Download presentation
Presentation is loading. Please wait.

1
Screening for Abuse & Violence in Fairfax County Partnership for a Healthier Fairfax’s IPV/SA Screening Action Group Spring 2016

2
Training Origins Partnership for a Healthier Fairfax Community Health Improvement Plan: “Implement Evidence-based behavioral health screenings and make appropriate referrals in health care provider offices, schools, and other settings.” Creation of the Intimate Partner Violence/Sexual Assault (IPV/SA) Screening Action Group Mission: Equip medical professionals with the education and resources to better screen for domestic and sexual violence experienced by their patients. The Action Group is comprised of: Fairfax County Office for Women & Domestic and Sexual Violence Services (OFWDSVS) Fairfax County Domestic Violence Action Center (DVAC) Fairfax County Health Department Inova Fairfax Hospital’s FACT (Forensic Assessment and Consultation Team) Department Inova Social Work program
 Fairfax County Domestic Violence Action Center (DVAC) Fairfax County Health Department Inova Fairfax Hospital’s FACT (Forensic Assessment and Consultation Team) Department Inova Social Work program.")
3
3 Taking Care of Ourselves

4
Learning Objectives Differentiate and define domestic violence, sexual violence, stalking, human trafficking and strangulation Discuss the prevalence of these crimes in our Fairfax County community Describe the administration of the Abuse Assessment Screen Explain safety planning and options counseling Identify available resources for clients

5
Possible Introductory videos? https://www.youtube.com/watch?v=xWrCoQMCvq0 https://www.youtube.com/watch?v=xWrCoQMCvq0 https://www.youtube.com/watch?v=1T-z_sX_QNc https://www.youtube.com/watch?v=1T-z_sX_QNc https://www.youtube.com/watch?v=SAKgylmFMy0 https://www.youtube.com/watch?v=SAKgylmFMy0 https://www.youtube.com/watch?v=JaB7XJk8fwg https://www.youtube.com/watch?v=JaB7XJk8fwg

6
Prevalence - National Statistics 1 in 4 Women & 1 in 7 Men have experienced severe physical violence by an intimate partner Women, young women, racial/ethnic minorities are disproportionately impacted Women account for 84% of spouse abuse victims; 86% of victims of abuse at hands of boyfriend/girlfriend More than 3 Women and 1 Man are killed by their intimate partners everyday 1 in 6 Women & 1 in 33 Men have experienced an attempted or completed rape

7
Prevalence - National Statistics 1 in 6 Women & 1 in 19 Men will experience stalking in their lifetime 1 in 3 adolescents is a victim of physical, sexual, emotional or verbal abuse from a dating partner 7.7% of women and 3.0% of men will be strangled in their lifetime ADD HT STAT

8
Prevalence - Fairfax County Every Month: Domestic Violence hotlines receive over 200 calls Victims request 53 family abuse protective orders 16 families escape to an emergency domestic violence shelter Over 160 family abuse arrests are made Domestic Violence is a leading cause of homicide in Fairfax County

9
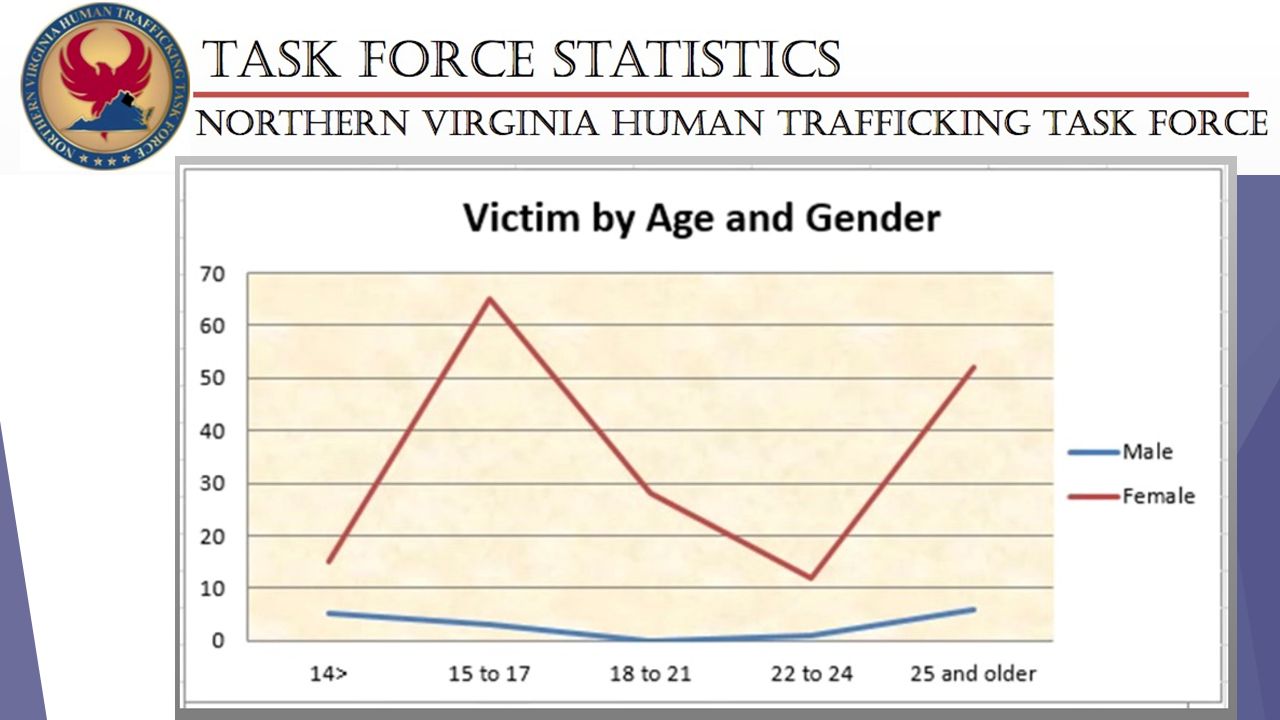
Prevalence - Fairfax County 397 Sex Offenses Reported by FCPD in Calendar Year 2015 68% of sex offenses are NOT reported to law enforcement (RAINN) ~800 additional sex offenses NOT reported in Fairfax County that year Between Oct 2013 – Jul 2015, Northern Virginia Human Trafficking Task Force received 102 adult and 90 teen sex trafficking leads ~5 adult leads/month ~4 teen leads/month In the first 6 months of county’s Lethality Assessment Program, 68% of 291 high-danger victims reported a history of strangulation
 ~800 additional sex offenses NOT reported in Fairfax County that year Between Oct 2013 – Jul 2015, Northern Virginia Human Trafficking Task Force received 102 adult and 90 teen sex trafficking leads ~5 adult leads/month ~4 teen leads/month In the first 6 months of county’s Lethality Assessment Program, 68% of 291 high-danger victims reported a history of strangulation")
10
The Facts on Health Care and Domestic Violence The costs of intimate partner violence exceed $5.8 billion each year, $4.1 billion of which is for direct medical and mental health care services. 81% of women and 35% of men who experienced IPV reported at least one health-related or other impact Both women and men with lifetime victimization experience were significantly more likely to report: Frequent headaches Chronic pain Difficulty sleeping Activity limitations Self-assessed poor physical and mental health

11
The Facts on Health Care and Domestic Violence Homicide is a leading cause of traumatic death for pregnant and postpartum women A study found that 44% of victims of domestic violence talked to someone about the abuse – 37% of those talked to their health care provider. Four different studies of survivors of abuse: 70% to 81% of the patients reported that they would like their healthcare providers to ask them privately about intimate partner violence

12
Direct and Indirect Effects on Health Short and long-term physical and mental health effects IPV can result in unintended pregnancies Witnessing IPV in childhood is 1 of 10 adverse childhood experiences linked to negative health Witnessing violence increases mental health impact to a greater degree than direct physical abuse

13
Importance of screening in Health Care Settings Provides a unique opportunity to identify patterns of violence and prevent future harm Trusting relationships, confidentiality, and space away from the abuser Growing consensus recommending routine IPV screening The Joint Commission on the Accreditation of Hospitals and Health Care Organizations American Medical Association American Congress of Obstetrician Gynecologists American Nurses Association U.S. Preventive Services Task Force Potential to improve health outcomes

14
Reasons for Low Screening by Clinicians Barriers reported: time constraints lack of knowledge, education, or training inadequate follow-up resources and support staff discomfort discussing violence and trauma

15
Mandated Reporting The information shared is confidential, however- mandated reporting laws: Child abuse (Va. Code 63.2-1509) Elder abuse (Va. Code 63.2-1606) Current injuries by weapon (Va. Code § 54.1- 2967) Threats to kill self or others (Agency based policies -FCHD has Mental Health Crisis PM)
 Elder abuse (Va. Code ) Current injuries by weapon (Va. Code § ) Threats to kill self or others (Agency based policies -FCHD has Mental Health Crisis PM).")
16
Fairfax County Abuse Assessment Screening Tool Tool screens for power & control issues in a variety of relationships and situations and aims to identify: domestic violence dating violence sexual violence stalking financial control human trafficking reproductive coercion strangulation

17
Agenda Topical Overview Domestic Violence & Stalking Child Witness to Domestic Violence Sexual Violence Human Trafficking Strangulation Working with victimized patients Cultural competency Screening & Documentation Medical Red Flags and Treatment Needs Resources & Safety Planning Scenarios Secondary Trauma

18
Domestic Violence & Stalking

19
Define Domestic Violence, Family Abuse, and Stalking Understand Power & Control and the Dynamics of Domestic Violence and Stalking Recognize Various Types of Abuse Empathize with Counterintuitive Victim Behavior Become more comfortable in working with victims Section Objectives

20
A pattern of coercive behaviors, used by an individual to gain and/or maintain power and control over another individual in the context of an intimate/dating relationship. Domestic Violence

21
When one person uses power to control another person. Domestic Violence

22
Family Abuse (Virginia §16.1-228): Any act involving violence, force, or threat that results in bodily injury or places one in reasonable apprehension of death, sexual assault, or bodily injury and that is committed by a person against such person's family or household member. Such act includes, but is not limited to: Any forceful detention Stalking Criminal sexual assault in violation of Article 7 (§ 18.2-61 et seq.) of Chapter 4 of Title 18.2, or18.2-61 Any criminal offense that results in bodily injury or places one in reasonable apprehension of death, sexual assault, or bodily injury. Several forms of family abuse may not be motivated by coercive control. Family Abuse
 of Chapter 4 of Title 18.2, or Any criminal offense that results in bodily injury or places one in reasonable apprehension of death, sexual assault, or bodily injury. Several forms of family abuse may not be motivated by coercive control. Family Abuse.")
23
Pattern of behavior directed at a specific person that would put a reasonable person in fear Stalking

24
On more than one occasion Engages in conduct directed at another person With the intent to place, or when he knows or reasonably should know that the conduct places that other person in reasonable fear of: Death Criminal sexual assault, or Bodily injury To that other person or to that other person's family or household member is Class one misdemeanor upon first offense Stalking: VA Code (§18.2-60.3)
")
25
Stalking & Domestic Violence 81% of victims stalked by their intimate partner report previous physical assaults by the same offender 3 out of 4 women murdered by their intimate partners had been stalked by that offender at least once in the year prior to the murder

27
Physical Emotional Sexual Children and Abuse Spiritual Verbal and Non-verbal Financial Reproductive Coercion Forms Of Abuse

28
Threats Physical & Sexual Violence Stalking Strangulation Power and Control Wheel

29
Hitting Threats of physical abuse Spitting Biting Slapping Grabbing Pulling/ripping hair Shoving Pushing Rough Play Physical Abuse

30
Name calling Disrespecting partner Degrading the partner Not supportive of the partner (in parenting, etc.) Making the partner feel ‘crazy,’ un-intelligent, less competent, less logical Making partner feel less sensitive than abuser Isolation (family, friends, religion) Using children to continue manipulation Engaging in reckless behavior (driving too fast with partner and kids in car) Emotional Abuse
 Making the partner feel ‘crazy,’ un-intelligent, less competent, less logical Making partner feel less sensitive than abuser Isolation (family, friends, religion) Using children to continue manipulation Engaging in reckless behavior (driving too fast with partner and kids in car) Emotional Abuse")
31
Rape Forced Oral or Anal Sex Forced Masturbation Inappropriate touching Humiliation Forced Prostitution Degradation (forced to watch porn, engage in porn) The ‘marital’ or ‘manly’ right to sex Rough Play sex or sexual activity Withholding sex Sexual Abuse
 The ‘marital’ or ‘manly’ right to sex Rough Play sex or sexual activity Withholding sex Sexual Abuse")
32
Abuser will turn children against mother/father Abuser will involve children in the abuse (all forms) Children may have cognitive and behavioral challenges Children may develop abuser like attitudes towards society (women, teachers, etc.) Children may take roles in family where chaos is present Abuser could continue abuse using numerous systems (court, custody, child support, benefits, housing) Abuser could use CPS as a tool against the victim Using Children
 Children may have cognitive and behavioral challenges Children may develop abuser like attitudes towards society (women, teachers, etc.) Children may take roles in family where chaos is present Abuser could continue abuse using numerous systems (court, custody, child support, benefits, housing) Abuser could use CPS as a tool against the victim Using Children")
33
Using faith as an excuse for abuse Using religious texts as justification for abuse Making fun of partners faith, church, etc. Only allowing partner to attend faith/place of worship of abuser’s choice **This applies to ALL religions** Spiritual Abuse

34
Using facial expressions and body language to threaten partner Slashing throat gesture A ‘look’ and/or action Using ‘props’ to illicit the same type of response that body language would: Cleaning a gun in front of partner Pulling out carving knives Gestures that only the victim/survivor may know what it means—it can be subtle or non-existent to others in the room Non-Verbal Abuse #

35
Allowance Withholding of financial information Will not allow partner to have separate bank accounts Will only allow partner to have joint accounts Running up credit cards, etc. Not paying bills, car notes, mortgage Taking partner’s money (from work, welfare, etc.) Putting every financial statement in her name, then running up credit, ruining credit (abuser then has no accountability) Putting the lease or mortgage in her name Financial #3
 Putting every financial statement in her name, then running up credit, ruining credit (abuser then has no accountability) Putting the lease or mortgage in her name Financial #3.")
36
Isolation Isolation from friends, family members or from others who speak her/his language or are from her/his culture, community or country Not allowing to learn English or not allowing to communicate in a language she/he is fluent in. Being the only person through whom she/he can communicate in English. Intimidation Hiding or destroying important papers or items she/he brought from home Threatening family and friends back home Threatening to do or say something that will shame the family Immigration and DV

37
Using Citizenship or Residency Privilege: Failing to file papers to legalize immigration status/Withdrawing or threatening to withdraw filed papers Controlling the ability to work Forcing to work without documentation Using undocumented status to keep from reporting abuse or leaving with the children Threatening the police will arrest for being undocumented to prevent from reporting the abuse Lying about the laws ( re: children, work, ICE, duty for sex) Immigration and DV
 Immigration and DV")
38
Economic abuse Forcing her to work "illegally" Threatening to report her/him if she/he works "under the table" Not allowing job training or education Forcing her/him to sign papers in English that she/he does not understand -- court papers, IRS forms, immigration papers Harassing her/him at work and risks job loss- may have been very difficult to get with documentation status Immigration and DV

39
What do you think a victim’s intuition should tell her/him about DV? Expected Victim Behavior

40
Minimization of violence Maintaining a Relationship with the Offender Victim’s Anger toward the System Victim Recantation Counterintuitive Victim Behavior

41
Cycle/Spiral of Violence Understanding Counterintuitive Behavior

42
Family, Cultural and Peer Pressure Housing Employment Children Cost-Benefit Analysis of Staying in a Bad relationship Money Love

43
DV survivors may: Lie to you about themselves or partner Lie to the children or, have the children lie to you Recant information if there is fear Protect their partner (despite obvious violence) Be very angry at the system Not be consistent or linear in their descriptions of events; not remember details clearly Appear emotionally detached/flat affect Common Victim Responses
 Be very angry at the system Not be consistent or linear in their descriptions of events; not remember details clearly Appear emotionally detached/flat affect Common Victim Responses")
44
Become familiar with warning signs of violence and what the victim may have experienced Listen for offender cognitive distortions- all the reasons things happened (the victim made me do it, I was justified, it was mutual abuse) Within safety and the protocols of your agency, confidentiality with the DV survivor could mean life or death (if you have information, be careful what you disclose and to who) When reporting information to others (including partner, etc.) be careful not to put the victim in a bad position/further at risk (offenders will seek info from other professionals) How You Can Help
 Within safety and the protocols of your agency, confidentiality with the DV survivor could mean life or death (if you have information, be careful what you disclose and to who) When reporting information to others (including partner, etc.) be careful not to put the victim in a bad position/further at risk (offenders will seek info from other professionals) How You Can Help")
45
Listen to their concerns and treat them seriously (they know the offender better than any of us) Follow through Listen to subtle phrases that we may dismiss as conversation—they may be real threats (“If I don’t do this, he will kill me”) To help the client and family learn that you are not someone who will be pulled into the chaos (set clear but supportive boundaries) Model professional and ethical collaborations with other agencies if you have a release (DVAC, therapists, doctors, schools) Call local resources for guidance, ideas, help with the situation (DVAC or other county and community agencies) How You Can Help
 Follow through Listen to subtle phrases that we may dismiss as conversation—they may be real threats ( If I don’t do this, he will kill me ) To help the client and family learn that you are not someone who will be pulled into the chaos (set clear but supportive boundaries) Model professional and ethical collaborations with other agencies if you have a release (DVAC, therapists, doctors, schools) Call local resources for guidance, ideas, help with the situation (DVAC or other county and community agencies) How You Can Help")
46
Child Witness to Domestic Violence Impact on MH

47
Child Witness to Domestic Violence FIRST IMPRESSIONS

48
Sexual Violence

49
‘Catcalling’ Rape Forced Sodomy Sexual Battery Object Penetration Peeping Tom Forced Exposure to Sexual Acts or Pornography

50
Statistics How often does it happen? 1 in 4 women experience unwanted sexual contact in their lifetime 1 in 9 men experience unwanted sexual contact in their lifetime 1 in 2 transgender individuals are sexual assaulted in their lifetime Every 2 minutes someone in the United States is sexually assaulted.

52
82% of sexual assaults are committed by non-strangers

53
Consent The person you intend to engage in sexual activity with must give affirmative (verbal) consent of their own free will before you begin to engage in that activity. Consent is not valid where someone is pressured, tricked, forced, coerced or convinced to engage in any sexual activity.

54
What is Intimate Partner Sexual Violence? Any unwanted sexual act perpetrated by an intimate partner such as a spouse, partner, boyfriend, girlfriend, or anyone the victim is currently or has previously been in an intimate relationship with.

55
What Does It look like? Use of force, intimation or coercion in sexual activity Insistence on sexual activity when partner is intoxicated or under the influence of drugs Engaging in sexual activity when a partner is physically or mentally unable to give consent Use of violent threats with or without weapons Use of sexually degrading language Birth control sabotage Pressure to terminate or keep a pregnancy

56
What is the impact? Longer lasting trauma Higher levels of physical injury Multiple instances of abuse Inability to report due to dependence on abuser Difficulty defining sexual acts as abuse Greater chance of STI exposure Greater chance of birth control sabotage or forced pregnancy Greater safety concerns Greater feelings of shame or self blame

57
Human Trafficking

58
Human Trafficking= Modern Slavery

59
Human Trafficking The United States Victims Protection Act (TVPA) defines human trafficking as the Recruitment, Harboring, Transportation, Provision, Or obtaining of a person through Force Fraud Or coercion….for the purpose of: 1. Commercial sex acts 2. Labor trafficking- for labor or services for the purpose of subjection, involuntary servitude, debt bondage or slavery

60
ONE OUT OF EIGHT endangered runaway youths is likely a victim of human trafficking. — National Center for Missing and Exploited Children

61
National Human Trafficking Resource Center 2014 Virginia has been consistently ranked the 5th State in the nation with the highest number of calls to the National Human Trafficking Hotline. Let's get our State off this list. Prevention is Awareness. It's Everyone's Job !

62
National Human Trafficking Resource Center 2014 Calls to the (NHTRC) Hotline: 1-888-373-7888 Caller’s type: Medical Professional 339 1.6% (highest = community member 27.9%) Caller’s by location: Virginia 663 3.4% (CA highest 17.9%) Type of case – Sex Trafficking 71.4%
 Hotline: Caller’s type: Medical Professional % (highest = community member 27.9%) Caller’s by location: Virginia % (CA highest 17.9%) Type of case – Sex Trafficking 71.4%")
63
Barriers to Disclosure Fear of harm to their family members Fear of being released back to trafficker Young age and feeling overwhelmed & frightened New to country or area- uncertainty in geographic location Lack of safe options post disclosure Fear of deportation, lack of legal documents, prior record Prior unsuccessful attempts to leave or escape Stigma and shame Language barriers, lack of trusted interpreter Physical or mental illness/disability Inability to speak privately with health care provider Economic reasons

64
What is Human Trafficking? 1) Using force, fraud or coercion to induce someone (adult or minor) to perform labor or services; 2) Using force, fraud or coercion to induce an adult to perform commercial sex; or 3) Recruiting, receiving, transporting or harboring a minor in commercial sex—evidence of force, fraud or coercion not needed. All teen prostitutes are trafficking victims Commercial means receiving anything of value Trafficking does not necessarily involve transporting the victim
 Using force, fraud or coercion to induce someone (adult or minor) to perform labor or services; 2) Using force, fraud or coercion to induce an adult to perform commercial sex; or 3) Recruiting, receiving, transporting or harboring a minor in commercial sex—evidence of force, fraud or coercion not needed. All teen prostitutes are trafficking victims Commercial means receiving anything of value Trafficking does not necessarily involve transporting the victim.")
65
The means of human trafficking FORCE FRAUD COERCION Physical assault Sexual assault Confinement Isolation False employment offer Lying about working conditions Deceit/enticement Threats to life, safety, family Threats involving immigration status or arrest Debt bondage Withholding legal documents Withholding/providing drugs Climate of fear/psychological abuse

66
Trafficking versus Commercial Sex Medical personnel may not be able to differentiate Many adult prostitutes were trafficked at some point or may be in the future Can offer options and information if either sex trafficking or commercial sex is indicated

67
Myth 1: Trafficking does not happen here Numbers difficult to obtain because they are not systematically collected Fastest growing criminal activity worldwide: $32 billion annually, surpassing guns and approaching drugs Virginia has the 6 th highest rate of calls to the national hotline October 2013 – July 2015, Northern Virginia Human Trafficking Task Force received 102 adult and 90 teen sex trafficking leads 2015 survey of Fairfax County teens by the Commission for Women: 9% of teens knew someone coerced into commercial sex

68
Source: National Human Trafficking Resource Center 1-888-373-7888 Map of national trafficking hotline calls from Virginia

69
Importance of Health Care Response Large national study of over 100 sex trafficking survivors published in 2014 found that 88% of survivors reported seeing a health care provider while they were being trafficked.

70
Why is trafficking so big? It’s business: Less risky than drug or gun trafficking “Supply” is easy to find Demand is large and culturally normative High income levels and anonymity in Northern Virginia

71
Myth 2: Sex trafficking only happens to certain categories of people Traffickers tap into any vulnerability—emotional, lack of social system, trapped in a bad situation, etc. Victims in all demographic groups: race, nationality, socioeconomic status, citizenship status, gender, age No area is immune: FCPD reports that there have been teen sex trafficking cases at every Fairfax County high school 72% of Northern Virginia trafficking victims were born in the U.S. Many victims maintain regular school and home life

73
Youth at risk for recruitment Wants more independence Desires consumer goods or basic needs met Has access to a computer Spends part of the day unsupervised Feels misunderstood Keeps secrets Wants a romantic relationship Wants a family or group to belong to Sometimes feels like parents don’t care Testing boundaries

74
Who are the traffickers? All demographic groups Gangs Pimps Businesses Intimate partners Friends Family The trafficker or an accomplice may accompany a victim seeking medical care

76
Myth 3: Manipulating someone into trafficking always happens quickly and violently Manipulation has 3 steps and may take months: Scouting Recruitment Entrapment

77
Shopping malls Metros/bus stops Schools Parties Rec centers Churches Social Media Scouting Traffickers often recruit in public places

78
Recruitment Seduction and coercion Gifts/basic needs Violence and force Isolation and dependence Peer recruitment Parents selling children Blackmail False advertising for modeling etc. Social media

79
Entrapment Traffickers will use drugs, money, violence and threats to keep victims trapped in the lifestyle Many don’t see themselves as victims or don’t know how to get help Victim may believe that if they initially agreed to a situation it cannot be trafficking Effects of psychological trauma support entrapment

80
Myth 4: Victims will self-identify and seek help Barriers to seeking help: Fear of trafficker Fear of systems Does not identify as a victim Love/loyalty for the trafficker Unclear or disjointed memories Lack of alternative living arrangement Frequent change in location Depression Addiction Hard to return to normal life

81
Possible Indicators of Trafficking Individual seems disoriented about the time or location Individual exhibits hyper-vigilance, paranoia, fear, anxiety, depression, submission, nervousness Inconsistencies in story Someone else speaks for them, and does not let him/her speak Someone else pays for the services and controls the money Fear of intervention Indicators of control, monitoring, fear of displeasing

82
Possible Indicators of Trafficking continued New clothes, phones, etc. Evidence of violence Tattoos or branding Inappropriate clothing Use of slang related to prostitution No ID/false ID Lies about their age

83
Strangulation

84
Virginia Code S 18.2-51.6 Strangulation Any person who, without consent, impedes the blood circulation or respiration of another person by knowingly, intentionally, and unlawfully applying pressure to the neck of such person resulting in the wounding or bodily injury of such person is guilty of strangulation, a Class 6 felony. A term of imprisonment not less than 1 year not more than 5 years-or- jail for not more than 12 months and a fine not more than $2500, either or both

85
Strangulation vs Choking Choking is an internal obstruction that lodges in the airway and impairs the ability to get oxygen to the lungs Strangulation may have the same end-result but occurs due to a pressure to the outside of the body compressing essential blood vessels or air passages.

86
Types of Strangulation Manual strangulation- is the result of using hands or arms to put pressure on the outside of the neck. It is the most common type. It occurs in 83% of strangulation cases. (Shield et al 2010) Ligature strangulation- is when the external pressure to the neck is caused by a rope or similar item encircling the neck Hanging- is a form of ligature strangulation which uses the person’s body weight to facilitate compression of the neck Postural strangulation- is when the victim is unable to breathe because of compression of the chest. i.e. assailant sitting on chest. (Faugno et al 2013)
 Ligature strangulation- is when the external pressure to the neck is caused by a rope or similar item encircling the neck Hanging- is a form of ligature strangulation which uses the person’s body weight to facilitate compression of the neck Postural strangulation- is when the victim is unable to breathe because of compression of the chest. i.e. assailant sitting on chest. (Faugno et al 2013).")
87
Brain Physiology The brain needs continuous oxygen delivery to function. It is the most sensitive organ to hypoxia or oxygen deprivation. It needs BOTH blood flow and respiration working together to accomplish oxygen delivery. Disruption of this balance quickly leads to: Symptoms- what a patient feels subjectively Signs- what others can objectively observe

88
Normal anatomy Arteries carry oxygen-rich blood and nutrients to cells Veins carry oxygen-poor blood and cell waste products away from the cells Trachea brings oxygen into the lungs when we inhale where it is absorbed into the blood for use by the cells. Carbon dioxide and other waste products or respiration leave the body through the trachea on exhale.

89
Obstruction of EITHER Circulation OR respiration = Hypoxia or Anoxia Hypoxia is an oxygen deficiency in body tissues Anoxia is absence of oxygen Taber’s Cyclopedic Medical Dictionary 2009

90
How Much Pressure IS That? Dr. Bill Smock, Louisville PD

91
10 seconds to unconsciousness 20 seconds should bounce back on own 30 seconds need to medically revive 50 seconds is point of no return-rarely recover even with CPR Dr. Louis Pena Time is Life!

92
50% with no visible injury 35% with injuries too minor to photograph 15% with injuries sufficient to photograph Strack GB, McClane G, Hawley DA; A review of 300 Strangulation Cases

93
WOW! Talk about Power and Control?!?! Less pressure than a handshake 10 seconds to being rendered incapacitated Near death experience for your victim Accomplished without leaving a mark

94
It IS happening National Violence Against Women Survey found: A lifetime prevalence of strangulation 7.7% of women 3.9% men For any type of offender (Pritchard et al 2015) Study of 62 women in shelter. Avg # strangulations were 5.3.X/ per woman (multiple strangulations increases risk of morbidity and mortality) Average time to FIRST strangle was 3.1yrs (Wilber et al 2001)
 Average time to FIRST strangle was 3.1yrs (Wilber et al 2001).")
95
We NEED to ask…. Start simple… “Did anyone put their hands or anything else around your neck or make it difficult to breathe?” “How did they do that?” “Were you able to breathe or speak while this was happening?” “Tell me about it.” – try to determine what they remember – was their LOC, incontinence? Are you worried for their safety? Does EMS need to respond? “Has this ever happened before?” DID THIS HAPPEN IN THE PREVIOUS 5 DAYS?

96
Physiologic Dangers Immediate dangers: Death from hypoxia or arrhythmia Within the next 24-36 hours: Airway compromise due to swelling of neck Pulmonary edema (up to 2 weeks) Nerve paralysis leading to vocal & swallow issues Arterial spasm, tears or dissection, stroke Depression and PTSD leading to Suicide Up to 20 years later: Stroke from clots or arterial damage
 Nerve paralysis leading to vocal & swallow issues Arterial spasm, tears or dissection, stroke Depression and PTSD leading to Suicide Up to 20 years later: Stroke from clots or arterial damage")
97
Signs & Symptoms of Strangulation Redness to neck Scratch marks Rope burns Thumb print bruising Red eyes Petechiae (tiny red spots) Loss of control over bodily functions Pain to neck/throat Coughing/clearing throat Raspy voice Nausea or vomiting Unconsciousness Ears ringing Head rush Miscarriage Restless/Combative 97 Or….No visible signs at all!
 Loss of control over bodily functions Pain to neck/throat Coughing/clearing throat Raspy voice Nausea or vomiting Unconsciousness Ears ringing Head rush Miscarriage Restless/Combative 97 Or….No visible signs at all!")
98
Symptoms Since signs are often not present- Symptoms become even more essential to document! We need to be able to prove impairment in breathing and circulation and all we may have to do this is SYMPTOMS and the history reported to us. We need to get it accurately, completely and in the patient’s words.

99
Loss of Consciousness Patients may not be aware they had a LOC. When the brain is subject to hypoxia it no longer creates and stores memory- we need to specifically ask: Did you find yourself on the floor or in a different room without remembering how you got there? Do you specifically remember when the strangulation stopped? Considered the most accurate subjective finding correlated to danger to life (Christie et all 2010) LOC= ANOXIA to brain cells
 LOC= ANOXIA to brain cells.")
100
Mental Status Changes Can be the result or PTSD, Brain Anoxia or both Often attributed to the patient being “hysterical”, “intoxicated” or an “exaggerated claim” especially when no outward signs are present. Restlessness and combativeness are common – especially after a LOC Memory loss Insomnia, nightmares Depression and suicide ideation (Smith et al 2001)
.")
101
Incontinence Did you lose your urine or stool while being strangled? It is important to ask – patients will not likely offer this information out of embarrassment and because they don’t understand its significance and will often change before seeking help Urination and defecation are controlled by the sacral nerves of the autonomic nervous system (involuntary body functions). Loss of bowel or bladder = cerebral hypoxia This is a LATE and CONCERNING sign 1944 study: At least 15 seconds of Anoxia for urinary sphincter to relax Even longer for bowel sphincter relaxation (30 seconds) *** Loss of bladder/bowel = prolonged anoxic episode
. Loss of bowel or bladder = cerebral hypoxia This is a LATE and CONCERNING sign 1944 study: At least 15 seconds of Anoxia for urinary sphincter to relax Even longer for bowel sphincter relaxation (30 seconds) *** Loss of bladder/bowel = prolonged anoxic episode.")
102
Petechiae Petechiae are tiny pin point hemorrhages which can be present on the skin, conjunctiva, mucous membranes and on our internal organs including the brain. They result as capillaries rupture from a combination of increased venous congestion and hypoxia. They can disappear in as little as one day. They are NOT specific to strangulation BUT – When present in a history of strangulation – they are considered a life threatening sign! That strangulation was particularly lethal (A.Christe et al. 2010) More common after violent struggle Considered to be “life threatening by themselves due to a considerable decrease in blood circulation” (A.Christe et al. 2010)
 More common after violent struggle Considered to be life threatening by themselves due to a considerable decrease in blood circulation (A.Christe et al. 2010).")
103
NO visible signs….. Does the patient History support occlusion of blood flow or airway? “ Couldn’t breathe” = YES – preventing air entry “Everything went dark” = YES – lack of oxygen to optic nerve “Roar in my ears” = YES – lack of oxygen to auditory nerve “I passed out” = YES – lack of oxygen to brain “I urinated on myself” = YES – prolonged lack of oxygen leading to loss of sphincter control “I lost stool” = YES – even longer to lose bowel sphincter “She was shaking after she passed out” – YES – anoxic convulsion ALL THESE = ANOXIC INJURY

104
Difficult to Prove Victims may be reluctant to participate since many strangulations occur in the DV context The patient may not have a clear recollection of the assault due to the hypoxia and possible LOC Many times the only witness’ to the assault are the victim and the perpetrator Hearsay, in the form of statements to the police at the scene and statements made to obtain restraining order, may be difficult to get admitted into evidence The can have an exam WITHOUT police involvement at NO cost.

105
Strangulation can be the last violent act before homicide.

106
Put risk into perspective Victims of prior attempted strangulation are: 7x or 800% more likely of becoming a homicide victim and 6x or 700% more likely of becoming an attempted homicide victim. (Glass, et al, 2008).
..")
107
Sadly, it is one of the most commonly minimized forms of violence. With increased awareness, better interviewing and documentation by all of us, we can improve victim outcomes, safety and potentially save a life.

108
Strangulation Forensic Exam-document injuries, signs and symptoms of strangulation and can refer to a higher level of care. Symptoms may be delayed. Concerning symptoms include Vision changes/blurred vision or hearing changes Neck pain and/or swelling, pain with swallowing Difficulty breathing and coughing Nausea/vomiting Loss of urine or bowels Hoarseness or voice changes Fainting, headache or loss of memory Anyone who is pregnant REQUIRES evaluation in ED/OBGYN

109
Medical Forensic Evaluation Patient Needs Medical evaluation Crisis intervention Danger assessment Safety Plan Emotional support Resources Follow up instructions Judicial Needs Detailed history of events and symptoms Documentation of physical findings with photography Evidence collection Interpretation of findings Expert testimony

110
Court Testimony… FNEs can give expert testimony as to the seriousness of strangulation when there is the lack of visible marks on the neck. Statements made by patient. Medical Exception to Hearsay Rule. And helping to LINK the specific signs and symptoms, however subtle, to the specific medical terminology of the law.

111
Inova FACT Department 12.5% of our total cases involved strangulation (including suspects, follow ups…) Type of case : 68% IPV/DV 30% SANE 2% Strangulation alone Signs and symptoms : 77% had Signs and symptoms 7% had NO signs or symptoms 16% had signs OR symptoms Jurisdiction : 48% Alexandria 30% Fairfax County – utilizing LAP since July 1 st 2015 54% DV screened =high-danger –OF THOSE -64% reported a history of strangulation 12% other ( Department statistics Feb1- mid September)
 Type of case : 68% IPV/DV 30% SANE 2% Strangulation alone Signs and symptoms : 77% had Signs and symptoms 7% had NO signs or symptoms 16% had signs OR symptoms Jurisdiction : 48% Alexandria 30% Fairfax County – utilizing LAP since July 1 st 2015 54% DV screened =high-danger –OF THOSE -64% reported a history of strangulation 12% other ( Department statistics Feb1- mid September)")
112
Strangulation is a red flag… “The most dangerous domestic violence offenders strangle their victims. The most violent rapists strangle their victims. We used to think all abusers were equal. They are not. Our research has now made it clear that when a man puts his hands around a woman’s neck he has just raised his hand and said, ‘I am a killer.’ They are more likely to kill police officers, to kill children, and to later kill their partners. So when you hear, ‘He choked me,’ now we know you are at the edge of a homicide.” (Casey Gwinn, President and Co-founder of the National Family Justice Center Alliance) 112
 112.")
113
Common Issues in Serving Victimized Patients Building rapport and trust Privacy and safety What control and fear look like Trauma & the brain Know your role – not investigators Victim Autonomy

114
Cultural Competency Differences in countries, customs, beliefs with disclosures and view of violence Examples of how different cultures might respond to violence Gender preference Language access Fear of systems Immigration concerns (see T’s section) Reporting to police/other systems (lack of understanding of how system works, carrying over beliefs on bribery etc. from other countries) Trust in system (racism, bias, etc.) Faith leaders responses
 Trust in system (racism, bias, etc.) Faith leaders responses.")
115
Screening & Documentation Administering the Tool

116
Administering the tool: Setting the Scene Find ways to speak to the patient alone Avoid using anyone with the patient as an interpreter Ensure the safety of the patient, yourself and your facility Reassure confidentiality EXCEPT in the areas of mandated reporting Ask questions as they pertain to the patient’s health Avoid referring to the possible abuser/controller as a trafficker or perpetrator – use the term or name the patient uses. Keep in mind the victim may have been told not to trust health care providers or law enforcement

117
Administering the Tool: The Form Instructions for the Health Care Provider CUT AND PASTE FROM FORM

118
Administering the Tool: Starting the Conversation “Because abuse is so common, we ask all of our patients these questions.” Normalize questions to avoid patient feeling targeted. “The answers to these questions are confidential, unless… Child Abuse Elder Abuse Threats to Kill Yourself or Others, and Current injuries by weapons” “We want to provide resources and support, if needed.”

119
Administering the Tool: The Questions Read aloud questions 1 – 10 and mark the shaded box (Yes or No) for each question and document any quotes or comments in designated section. 1. Have 2. Are 3. Does 4. Does 5. Do 6. Do 7. Within 8. Has 9. Within 10. Since

120
Administering the Tool: The Questions

121
Administering the Question Follow-up Questions if needed: Has anyone ever caused you bodily harm or mental harm? Are you fearful of anyone? (this could be related to human trafficking) Are you free to manage your own life events? Do you feel someone is stalking you? AND 6) Can you make your own decisions of whether or not you will use birth control or condoms? (These questions pertain to reproductive coercion tactics that can be used to control someone’s ability to negotiate their birth control methods or decisions on whether to get pregnant or stay pregnant) Has anyone made you feel that you were forced into having sex or performing a sex act? IF SO, HOW LONG AGO? Has anyone strangled you or tried to strangle you? IF SO, HOW LONG AGO? Has anyone physically abused you? IF SO, HOW LONG AGO? Since you have been pregnant, has anyone physically abused you? IF SO, HOW LONG AGO? (Studies have shown that pregnancy can increase the likelihood of violence and its severity.)
 Are you free to manage your own life events. Do you feel someone is stalking you. AND 6) Can you make your own decisions of whether or not you will use birth control or condoms. (These questions pertain to reproductive coercion tactics that can be used to control someone’s ability to negotiate their birth control methods or decisions on whether to get pregnant or stay pregnant) Has anyone made you feel that you were forced into having sex or performing a sex act. IF SO, HOW LONG AGO. Has anyone strangled you or tried to strangle you. IF SO, HOW LONG AGO. Has anyone physically abused you. IF SO, HOW LONG AGO. Since you have been pregnant, has anyone physically abused you. IF SO, HOW LONG AGO. (Studies have shown that pregnancy can increase the likelihood of violence and its severity.).")
122
Sample question starters “you look pale, can you tell me about your diet?” “Feeling tired can be from lack of sleep. Can you tell me about your home and where you sleep? Do you have to ask permission to sleep, eat or go to the bathroom?” “The disease you have is not common in the US, how long have you been here? Can you tell me how and why you left your country? Do you have family or relatives here?” “I see that you have been treated for several STI’s, were you not able to have your partner treated or are you not able to negotiate condom use?” “Did you ever have sex to get things of value?” “Can you tell me about that tattoo/mark? Does it have special meaning to you?” How did you get that scar? Can you tell me about it?”

123
Supportive Statements Avoid appearing judgmental Check facial expressions and body language I’m glad you shared that with me. There is help available. Other possible statements: I believe you. The abuse is not your fault. How can I assist you in feeling safer? Help me understand how you feel. Avoid “Why” statements Avoid “Should” phrases

124
Documentation Documentation should include direct quotes whenever possible, especially any response in a bolded box. Carefully document any injuries using written descriptions of where on the body, type of injury and approximate size as well as the patient’s description of how the injury occurred.

125
Documentation If the patient consents and you have the option, photograph all injuries with and without a scale as well as some sort of patient identifier. Record areas of tenderness in conjunction with visible injuries as well as when no visible injury is apparent. Document symptoms Maximize your time with the patient since they may not have regular access to health care

126
Medical Red Flags & Treatment Needs

127
Medical Indicators of Trafficking In the 2014 study, the average sex trafficking victim had 10-13 buyers per day; up to 30-50 per day Chronic untreated health problems, including cardio, respiratory, gastrointestinal Long-term antibiotic use Significant dental problems Chronic back pain Bruises, scars and other indicators of physical abuse Substance abuse Note: medical issues persist after victim has left the life

128
Health Indicators: Sexual Health Reports a high number of sexual partners Multiple/frequent STIs or STI screening requests Multiple/frequent pregnancies or testing requests In 2014 study, 71% of survivors reported one or more pregnancies; 21% reported 5 or more while being trafficked 55% reported abortions, half of them forced. Complications of abortions--many are forced to resume sexual activities too soon. 55% had miscarriages HIV Pelvic pain Rectal trauma Urinary tract trauma/infections Infertility

129
Human Trafficking Indicators Delayed presentation for medical care or missed follow up appointments Forced abortion Discrepancy between injury and history Stated age older than visual appearance Patient not in control of his/her documents Another person speaking on behalf of pt. Few or no personal possessions Language barriers Lack of eye contact Flat affect/ submissive demeanor Loss of sense of time

130
Human Trafficking Indicators Claim that person is visiting the area or unable to clarify where he/she lives Marks, tattoos or insignias which may indicate an ownership Person accompanying potential victim insists on being present or giving all information to provider Multiple or frequent pregnancies Frequent abortions Frequent sexually transmitted infections Evidence of any kind of physical violence including torture

131
Offer additional medical services Inova Forensic Assessment and Consultation Teams (FACT) Department: Open 24/7, 365 days a year. Call us with questions or for clarification (703-776- 6666) or page us through hospital operator (703-776- 4001) All services are FREE and insurance is not charged so no EOBs sent to patient’s home Law enforcement does NOT need to be involved. An anonymous report can be generated and saved pending the patient’s desire to report.
 or page us through hospital operator ( ) All services are FREE and insurance is not charged so no EOBs sent to patient’s home Law enforcement does NOT need to be involved. An anonymous report can be generated and saved pending the patient’s desire to report..")
132
Offer additional medical services Inova Forensic Assessment and Consultation Teams (FACT) Dept #1 “Have you ever been emotionally or physically abused by your partner or someone else?” If Yes: “Has physical abuse happened within the last 5 days?” If Yes: “Would you like me to arrange a free, confidential exam? You do not have to have the police involved. I can put you in touch with a nurse who can more specifically explain the exam and your options.”

133
FACT Services: Domestic Violence What? A detailed report of the physical assault details; identification, assessment and photography of injuries; A danger assessment to measure risk of future lethality; connection to advocacy when possible and safety planning When? Within 5 days of the assault Where? Inova Fairfax (may be done at other safe locations if necessary) Why? Can be used for current or future litigation including protective orders How? Call 703-776-6666 during business hours or page the FACT nurse on call through the hospital operator (703-776- 4001)
 Why. Can be used for current or future litigation including protective orders How. Call during business hours or page the FACT nurse on call through the hospital operator ( ).")
134
Offer additional medical services Inova Forensic Assessment and Consultation Teams (FACT) Dept #7 “Within the last year, has anyone made you or pressured you into sexual activities?” If Yes: “Has that happening within the last 5 days?” If Yes: “Would you like me to arrange a free, confidential, exam? You do not have to have the police involved. I can put you in touch with a nurse who can more specifically explain the exam and your options.”

135
FACT Services: Sexual Violence What? A detailed report of the sexual assault details; identification, assessment and photography of injuries both genital and non-genital; Collection of a ‘rape kit’; Baseline STI testing; Provision of Plan B, STI prophylaxis and HIV prophylaxis when indicated; connection to advocacy when possible. When? Within 5 days of the assault Where? Inova Fairfax Why? Can be used for current or future litigation including protective orders How? Call 703-776-6666 during business hours or page the FACT nurse on call through the hospital operator (703-776- 4001)
.")
136
Offer additional medical services Inova Forensic Assessment and Consultation Teams (FACT) Dept #8 “Has anyone put their hands or anything else around your neck or over your mouth making it difficult to breathe?” If Yes: “Has that happening within the last 5 days?” If Yes: “This can be very dangerous. Are you having difficulty breathing or swallowing now?” If Yes – consider calling EMS If Yes: “Would you like me to arrange a free, confidential exam? You do not have to have the police involved. I can put you in touch with a nurse who can more specifically explain the exam and your options.”

137
FACT Services: Strangulation What? A detailed report of the physical assault details; identification, assessment and photography of injuries; Assessment for any current life threats: A danger assessment to measure risk of future lethality; connection to advocacy when possible and safety planning When? within 5 days of the assault Where? Inova Fairfax – may be done at other safe locations if necessary Why? Specialized medical expertise; Can be used for current or future litigation including protective orders How? Call 703-776-6666 during business hours or page the FACT nurse on call through hospital operator (703-776-4001)
.")
138
Pregnancy Risks Pre-term delivery - Study Low birth weight Each year, about 324,000 pregnant women in this country are battered by their intimate partners. That makes abuse is more common for pregnant women than gestational diabetes or preeclampsia -- conditions for which pregnant women are routinely screened. However, few physicians screen pregnant patients for abuse. Complications of pregnancy, including low weight gain, anemia, infections, and first and second trimester bleeding are significantly higher for abused women, as are maternal rates of depression, suicide attempts, tobacco, alcohol, and illicit drug use. DOUBLES RISK OF PREMATURE BIRTH

139
Resources & Safety Planning

140
What is Safety Planning Thinking ahead and acting in a way that can increase a victim’s safety and the safety of their loved ones. Safety Planning is MANDATORY -should be done whether a victim decides to stay in or leave an abusive relationship Develop a plan for each member of the household (mother, children, pets) Fluid, Continuous Process Victim-driven Assessing the offender- assess the victim’s fears Assessing danger in all environments ( work, home, school) Don’t forget, they know their situation better than anyone else.
 Fluid, Continuous Process Victim-driven Assessing the offender- assess the victim’s fears Assessing danger in all environments ( work, home, school) Don’t forget, they know their situation better than anyone else..")
141
What Does a Safety Plan Do? Promote safety Identify resources Develop tools and strategies Aim to reduce violence/threat of violence A safety plan does not guarantee safety… but it’s a start!

142
What Safety planning is not: Convincing the client to leave A rigid instruction manual Telling the client you think they should do A guarantee that the client will be safe

143
Safety Planning Conversation Questions: What strengths are you using to survive and stay safe? Who is the most helpful person in your life now? Who knows about the abuse? (family, boss, teachers) If you haven’t told anyone about the abuse, who is the family member or person that will listen with respect? Do you have a plan for if someone tries to hurt you or your children Do you and your children have a place to go if you are in danger? Have you asked the children where they can hide to feel safe? (Important for the victim to know where that place is.)
 If you haven’t told anyone about the abuse, who is the family member or person that will listen with respect. Do you have a plan for if someone tries to hurt you or your children Do you and your children have a place to go if you are in danger. Have you asked the children where they can hide to feel safe. (Important for the victim to know where that place is.).")
144
Safety Planning Conversation Questions: Have you ever had to make an important decision in the past? Who helped you look at your options and make a choice? Have you had to make a big change before? What or who helped you? Be careful in your questions that you aren’t making judgments or telling them to leave.

145
Crisis Intervention and Safety Planning Immediate Physical Safety Is the offender in the waiting room or building? Do you feel safe leaving here today and/or do you have a safe place to stay tonight? Who is in your life as a safe person you can trust to help you and do they know about the abuse/situation? Offer shelter options and resources Address medical necessities (FACT Dept)
.")
146
Artemis House: 703-435-4940 24-hour emergency shelter Imminent Risk Approximately 45 day stay Bethany House: 703-658-9500 Emergency Shelter Intakes conducted M-F 8:30-5:30 4-month stay No geographic limitations Domestic & Sexual Violence Emergency Shelters

147
What to Pack/Take Gather important documents such as: birth certificates, passports, social security numbers prescriptions copies of any protective orders marriage license insurance information children’s school records immunization (shot) records medical records information about bank accounts any other information you feel is necessary Clothing for yourself and children. Keep these things with a safe friend or hidden in a safe place you are able to access

148
Lethality Indicators/Signs of Escalation Has he/she ever used a weapon against you or threatened you with a weapon? Has he/she threatened to kill you or your children? Do you think he/she might try to kill you? Does he/she have a gun or can he/she get one easily? Has he/she ever tried to choke you? Is he/she violently or constantly jealous or does he/she control most of your daily activities?

149
Lethality Indicators/Signs of Escalation Have you left him/her or separated after living together or being married? Is he/she unemployed? Has he/she ever tried to kill himself/herself? Do you have a child that he/she knows is not his/hers? Does he/she follow or spy on you or leave threatening messages? Has he/she ever forced you to have sex when you did not wish to?

150
Safety Planning & Options Counseling Connection with DVAC (warm handoff) for more detailed options counseling and support: 703-246-4573 24-Hour Domestic & Sexual Violence Hotline: 703-360-7273 DVAC Victim Advocate will provide detailed options counseling: Crisis Intervention Detailed individualized safety planning Shelter Options Law Enforcement Reporting Options/Civil Protective Order Options Lethality Assessment Stalking & Technology
 for more detailed options counseling and support: 24-Hour Domestic & Sexual Violence Hotline: DVAC Victim Advocate will provide detailed options counseling: Crisis Intervention Detailed individualized safety planning Shelter Options Law Enforcement Reporting Options/Civil Protective Order Options Lethality Assessment Stalking & Technology")
151
Resource Handout I Hotlines Advocacy & Support Services Basic Needs Helpline (Coordinated Services Planning or CSP) Counseling & Support Groups DV Shelters (DV, SA and stalking) Homeless Emergency Shelters Transitional Housing (referral from shelter) Law Enforcement
 Counseling & Support Groups DV Shelters (DV, SA and stalking) Homeless Emergency Shelters Transitional Housing (referral from shelter) Law Enforcement")
152
Resource Handout II Legal Services Immigration Protective orders Family law/divorce/custody Magistrate’s Office Emergency Protective Orders Offender Services Protective Orders Underserved Populations

153
Sexual Assault Resources Handout

154
Human Trafficking Resource Brochure

155
Trafficking Safety Planning Some general features of safety planning are especially important in the case of trafficking victims: There is not a one-size-fits-all approach. This idea can actually increase danger. Safety planning must be constantly revisited as conditions change A victim may not leave the situation at this time, but need help planning how to anticipate and cope with possible risks Criminal justice and civil legal options may increase danger in the situation Victims have been applying safety measures to their situation, and must be free to choose their safety options Safety planning discussions are a time to help victims think about risks and resources they may not have considered

156
Trafficking Safety Planning Can be particularly challenging because of: Risks of harm by buyers as well as trafficker Gang involvement Threats to victim’s family Frequent movement Victim may have done illegal activities Victim’s family & friends may have put her/him into trafficking Victim may have small children Substance abuse Mental health issues

157
Potential considerations in safety planning with a trafficking victim: Assisting the trafficker may seem to increase a victim’s short-term safety, but make the victim vulnerable to charges and long-term control Because of traffickers’ networks, many victims must leave the area Traffickers may have access to victims’ phones and online accounts Victims may need assistance with pregnancies and children Victims with children may want to avoid actions with repercussions for child custody. Victims have lost custody to trafficker-fathers. Helpers or those looking for a victim may be in danger or place the victim in danger. Arranging a safe communication system can be very important. A trafficker may hold victim’s important documents or have legal rights over the victim Mental health resources may be very important for long-term recovery. Victims who have left the life may miss elements of it and return. This is especially true if victims are housed in groups. Return to family may not be the best goal. Family may have contributed to the victimization, or may not be able to deal with ways the victim has changed.

158
Secondary Trauma

159
What is Vicarious Trauma video https://www.youtube.com/watch?v=icYqLdlvyUk

160
Trauma Stewardship Video https://www.youtube.com/watch?v=tAKPgNZi_as

161
What is Secondary Trauma? Secondary traumatic stress is the emotional duress that results when an individual hears about the firsthand trauma experiences of another. Its symptoms mimic those of post-traumatic stress disorder (PTSD). Also known as vicarious trauma and provider fatigue. Change in the helper who may find themselves in a state of tension and may be pre-occupied with the stories/experiences of the client It’s not only normal, it’s expected – the difference is how we manage Commonly confused with compassion fatigue which is Secondary trauma + Burnout and sometimes primary trauma stress. Compassion fatigue is recognized by caregiver becoming the patient/client/victim. Primary Traumatic Stress + + Secondary Traumatic Stress Burnout Compassion Fatigue
. Also known as vicarious trauma and provider fatigue. Change in the helper who may find themselves in a state of tension and may be pre-occupied with the stories/experiences of the client It’s not only normal, it’s expected – the difference is how we manage Commonly confused with compassion fatigue which is Secondary trauma + Burnout and sometimes primary trauma stress. Compassion fatigue is recognized by caregiver becoming the patient/client/victim. Primary Traumatic Stress + + Secondary Traumatic Stress Burnout Compassion Fatigue.")
162
Why does it occur? Exposure to stories of trauma Desire to help/change survivor’s situation Feeling powerless when a service provider does not see positive changes in the survivor’s situations Overly identifying with survivors Thinking we have the power to change the survivor’s situations Your own experience of trauma possibly increasing risk of being triggered

163
Prevention and Management Self Awareness Self-care! Educate yourself about secondary trauma Eat healthy. Exercise. Spend time with family/friends. Do something you enjoy. Create a personal, safe work environment – a calming, relaxed, comfortable Purposefully be present Positive self talk Balance Work/Life Balance – spend time away from the office – 100% disconnected from work Recognize your limitations Manage workload – organization and scheduling – Go home on time Recognize your triggers Can I work with this population? Connection Support system - Make sure you have a healthy, well rounded group of people who you can trust to let you know when they see signs of vicarious trauma in you; and that you trust to help you work through it. Connect with colleagues/peers - participate in bonding opportunities and support others when you are able to Quality clinical supervision & continuing education

164
Initial Observable Changes: having difficulty talking about your feelings Increased caffeine and/or alcohol consumption difficulty falling asleep and/or staying asleep losing sleep over clients worried that you are not doing enough for their clients Lingering thoughts or dreaming about a clients’ trauma diminished joy toward things they once enjoyed or withdrawing from activities blaming others laughing at humor you would have once thought was offensive

165
Symptoms you can recognize Hypervigilance / anxiety Hopelessness / depression Inability to embrace complexity Inability to listen, avoidance of clients Anger, cynicism, irritability Sleeplessness / chronic exhaustion Fear Physical ailments Minimizing Guilt Fluctuations in weight – significant loss/gain Reliance on negative coping - Addiction Difficulty with interpersonal relationships Overworking Numbness Flashbacks / nightmares

166
What do I do it if I think I am experiencing Vicarious Trauma? Don’t be ashamed Tell someone you trust A colleague or peer A supervisor Someone from your support system Seek professional help Even counselors see other counselors

167
Intervention – What can be done? Strategies to evaluate secondary stress – be an advocate for yourself, assess to what degree this is impacting you - PROQOL Therapeutic Interventions – reach out to a counselor, therapist or mentor for help – EAP or OFWDSVS Mindfulness training – use mindfulness practices in daily work – breathing, grounding, visualizing other places, calming music Quality, honest supervision or mentoring Caseload / workload / schedule adjustment Informal gatherings following crisis events (to allow for voluntary, spontaneous discussions) Change in job assignment or work group
 Change in job assignment or work group.")
168
Increase your Self Awareness Ask yourself: How am I coping? What are my “hot buttons?” What are my warning signs? Am I practicing coping strategies? Am I self assessing my work stress? Am I being honest with myself? Who is a support I can be honest with about how I am doing? Buddy system for checking in on each other 168

169
Scenarios & Role Play

170
Resources & References

171
Domestic Violence and Health Resources & References http://www.fairfaxcounty.gov/domesticviolence/documents/dvppcc-annual- report-2014.pdf http://www.fairfaxcounty.gov/domesticviolence/documents/dvppcc-annual- report-2014.pdf https://aspe.hhs.gov/report/screening-domestic-violence-health-care-settings https://aspe.hhs.gov/report/screening-domestic-violence-health-care-settings http://www.futureswithoutviolence.org/userfiles/file/HealthCare/HealthCare. pdf http://www.futureswithoutviolence.org/userfiles/file/HealthCare/HealthCare. pdf http://www.cdc.gov/cdcgrandrounds/pdf/gr_partner_violence_jun19.pdf http://www.cdc.gov/cdcgrandrounds/pdf/gr_partner_violence_jun19.pdf www.cdc.gov/violenceprevention/nisvs www.cdc.gov/violenceprevention/nisvs https://www.acog.org/-/media/Committee-Opinions/Committee-on-Health- Care-for-Underserved-Women/co554.pdf?dmc=1&ts=20160401T0843418330 https://www.acog.org/-/media/Committee-Opinions/Committee-on-Health- Care-for-Underserved-Women/co554.pdf?dmc=1&ts=20160401T0843418330 http://www.futureswithoutviolence.org/userfiles/file/HealthCare/reproguidel ines_low_res_FINAL.pdf http://www.futureswithoutviolence.org/userfiles/file/HealthCare/reproguidel ines_low_res_FINAL.pdf

172
Strangulation Resources & References Bakers, RB & Somers, MS. Physical Injury from Intimate Partner Violence. Measurement, Strategies and Challenges. Journal of Obstetrics, Gynecology and Neonatal Nursing. 2008. 37 Christie et al. Can MRI of the Neck Compete with Clinical Findings in Assessing Danger to Life for Survivors of Manual Strangulation? A Statistical Analysis. Legal Medicine 2010. 12, 228-232 Faugno et al. Strangulation Forensic Examination. Best Practice for Health Care Providers. Advanced Emergency Nursing Journal. 2013. Vol 35, No 4, 314-327. Fineman. Riverside County District Attorneys Office 2013 Study. Glass et al. Non fatal Strangulation is an Important Risk Factor for Homicide of Women. Journal of Emergency Medicine. 2008. 35, 329-335. Laughon et al. Revision of the Abuse Assessment Screen to Address Non Lethal Strangulation. 2008 JOGNN 37, 502-507. McClane et al. A Review of 300 Attempted Strangulation Cases Part II Clinical Evaluation of the Surviving Victim. The Journal of Emergency Medicine. 2001. 21, no 3, 311-315. Pitchard et al. Non Fatal Strangulation as Part of Domestic Violence: A review of Research. Trauma, Violence and Abuse. 2015. 1-18.

173
Strangulation Resources & References Pollanen et al. Fracture of the Hyoid Bone in Strangulation: A Comparison of Fractured and Unfractured Hyoids from Victims of Strangulation. Journal of Forensic Science. 1996. 41:110-113. Rossen, Kabal, Anderson. Acute Arrest of Cerebral Circulation in Man. Archives of Neurology and Psychology. 1944. 50:510-528. Shield et al. Living Victims of Strangulation. A 10 Year Review of Cases in a Metropolitan Community. American Journal of Forensic Medicine and Pathology. 2010. 31:320-325. Smith et al. Frequency and Relationship of Reported Symptomatology in Victims of Intimate Partner Violence: The Effect of Multiple Strangulation Attacks. Journal of Emergency Medicine. 2001. 21:323- 329. Sorenson et al. A Systematic Review of the Epidemiology of Non fatal Strangulation: A Human Rights and Health Concern. American Journal of Public Health. 2014 Vol104 No.1 e54-e61. Stanley & Hanson. Manual Strangulation Injuries of the Larynx. Arch Otolarngol. 1982. Vol 109:344- 347. Strack et al. A Review of 300 Attempted Strangulation Cases Part I Criminal Legal Issues. The Journal of Emergency Medicine. 2001. 21, no 3, 303-309.

174
Human Trafficking Resources National Human Trafficking Resource Center (NHTRC) Hotline 1-888-373-7888 or www.traffickingresourcecenter.orgwww.traffickingresourcecenter.org Futures Without Violence http://www.futureswithoutviolence.org/workplace-safety- inequality/human-trafficking/ http://www.futureswithoutviolence.org/workplace-safety- inequality/human-trafficking/ JUST ASK Trafficking Prevention Foundation http://justaskprevention.com http://justaskprevention.com Fairfax County Office for Women & Domestic and Sexual Violence Services 24-hour hotline 703-360-7273 Fairfax County Public Schools teen sex trafficking curriculum and videos http://www.fcps.edu/it/fairfaxnetwork/trafficking/index.html http://www.fcps.edu/it/fairfaxnetwork/trafficking/index.html
 Hotline or Futures Without Violence inequality/human-trafficking/ inequality/human-trafficking/ JUST ASK Trafficking Prevention Foundation Fairfax County Office for Women & Domestic and Sexual Violence Services 24-hour hotline Fairfax County Public Schools teen sex trafficking curriculum and videos")
175
Secondary Stress Resources & References Secondary Traumatic Stress: A Fact Sheet for Child-Serving Professionals The National Child Traumatic Stress Network www.NCTSN.orgwww.NCTSN.org American Counseling Association Fact Sheet #9 (www.counseling.org)www.counseling.org DV Network Tier One Training - Susan Folwell, LCSW – Sept 2012

Similar presentations





 Click here to launch video Click here to download print activity.>")














: OCONUS 484-530-5908 www.myarmyonesource.com.>")

