Download presentation
Presentation is loading. Please wait.

1
Clinical Management of Lymphoma 新光醫院 血液腫瘤科 溫 武 慶

2
Malignant Lymphoma Neoplastic lymphoid cells Arrested at different stages of normal differentiation Tumor formation in the lymph nodes (usually) or extranodal areas
 or extranodal areas")
6
90.9.2890.11.2891.03.13

7
Classification of Lymphoma Hodgkin lymphoma (HL) –Classic (CHL) LR (lymphocyte-rich) LD (lymphocyte-depleted) MC (mixed cellularity) 17% NS (nodular sclerosis) 80% –NLPHL (nodular lymphocyte predominant) 3-8% Non-Hodgkin lymphoma (NHL) –B-cell, T-cell –High, intermediate, low grade (REAL/WHO classification)
 –Classic (CHL) LR (lymphocyte-rich) LD (lymphocyte-depleted) MC (mixed cellularity) 17% NS (nodular sclerosis) 80% –NLPHL (nodular lymphocyte predominant) 3-8% Non-Hodgkin lymphoma (NHL) –B-cell, T-cell –High, intermediate, low grade (REAL/WHO classification)")
8
Differences in HL and NHL HL NHL RS or L & H cells Lymphoma cells nodular diffuse

9
Differences in HL and NHL HLNHL Cell RS (Reed-Sternberg) L & H (lymphocytic and histiocytic) cells B- and T- cells GradeLowLow intermediate high SpreadLymphatic (contiguously) Hematogenous Lymphatic
 L & H (lymphocytic and histiocytic) cells B- and T- cells GradeLowLow intermediate high SpreadLymphatic (contiguously) Hematogenous Lymphatic")
10
Lymphoma Work-up Diagnosis and Classification Stage Other prognostic factors –Age –LDH –Beta-2 microglobulin –IPI (international prognostic index)
")
13
Staging Work-up CBC, platelet LDH, biochemistry CXR, chest/abdomen/pelvic CT PET scan Bone marrow examination

14
Lymphoma Stage 1974 Ann Arbor, 1988 Cotswolds I1 single LN region or lymphoid structure II > 2 LN regions on the same side of diaphragm (No. of LNs indicated by a subscript e.g. II 2 ) IIILN regions or lymphoid structures on both sides of the diaphragm –III1splenic hilar, celiac, or portal LNs –III2PALN, iliac, mesenteric LNs IV> 2 extranodal sites
 IIILN regions or lymphoid structures on both sides of the diaphragm –III1splenic hilar, celiac, or portal LNs –III2PALN, iliac, mesenteric LNs IV> 2 extranodal sites.")
15
Lymphoma Stage A: no symptoms B: fever, night sweating, BW loss (any one) X: bulky disease –Mediastinal mass > 1/3 of maximum transverse chest diameter –LN > 10cm E: single extranodal site (contiguous or proximal to a known LN stie)
 X: bulky disease –Mediastinal mass > 1/3 of maximum transverse chest diameter –LN > 10cm E: single extranodal site (contiguous or proximal to a known LN stie)")
16
A = without symptoms, B = with symptoms including unexplained weight loss 10% in 6 months), unexplained fever, and drenching night sweats
, unexplained fever, and drenching night sweats")
17
Lymph Node Region

18
Gastric Lymphoma Stage

19
SL/CLL Stage

20
Principles of NHL Treatment Low risk –Stage I, IIC/T + R/T –Stage III, IVobservation, C/T Intermediate~ high grade –Stage I, IIC/T + R/T –Stage III, IVC/T

21
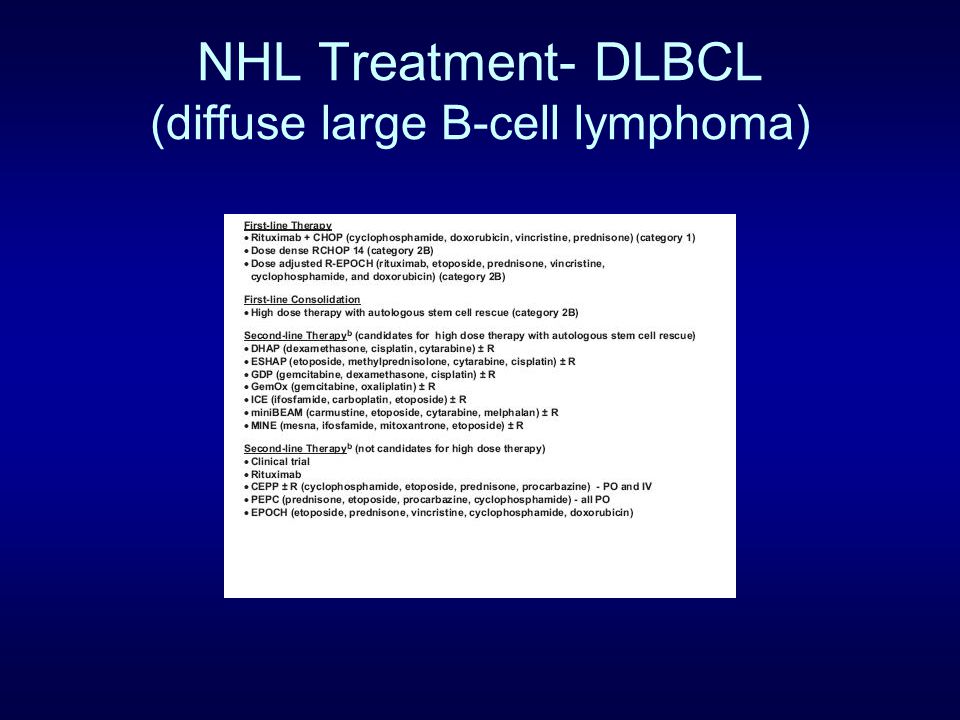
NHL Treatment- DLBCL (diffuse large B-cell lymphoma)
")
23
NHL Treatment- DLBCL IPI 5ys: score 0-1 73%; 2 51%; 3 43%; 4-5 26%

24
NHL Treatment-FL

25
NHL Treatment-FL (follicular lymphoma)
")
26
NHL Treatment-FL Median survival 8-10y

27
NHL Treatment- Margional Zone Lymphoma

28
Median survival 10y

29
NHL Treatment-MCL (Mantle Cell Lymphoma)
")
30
NHL Treatment-MCL Median survival 3-5y

31
NHL Treatment-SL/CLL (small lymphocytic lymphoma)
")
32
NHL Treatment-SL/CLL Median survival: 10 y

33
NHL Treatment-Burkitt Lymphoma

34
NHL Treatment-PTL

36
5 year survival 25%

37
HL Treatmet Prognostic factors

38
HL treatment- Classic HL Stage IA, IIA, nonbulky, cure rate: >90% –C/T (ABVD) + IFRT (category 1) –C/T only (ABVD x 6) (category 2B) Stage I, II, bulky, cure rate >80% Stage III, IV, cure rate 60-70% –ABVD x 4 -> restage -> 2-4 cycles -> observe or IFRT –Stanford V x 3 -> restage + R/T –Escalated BEACOPP (if IPS > 4)
 + IFRT (category 1) –C/T only (ABVD x 6) (category 2B) Stage I, II, bulky, cure rate >80% Stage III, IV, cure rate 60-70% –ABVD x 4 -> restage -> 2-4 cycles -> observe or IFRT –Stanford V x 3 -> restage + R/T –Escalated BEACOPP (if IPS > 4)")
39
Classic HL Treatmet-C/T

40
NLPHL Treatmet I-IIA: IFRT or regional R/T I-IIB: C/T + IFRT III-IVA –C/T + R/T –local R/T –observation (category 2B) III-IVB: C/T + R/T
 III-IVB: C/T + R/T")
41
NLPHL Treatmet-C/T 10 year survival 80%

42
HL Treatmet-R/T

43
PET in lymphoma

44
International Harmonization Project in Lymphoma PET scanning before treatment is recommended only for those lymphomas that are routinely avid for labeled glucose (eg, DLBCL, Hodgkin lymphoma)]. There is not sufficient evidence in support of the use of PET scanning for lymphomas other than DLBCL and Hodgkin Lymphoma. Use of PET for treatment monitoring during a course of therapy should only be done as part of a clinical trial or as part of a prospective registry. PET scanning after completion of therapy should be performed at least three weeks and preferably at six to eight weeks after chemotherapy or chemo-immunotherapy and 8 to 12 weeks after radiation or chemoradiotherapy. Mediastinal blood pool activity is recommended as the reference background activity to define PET positivity for a residual mass ≥2 cm in greatest transverse diameter, regardless of location. A smaller residual mass or a normal sized lymph node (ie, ≤1 x 1 cm in diameter) should be considered positive if its activity is above that of the surrounding background. There is no role for the use of PET to follow patients in remission. JCO 2007 25;571-8
![International Harmonization Project in Lymphoma PET scanning before treatment is recommended only for those lymphomas that are routinely avid for labeled glucose (eg, DLBCL, Hodgkin lymphoma)].](http://images.slideplayer.com/14/4337549/slides/slide_44.jpg "There is not sufficient evidence in support of the use of PET scanning for lymphomas other than DLBCL and Hodgkin Lymphoma. Use of PET for treatment monitoring during a course of therapy should only be done as part of a clinical trial or as part of a prospective registry. PET scanning after completion of therapy should be performed at least three weeks and preferably at six to eight weeks after chemotherapy or chemo-immunotherapy and 8 to 12 weeks after radiation or chemoradiotherapy. Mediastinal blood pool activity is recommended as the reference background activity to define PET positivity for a residual mass ≥2 cm in greatest transverse diameter, regardless of location. A smaller residual mass or a normal sized lymph node (ie, ≤1 x 1 cm in diameter) should be considered positive if its activity is above that of the surrounding background. There is no role for the use of PET to follow patients in remission. JCO ;")
Similar presentations









>")










i.>")




