Download presentation
Presentation is loading. Please wait.

1
Early Intervention System of Payment (EISOP) Service Coordinator Training Revised December 2013
 Service Coordinator Training Revised December 2013")
2
What is EISOP? Ohio Help Me Grow Program established the EI System of Payment (EISOP) in 2005 in accordance with the Individuals with Disabilities Education Act (IDEA P.L. 108-446) Part C. The EI System of Payment: Determines a parent’s ability to pay for specialized EI Services; and Identifies providers who agree to follow Early Intervention and federal and state rules.(Ohio Revised Code rule 3701-08-10 and the EISOP Policy)
 in 2005 in accordance with the Individuals with Disabilities Education Act (IDEA P.L ) Part C. The EI System of Payment: Determines a parent’s ability to pay for specialized EI Services; and Identifies providers who agree to follow Early Intervention and federal and state rules.(Ohio Revised Code rule and the EISOP Policy).")
3
Training Objectives By the end of this training the participant will: Be aware of when it is appropriate to apply for the E.I. System of Payment Know how to complete the application and accompanying forms Provide accurate documentation to request payment for early intervention

4
Who is eligible for EI payment system? Families with children determined eligible for HMG/Part C. This includes children with: – A developmental delay – A diagnosed physical or mental condition that results in a high probability of delay – Financial eligibility is based on 185% of Poverty (the same as BCMH’s financial guidelines)
.")
5
Financial Eligibility Families who report a household income over 185% of poverty have the opportunity to participate in the EISOP Cost Share Option 5

6
The Cost Share Option Families who do not meet eligibility and receive a denial letter may qualify for the Cost Share Option. The cost share is the amount that families pay out of pocket for the entire family before they qualify for EISOP. The family can submit expenses that occur 12 months prior to the date of application through 12 months after the date of application or the child’s 3 rd birthday, whichever comes first.

7
The Cost Share Option Submission of Paid Expenses Include Expenses From 12/17/2012 Include Expenses From 12/17/2012 Include Expenses To 12/17/2014 Include Expenses To 12/17/2014 Application Date 12/17/2013 Application Date 12/17/2013

8
The Cost Share Option Non-reimbursable paid medical expenses incurred by household members will count toward the cost share The cost share is the amount that families pay out of pocket before they qualify for EISOP The family will receive a financial worksheet that indicates the amount required to meet the cost share

10
Cost Share Option Steps Step One- The family should review the income calculations on the financial worksheet received with your denial letter. Step Two - The family should submit verification on non- reimbursable paid medical, dental, vision and early intervention services expenses on the expense form. Step Three –The Ohio Department of Health will review the information and recalculate to see if eligibility is met.

12
Cost Share Option Remind Families: The date of application will be located in the denial letter. Verification must be sent on all items over $100. Receipts, credit card statements, bank statements are all forms of verification. Blackout any account numbers and any other information not pertinent. Questions may be directed to the Early Intervention System of Payment manager by calling (614) 644-8389.
")
13
Summary of the Cost Share Option Steps Family receives a denial letter due to income. The Family submits paid non- reimbursable medical expenses to ODH ODH mails Letter of Approval to Family and Service Coordinator ODH mails Letter of Approval to Family and Service Coordinator ODH conducts a financial review Family meets the cost share amount.

14
What are EI Services/Covered Services? The following services are designed to meet the developmental needs of each eligible child and family : – Assistive Technology Services/Devices(AT) – Audiology Services – Family Training, counseling and home visits – Health Services – Medical Services – Nursing Services – Nutrition Services(Nutr) – Occupational Therapy (OT) – Physical Therapy (PT)
 – Audiology Services – Family Training, counseling and home visits – Health Services – Medical Services – Nursing Services – Nutrition Services(Nutr) – Occupational Therapy (OT) – Physical Therapy (PT).")
15
What are Specialized Services/Covered Services? – Psychological Service (Psy) – Service Coordination Services – Social Work Services – Special Instruction – Speech-Language Pathology (ST) – Vision Services – Other Services : Aquatic Therapy Applied Behavior Analysis )
 – Service Coordination Services – Social Work Services – Special Instruction – Speech-Language Pathology (ST) – Vision Services – Other Services : Aquatic Therapy Applied Behavior Analysis ).")
16
Services NOT Covered by the EI System of Payment Transportation: County programs are responsible for finding resources. Medical Services: Well child and sick visits, immunizations,hospitalizations, prescriptions, surgery, etc. 16

17
Before Submitting an Application…. IFSP The IFSP Team determines a service is needed to reach an outcome in section six (VI) of the IFSP IFSP The IFSP Team determines a service is needed to reach an outcome in section six (VI) of the IFSP
 of the IFSP IFSP The IFSP Team determines a service is needed to reach an outcome in section six (VI) of the IFSP.")
21
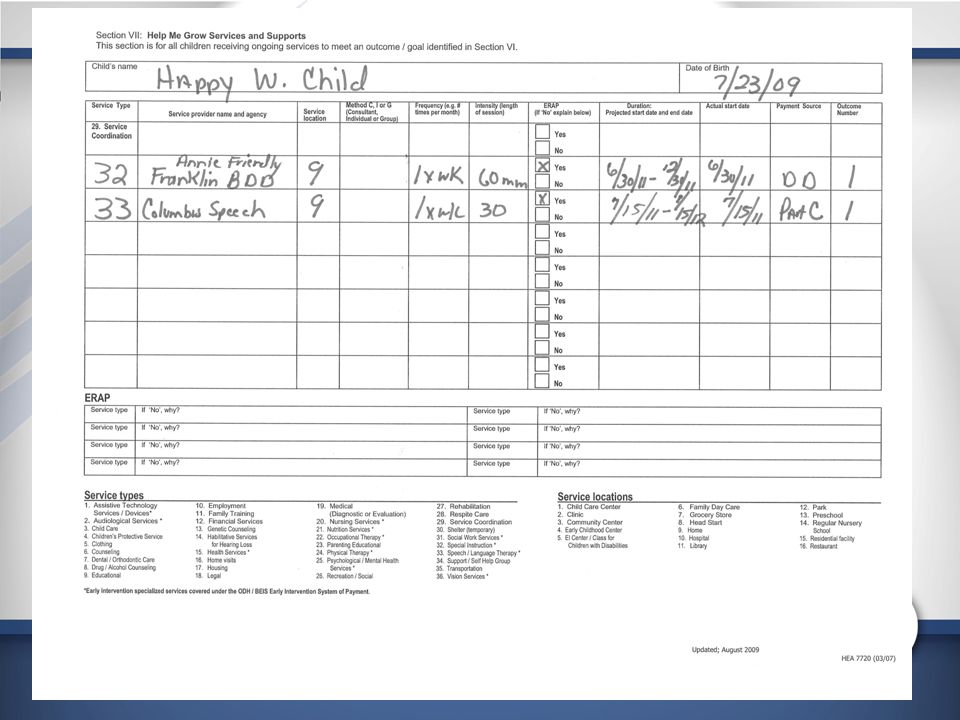
Before Submitting an Application…. The Service is also written on Section Seven (VII) of the IFSP
 of the IFSP")
23
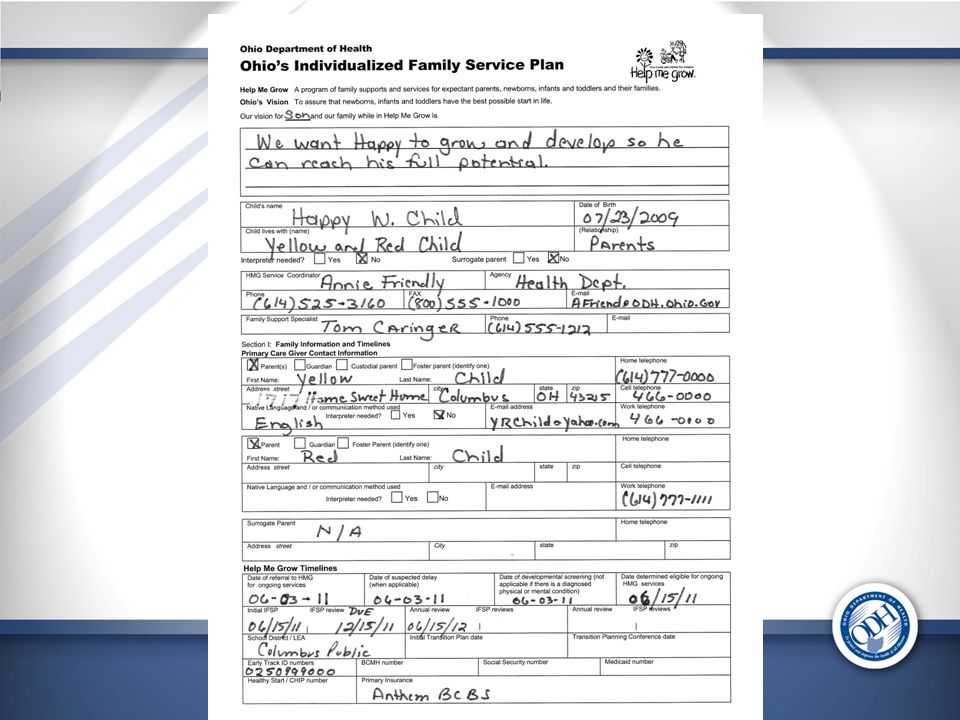
Submit the following sections of The Individualized Family Service Plan (IFSP) Sections I Section 2 Section 6 Section 7 Section 10 ***Also send a copy of the evaluation and assessment
 Sections I Section 2 Section 6 Section 7 Section 10 ***Also send a copy of the evaluation and assessment")
25
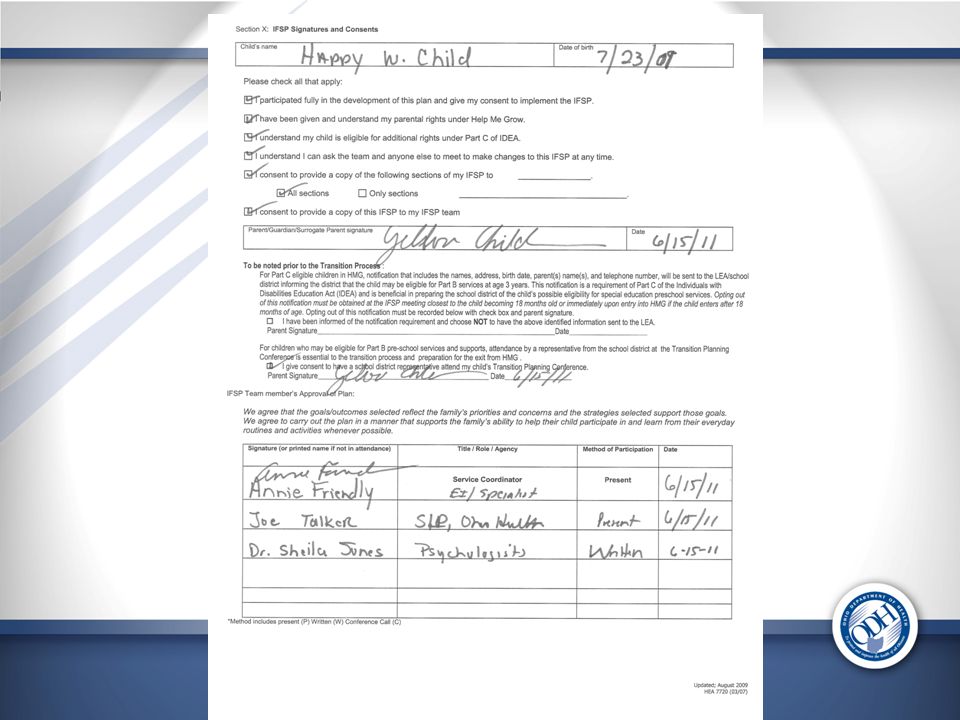
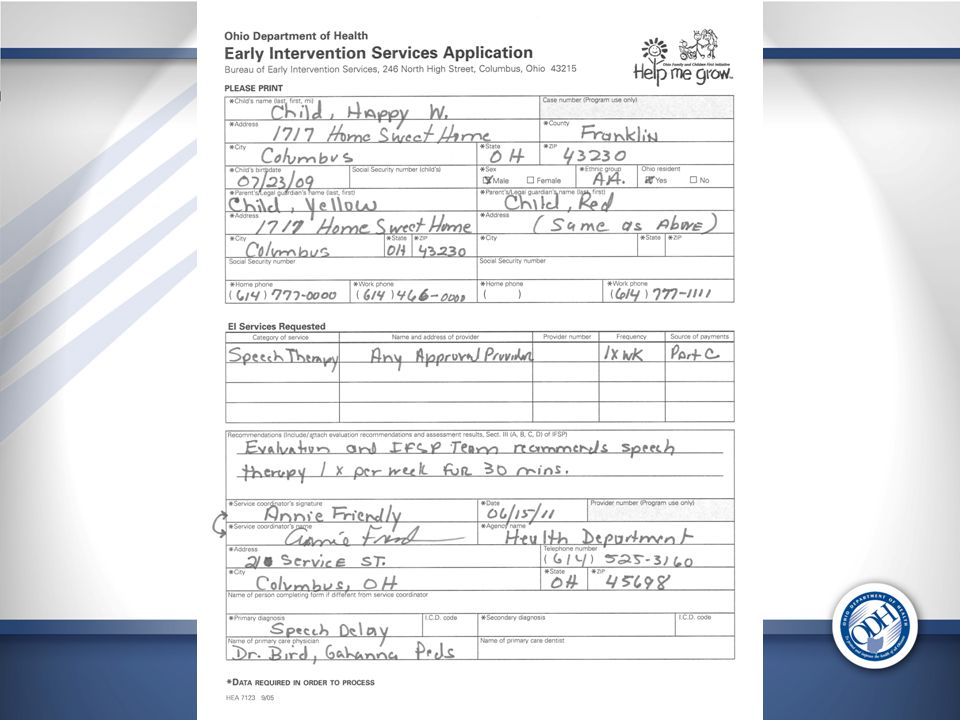
Completing the Application Applications must be sent in the mail. We need original signatures for the following forms: 1.Early Intervention Services Application (two pages) 2. Parent Consent Form. 3. Service Not Available Certification Form. 4.Use of Insurance Inability to Pay Form (If applicable).
 2. Parent Consent Form. 3. Service Not Available Certification Form. 4.Use of Insurance Inability to Pay Form (If applicable)..")
31
Use of Insurance A family may use their insurance to pay for E.I. Services They may also elect to use their insurance and request that the System of Payment cover the co-pays and/or co-insurances

32
Use of Insurance Families may also request that insurance not be billed at all and that the System of Payment cover all approved early intervention services These families must complete the “Use of Insurance Inability to Pay Form”

34
Provide Documentation of The Service Requested Provide a copy of the developmental evaluation or developmental assessment (re report form) that includes recommendations on the service requested: The early intervention service requested (ex: speech therapy) The frequency of the service – How often (ex: weekly) The intensity of the service – The length of the session if applicable (30 minutes) The duration of the service – How long (ex: 6 months)
 that includes recommendations on the service requested: The early intervention service requested (ex: speech therapy) The frequency of the service – How often (ex: weekly) The intensity of the service – The length of the session if applicable (30 minutes) The duration of the service – How long (ex: 6 months)")
35
Completing Financial Portion of the Application This section can be completed by the Service Coordinator along with the family, or the family may submit this directly to ODH

36
Completing Financial Portion of the Application Families Receiving WIC (Women, Infants and Children – nutritional program) If the family receives WIC and does not receive Medicaid, or receives WIC and is applying for a service not covered by Medicaid, submit the WIC verification letter or proof of WIC eligibility. No other financial documentation is required for families in this category.

37
Completing Financial Portion of the Application Submit the completed Combined Programs Application Submit 1 month of check stubs, or a letter from the employer on company letterhead verifying the gross monthly wages. Submit the first two pages of the most recent Federal tax form 1040. If the family is self-employed, submit the IRS 1040 with a copy of Schedule C.

39
Completing the Application Applications must be sent in the mail. We need original signatures for the following forms: 1. The two page Early Intervention Services Application. 2. Parent Consent Form. 3. Service Not Available Certification Form. 4. Use of Insurance Inability to Pay Form (If applicable).
..")
40
Reminders Please make sure all required data is filled out on page one of the EISOP application. For example the child’s diagnosis, the date and the Service Coordinator’s contact information List the services requested along with the provider and the frequency and source of payment which is “Part C” On page two indicate if child is Medicaid Eligible

41
Reminders Please make sure the provider is an APPROVED EISOP provider/or is actively trying to become one Please do not send in the following items: Birth certificates Drivers licenses Ask the family if they receive WIC

42
Summary of the Application Process SC is notified that application was received. Application reviewed for service approval SC submits application to ODH via mail ODH Reviews for Financial Eligibility Letter of Approval is mailed to Family and Service Coord. Family Selects a provider for the approved listing Child receives E.I. service (s) Family presents LOA to Provider Provider bills the Ohio Dept. of Health
 Family presents LOA to Provider Provider bills the Ohio Dept. of Health.")
43
The Letter of Approval LOA

46
Requesting Additional Services Reminders Remind the family to contact their Service Coordinate if you and the team determine to increase the services or the child needs an additional Early Intervention Services All services must be included on the Letter of Approval before the provider can bill the Ohio Department of Health to receive reimbursement for services.

48
Requesting Additional Services After an application is approved, a child may need an additional service covered or an increase in the number of units approved for a service.

49
Requesting Additional Services After an application is approved, a child may need an additional service covered or an increase in the number of units approved for a service. Step One- The Service Coordinator obtains written documentation from the EI Service Provider and IFSP Team verifying the type of service, frequency, intensity and duration. Step Two - An IFSP Review is completed to see how this will help meet the outcomes or a new outcome is written.(Section VI) Step Three- The service is added to section seven (VII) of the IFSP
 Step Three- The service is added to section seven (VII) of the IFSP.")
50
Requesting Additional Services Step Four- The Service Coordinator completes the “Request For Payment of Additional Early Intervention Services” Form. Step Five- The Service Coordinator submits the following to the Ohio Department of Health: 1.Request For Payment of Additional Early Intervention Services” Form 2.Section six (VI) of the IFSP 3.Section seven (VII) of the IFSP 4.Documentation from the provider of the need for additional services.
 of the IFSP 3.Section seven (VII) of the IFSP 4.Documentation from the provider of the need for additional services..")
51
Forms are located on the Help Me Grow Website www.helpmegrow.ohio.gov Look under the professional tab Click on the Early Intervention System of Payment Go to EISOP Forms

52
Assistive Technology (AT) Requests The AT request must relate to an outcome on the child’s IFSP and be supported by the IFSP Team ( IFSP Section 6) Section 7 of the IFSP must be completed The request must include recommendations from the Therapist/EI Service Provide An estimate from the vendor on the costs of the device Prior Authorization is required on all AT requests Contact the Bureau prior to purchasing or leasing assistive technology devices Submit the Assistive Technology Request Form
 Requests The AT request must relate to an outcome on the child’s IFSP and be supported by the IFSP Team ( IFSP Section 6) Section 7 of the IFSP must be completed The request must include recommendations from the Therapist/EI Service Provide An estimate from the vendor on the costs of the device Prior Authorization is required on all AT requests Contact the Bureau prior to purchasing or leasing assistive technology devices Submit the Assistive Technology Request Form")
54
Assistive Technology (AT) Requests The System of Payment will not cover the following: AT items for a child age 33 months or older Items that do not relate to the outcome on the child’s IFSP Medical Items: Eye glasses, Hearing Aides, Wheel chair. Items purchased over the counter

55
Submitting the application to ODH Mail the original application, forms and documents to: Ohio Department of Health BCDSHN - EI System of Payment 246 North High Street, 5 th Floor Columbus, OH 43215

56
Questions? Contact the Bureau for Children with Developmental & Special Health Needs at (614) 644-8389 We will gladly walk you through the process!
 We will gladly walk you through the process!.")
Similar presentations
















>")













 is intended to help students with disabilities interact with the same content.>")