed antibody and releases the agent within the target cell Antibody The antibody, brentuximab, specific for CD30 Reference: ADCETRIS [Prescribing Information].](http://images.slideplayer.com/35/10302062/slides/slide_61.jpg "Bothell, WA: Seattle Genetics Inc;")
62
Relapsed or Refractory HL Up to 10% of all patients are refractory to initial therapy 1 Up to 30% of all patients will eventually relapse 1 The relapse rate exceeds 50% for patients with ≥4 factors on the International Prognostic Index (IPI) 2 : Serum albumin <4 g/dL Serum albumin <4 g/dL Hemoglobin <10.5 g/dL Hemoglobin <10.5 g/dL Male gender Male gender Stage IV disease Stage IV disease Age >45 years Age >45 years White cell count ≥15,000/mm 3 White cell count ≥15,000/mm 3 Lymphocyte count <600/mm 3 or <8% of white cell count Lymphocyte count <600/mm 3 or <8% of white cell count References: 1. Quddus F et al. Cancer J. 2009;15(2):161-163. 2. Hasenclever D et al. N Engl J Med. 1998;339(21):1506-1514. 62
: Hasenclever D et al. N Engl J Med. 1998;339(21):")
63
Options Limited for Older Adult Population 63 Older patients with HL have a poorer risk profile and do not tolerate therapy as well as younger patients 1,2 The remission rate, relapse-free survival and OS decrease within each decade after 50 years of age 3 References: 1. Engert A et al. J Clin Oncol. 2005;23(22):5052-5060. 2. Punnett A et al. Semin Radiat Oncol. 2010;20(1):30-44. 3. Canellos GP. Hematol Oncol Clin North Am. 2007;21(5):929-941. OS in elderly vs younger patients with HL 1
: Punnett A et al. Semin Radiat Oncol. 2010;20(1): Canellos GP. Hematol Oncol Clin North Am. 2007;21(5): OS in elderly vs younger patients with HL 1.")
64
*Outcomes Depending on IPS Canada(1990-2008)Blood 2009
Blood 2009")
65
ADCETRIS Indications ADCETRIS is a CD30-directed antibody-drug conjugate (ADC) indicated for the treatment of: Hodgkin lymphoma (HL) after failure of autologous stem cell transplant (ASCT) Hodgkin lymphoma (HL) after failure of autologous stem cell transplant (ASCT) HL in patients who are not ASCT candidates after failure of at least 2 prior multiagent chemotherapy regimens HL in patients who are not ASCT candidates after failure of at least 2 prior multiagent chemotherapy regimens Systemic anaplastic large cell lymphoma (sALCL) after failure of at least 1 prior multiagent chemotherapy regimen Systemic anaplastic large cell lymphoma (sALCL) after failure of at least 1 prior multiagent chemotherapy regimen These indications are based on response rate. There are no data available demonstrating improvement in patient-reported outcomes or survival with ADCETRIS. Please see accompanying full Prescribing Information and Important Safety Information, including Boxed WARNING, on slides 15-18. Reference: ADCETRIS [Prescribing Information]. Bothell, WA: Seattle Genetics Inc; 2012.

66
Summary Up to 30% of patients with HL will relapse 1 HL will progress after ASCT in ≈50% of patients 2,3 Relapse after ASCT generally carries a poor prognosis 4 Benefit of allo-SCT may be offset by high TRM 5 References: 1. Diehl V et al. In: DeVita VT Jr et al, eds. Cancer: Principles and Practice of Oncology. Vol 2. 8th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2008:2167-2220. 2. Sureda A et al. Ann Oncol. 2005;16(4):625-633. 3. Majhail NS et al. Biol Blood Marrow Transplant. 2006;12(10):1065 ‑ 1072. 4. Martinez C et al. J Clin Oncol. 2010;28(15)(suppl):8060. 5. Sureda A et al. J Clin Oncol. 2008;26(3):455-462. 66 Seattle Genetics and are US registered trademarks of Seattle Genetics, Inc. © 2011 Seattle Genetics, Inc., Bothell, WA 98021. All rights reserved. Produced in USA 9/11
: Majhail NS et al. Biol Blood Marrow Transplant. 2006;12(10):1065 ‑ Martinez C et al. J Clin Oncol. 2010;28(15)(suppl): Sureda A et al. J Clin Oncol. 2008;26(3): Seattle Genetics and are US registered trademarks of Seattle Genetics, Inc. © 2011 Seattle Genetics, Inc., Bothell, WA All rights reserved. Produced in USA 9/11.")
67
Problems With Allo-SCT for HL A minority of patients are eligible Experimental approach; highly controversial Benefit of reduced relapse rates is offset by high TRM of 24% (RIC allo-SCT) to 49% (myeloablative allo- SCT) Acute graft-vs-host disease (GVHD) in ≈50% of patients Chronic GVHD in ≈35% of patients High relapse rate: 5-year PFS (all allo-SCT) ≈20% Reference: Sureda A et al. J Clin Oncol. 2008;26(3):455-462. 67
:")
68
Problems With Allo-SCT for HL A minority of patients are eligible Experimental approach; highly controversial Benefit of reduced relapse rates is offset by high TRM of 24% (RIC allo-SCT) to 49% (myeloablative allo-SCT) Acute graft-vs-host disease (GVHD) in ≈50% of patients Chronic GVHD in ≈35% of patients High relapse rate: 5-year PFS (all allo- SCT) ≈20% Reference: Sureda A et al. J Clin Oncol. 2008;26(3):455-462. 68
:")
69
Allogeneic Transplantation for HL Despite high treatment-related mortality (TRM), allogeneic stem cell transplantation (allo-SCT) is still utilized as an option in relapsed or refractory HL, even after failed ASCT, because of the young age of many of these patients Dose intensity can be delivered in myeloablative allograft Dose intensity can be delivered in myeloablative allograft Donor cells free from tumor-cell contamination Donor cells free from tumor-cell contamination Possible graft-vs-tumor effect Possible graft-vs-tumor effect Reduced-intensity conditioning allogeneic stem cell transplantation (RIC allo-SCT) decreases early TRM Reduced-intensity conditioning allogeneic stem cell transplantation (RIC allo-SCT) decreases early TRM Reference: Kuruvilla J et al. Blood. 2011;117(16):4208-4217. 69
:")
70
Salvage Therapy for R/R HL Complete remission (CR) is a desirable goal: transplantation in CR improves OS and time to treatment failure 1,2 DHAP: cisplatin, cytarabine and dexamethasone; GDP: gemcitabine, dexamethasone and cisplatin; GVD: gemcitabine, vinorelbine and pegylated liposomal doxorubicin; ICE: ifosfamide, carboplatin and etoposide; RR: response rate References: 1. Majhail NS et al. Biol Blood Marrow Transplant. 2006;12(10):1065 ‑ 1072. 2. Sureda A et al. J Clin Oncol. 2001;19(5):1395-1404. 3. Josting A et al. Ann Oncol. 2005;16(1):116-123. 4. Moskowitz CH et al. Blood. 2001;97(3):616-623. 5. Bartlett NL et al. Ann Oncol. 2007;18(6):1071-1079. 6. Kuruvilla J et al. Cancer. 2006;106(2):353-360. Salvage regimen NRR (%)CR (%) DHAP 3 998721 ICE 4 658817 GVD 5 917019 GDP 6 3462 9 Results with salvage chemotherapy pre-ASCT 70
:1065 ‑ Sureda A et al. J Clin Oncol. 2001;19(5): Josting A et al. Ann Oncol. 2005;16(1): Moskowitz CH et al. Blood. 2001;97(3): Bartlett NL et al. Ann Oncol. 2007;18(6): Kuruvilla J et al. Cancer. 2006;106(2): Salvage regimen NRR (%)CR (%) DHAP ICE GVD GDP Results with salvage chemotherapy pre-ASCT 70.")
Similar presentations






>")
















 Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.>")