Download presentation
Presentation is loading. Please wait.

1
TB AND HIV/AIDS THE SITUATION AT BMC Care & Treatment Unit CME, 5/5/20166 PRESENTERS: Dr. Desideris Bernard, Dr. Magawa

2
INTRODUCTION

3
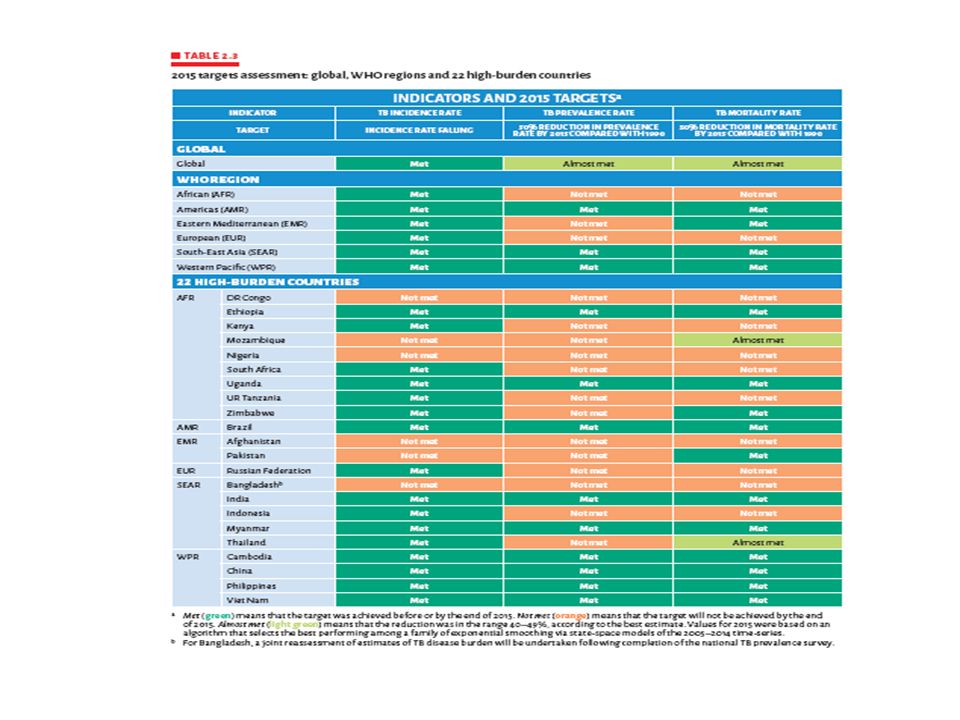
TB/HIV Global situation TB and HIV have been declared as global emergencies demanding global attention(NACP,2015) Worldwide, 34.3 million people are living with HIV. Of these, 24.5 million (71%) live in sub-Saharan Africa and approximately one third are co-infected with TB Globally in 2014, there were an estimated 9.6 million incident cases of TB: 5.4 million among men, 3.2 million among women and 1.0 million among children. Of those who suffer TBs-related mortality, 31% are HIV-infected Some countries have documented up to 70% of TB patients are HIV positive.
 live in sub-Saharan Africa and approximately one third are co-infected with TB Globally in 2014, there were an estimated 9.6 million incident cases of TB: 5.4 million among men, 3.2 million among women and 1.0 million among children. Of those who suffer TBs-related mortality, 31% are HIV-infected Some countries have documented up to 70% of TB patients are HIV positive..")
4
.

5
.

6
Tanzania and the burden of TB/HIV In Tanzania, TB cases have increased six-fold from 11,843 in 1983 to 64,267 in 2009, mainly due to HIV/AIDS. About 37% of TB patients in Tanzania are co-infected with HIV, accounting for 60-70% of the increase in the number of TB patients. About 41.5% of new TB patients present with smear positive pulmonary tuberculosis (PTB+) and 36.2% with smear negative pulmonary tuberculosis (PTB-) and 22.3% presented with ETB in 2009
 and 36.2% with smear negative pulmonary tuberculosis (PTB-) and 22.3% presented with ETB in")
8
INTERACTION OF TB & HIV HIV -↑number of TB cases and alters the clinical course of TB disease. As HIV infection progresses → CD4+ T- lymphocytes decline in number and function. Thus, the immune system becomes less able to prevent the growth and local spread of M. tuberculosis The most common types of TB in HIV are disseminated and extra pulmonary TB

9
TB/HIV IN THE MEDICAL WARDS In the US, HIV clients accounts for 22% of re- admission (59% higher than non-HIV cases) but TB/HIV is <1% in the medical wards. TB/HIV co-infection lead to prolonged hospital stay and significantly affect the economic status of clients (especially MDR TB –av. 6826 USD per person globaly). A study at MNH medical wards, TB/HIV was reported the major cause of morbidity (27.9%) and mortality (39.6%) [Desderius BM, Munseri P, Pallangyo KJ 2015]
. A study at MNH medical wards, TB/HIV was reported the major cause of morbidity (27.9%) and mortality (39.6%) [Desderius BM, Munseri P, Pallangyo KJ 2015].")
10
EFFORTS TO REDUCE BURDEN OF TB ART initiation -Once the diagnosis of TB is made in PLHIV, Start TB Rx within 2 weeks(WHO, 2014) Three I’s o Intensive case finding o Infection control o IPT
 Three I’s o Intensive case finding o Infection control o IPT")
11
Three I’s Intensive case finding – Based on TB screening tool To increase the yield of confirmed cases from TB suspects/presumptive TB cases Infection control – Each POC should take precautions to protect HCWs from acquiring TB and establish IC plans at each POC.

12
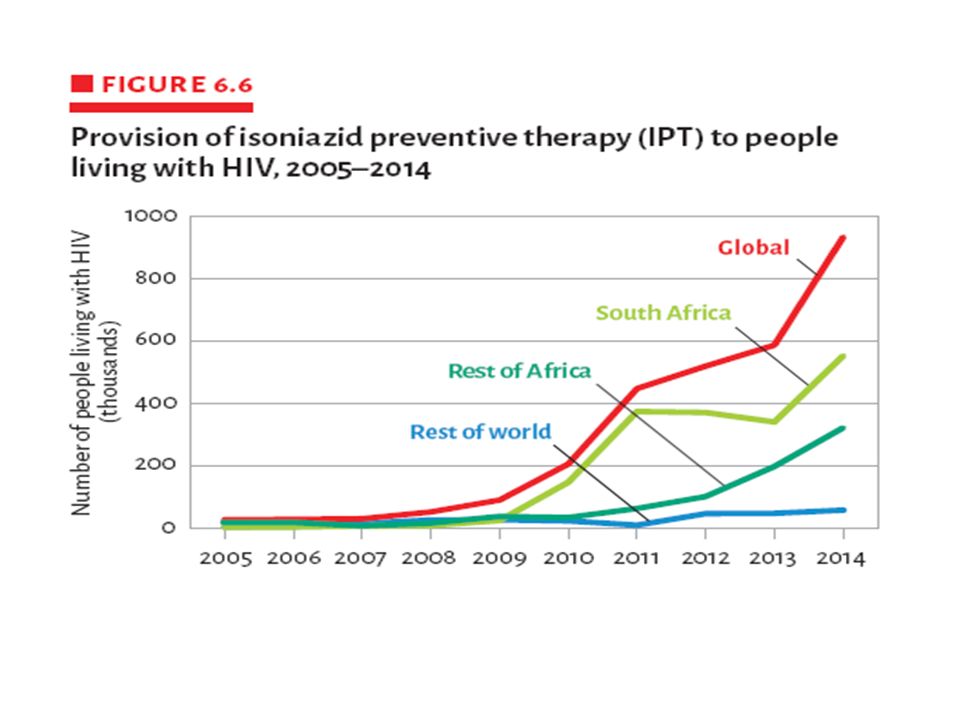
IPT

14
IPT PROVISION AT BMC IPT Started July 2011 Total clients given IPT - 3,428 (Clients on care – 14,732, Not on ART -5,355)
")
15
TB/HIV Co-treatment challenges Concurrent treatment of tuberculosis and HIV is complicated by:- o the adherence challenges of polypharmacy o overlapping side effect profiles of anti-TB and antiretroviral drugs, o immune reconstitution inflammatory syndrome (IRIS), and o drug-drug interactions
, and o drug-drug interactions")
16
HIV/TB SITUATION AT BMC

17
At BMC,We are focused and working hard to fight TB through several activities: EDUCATION Clients:health talk,posters,??Audiovisual TBtrasmission:Airborne,m.tuberculos Risk factors:Time,burden,sunlight,ventilation Staff:TBIC

18
SCREENING OF ACTIVE TB TB screen tool:(a) cough of any duration (b) fever of any duration (c) excessive night sweats (d) loss of weight >3kg/1mo Sites:CTC Clinic,VCT,PMTCT,OPDs,Wards,EMD Cough registers
 cough of any duration (b) fever of any duration (c) excessive night sweats (d) loss of weight >3kg/1mo Sites:CTC Clinic,VCT,PMTCT,OPDs,Wards,EMD Cough registers")
19
ISONIAZID PREVENTIVE THERAPY(IPT) Tab 300mg OD of INH for 6months. Repeat after every 2years Eligibility: (a) no current/past h/o hepatitis (b)no h/o of TB Treatment in the past 2 years (c) no non-adherence to long term treatment
 no current/past h/o hepatitis (b)no h/o of TB Treatment in the past 2 years (c) no non-adherence to long term treatment.")
20
(d) no alcohol abuse (e)any medical contraindication to INH (f) no symptoms of peripheral neuropathy TB INFECTION CONTROL (A)Admistrative measures: TBIC plan: well-ventilated waiting area,consultation room Ensure turn around time of sputum smear,G- Expert in 24hours orientation of all staff on TBIC measures
 no alcohol abuse (e)any medical contraindication to INH (f) no symptoms of peripheral neuropathy TB INFECTION CONTROL (A)Admistrative measures: TBIC plan: well-ventilated waiting area,consultation room Ensure turn around time of sputum smear,G- Expert in 24hours orientation of all staff on TBIC measures")
21
(B)Environmental measures Open windows and doors Fans Collect sputum outside and away from other people Isolation of TB suspects Isolation of TB patients in the ward
Environmental measures Open windows and doors Fans Collect sputum outside and away from other people Isolation of TB suspects Isolation of TB patients in the ward")
22
(C)Pesornal Protection Provide handkerchiefs/tissues for all coughing patients Use of mask N95 Reduce time of staying with TB presumptive or active TB Cases
Pesornal Protection Provide handkerchiefs/tissues for all coughing patients Use of mask N95 Reduce time of staying with TB presumptive or active TB Cases")
23
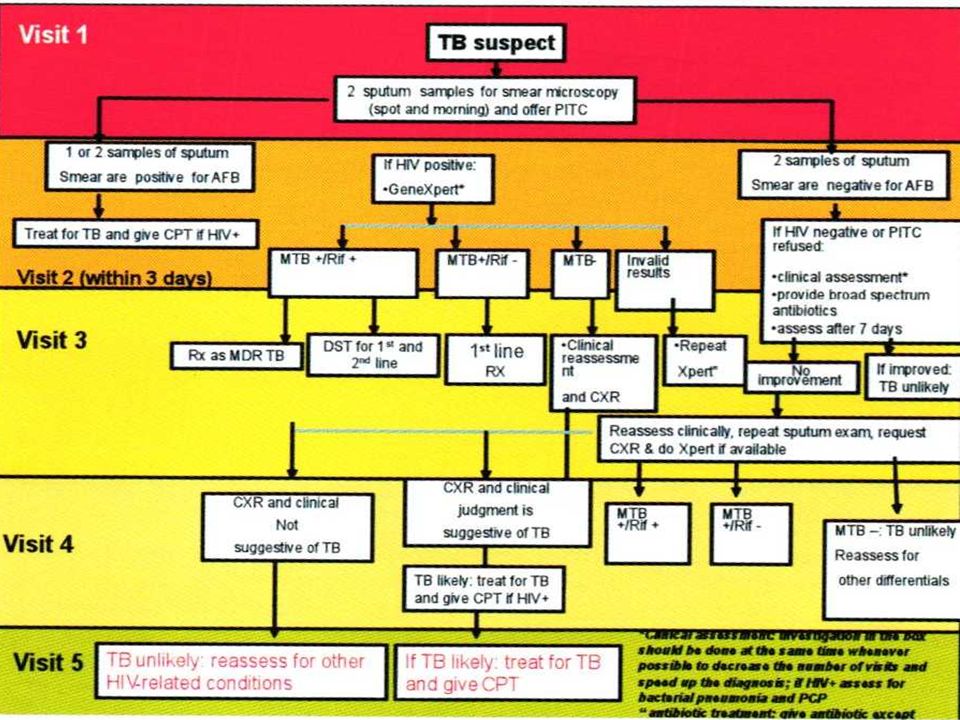
DIAGNOSIS Smear Microscopy GeneXpert Solid Culture

25
Test statistics (2015): Tb laboratory register Total smears: 2100 Smear positivity 6.1% Follow up positivity 1% Low grade AFB: 1%
: Tb laboratory register Total smears: 2100 Smear positivity 6.1% Follow up positivity 1% Low grade AFB: 1%")
26
Test statistics(2015): Tb Culture register Smear pos/Culture pos: 55 ( 37%) Smear neg/Culture pos 5 (3.3%) Smear neg/Culture neg: 43 (29%) Smear pos/Culture neg:37 (25%)
: Tb Culture register Smear pos/Culture pos: 55 ( 37%) Smear neg/Culture pos 5 (3.3%) Smear neg/Culture neg: 43 (29%) Smear pos/Culture neg:37 (25%)")
27
Test statistics(2015): GeneXpert Total GeneXpert1252 MTB Not detected (N)1073 MTB detected /Rif neg(T)70 MTB detected / Rif detected ( RR)4 MTB detected/ Rif Indeterminate (I)7 Error23 Invalid63 No result5
: GeneXpert Total GeneXpert1252 MTB Not detected (N)1073 MTB detected /Rif neg(T)70 MTB detected / Rif detected ( RR)4 MTB detected/ Rif Indeterminate (I)7 Error23 Invalid63 No result5")
28
Results feedback and reports Results of AFB Smears and GeneXpert released to requesting clinician within 24 hours. Critical results have been identified and are immediately communicated to clinician. If RR in addition to clinician RTLC is informed Customer satisfaction survey of January 2016 does not show negative statements or complaints for AFB smears or GeneXpert

29
TREATMENT For new TB/HIV Patients, start ART within two weeks of antTBRX All TB Patient should start ART regardless of CD4 count Initiate co-trimoxazole prophylaxis to all PTB patients regardless of CD4 count Drug-drug interaction:Nevirapine and atazanavir

30
Regimes New adult 2RHZE/4RH All retreatment and defaulters 2RHZE/1RHZE/5RHZE Rifampicin resistant MDRTB RX

31
DOT -Treatment supporter -DOT Nurse or HCW

32
Trends of TB at BMC, 2014-2016 TB AMONG NON-HIV

33
BMC Trends of TB/HIV co-Infection

34
Trends of Types of TB/HIV co-infection 2015

35
Annual Trends for types TB in HIV 2015/2016

36
WAY FOWARD

37
THE FUTURE OF BMC ON TB Dx & Rx Capacity building for TB culture o Microscopy -AFB o Gene expert/RIF o ?Line probe assay o ?DST o ?LAM test o ?ADA test Establishment of MDR centre - MOH has appointed BMC as one of MDRTB Initiation site (once negative pressure is established)
")
38
WABEJA!

Similar presentations


















: Relevance for neurological infections Lucie Jean-Gilles.>")
