Download presentation
Presentation is loading. Please wait.

1
Spontaneous bacterial peritonitis (SBP)
")
2
SBP-Definition Peritoneal infections are classified as primary (ie, spontaneous), secondary (ie, related to a pathologic process in a visceral organ), or tertiary (ie, persistent or recurrent infection after adequate initial therapy). Spontaneous bacterial peritonitis is characterized by the spontaneous infection of ascitic fluid in the absence of an intraabdominal source of infection (e.g. intestinal perforation, abscess). (Genuit T., e-medicin august, 2002). (Garcia-Tsao, Can J Gastroenterol. 2004)
, secondary (ie, related to a pathologic process in a visceral organ), or tertiary (ie, persistent or recurrent infection after adequate initial therapy). Spontaneous bacterial peritonitis is characterized by the spontaneous infection of ascitic fluid in the absence of an intraabdominal source of infection (e.g. intestinal perforation, abscess). (Genuit T., e-medicin august, 2002). (Garcia-Tsao, Can J Gastroenterol. 2004)")
3
SBP-Definition Other spontaneous infections in cirrhotic patients are spontaneous bacterial empyema and spontaneous bacteremia (positive blood cultures in the absence of a source of infection). All have the same pathogenesis and should be managed in the same fashion. The most common is SBP with an incidence of approximately 10-30%. (Garcia-Tsao, Can J Gastroenterol. 2004)
. All have the same pathogenesis and should be managed in the same fashion. The most common is SBP with an incidence of approximately 10-30%. (Garcia-Tsao, Can J Gastroenterol. 2004)")
4
SBP-Aetiology Infection is blood-born and in 90% monmicrobial.
The majority (70%) of the cases are caused by organisms of the normal flora of the intestine, mainly aerobic gram-negative organisms with E. coli accounting for half the cases. The next most frequent microorganisms are gram-positive cocci, mainly Streptococcus sp (20%) with enterococcus accounting for 5% of the cases. Infection with more than one organism is likely to be associated with abdominal paracentesis or intra-abdominal source of infection. (Garcia-Tsao, Can J Gastroenterol. 2004 (Sheila Sherlock2002).
 of the cases are caused by organisms of the normal flora of the intestine, mainly aerobic gram-negative organisms with E. coli accounting for half the cases. The next most frequent microorganisms are gram-positive cocci, mainly Streptococcus sp (20%) with enterococcus accounting for 5% of the cases. Infection with more than one organism is likely to be associated with abdominal paracentesis or intra-abdominal source of infection. (Garcia-Tsao, Can J Gastroenterol (Sheila Sherlock2002).")
5
SBP-Aetiology A variety of abnormalities have been identified contributing to infection. Gastrointestinal bleeding, Increased colonization of the small bowel with prominent bacterial translocation, decreased opsonin function in both blood and ascites, impaired complement, leukocyte dysfunction, decreased antibodies and increased immunosuppressive cytokines, endotoxin, or tumor necrosis factor have been found in advanced liver failure. Invasive procedures, such as endoscopy or TIPS, the use of indwelling venous and urinary catheters are often immediate antecedents of infection (Iber, American J Gastro 1999)
")
6
SBP-Pathogenesis As cirrhosis develops in animals, gram-negative bacteria increase in numbers in the gut. The gut of patients with advanced cirrhosis is more permeable to bacteria than the normal gut and more permeable than the gut in less advanced cirrhosis. Once bacteria reach a critical concentration in the gut lumen, they "spill over", and escape the gut, "translocating" to mesenteric lymph nodes. Then they can enter lymph, blood, and eventually ascitic fluid. (Runyon Gut 2004) (Cirera, J Hepatol 2001) ( Runyon J Hepatol 1994)
 (Cirera, J Hepatol 2001) ( Runyon J Hepatol 1994)")
7
SBP-Pathogenesis Peritoneal macrophages are the first line of defence against bacterial colonisation of ascitic fluid. SBP occurs when macrophages fail to kill the bacteria and the second line of defence is called in, the neutrophils. Opsonins assist motile and fixed killers of bacteria, the neutrophils and Kupffer cells, respectively. If the ability of the ascitic fluid to assist macrophages and neutrophils in killing the errant bacteria is deficient, uncontrolled growth occurs. The opsonic activity of the ascitic fluid is proportional to protein concentration and SBP is more likely if ascitic fluid protein is less than 1 g/ dl.

8
SBP-Pathogenesis Thus SBP is the result of failure of the gut to contain bacteria and failure of the immune system to kill the virulent bacteria once they have escaped the gut making patients with cirrhosis vulnerable to infection by their own gut flora. The recent molecular evidence of bacterial translocation shows patients with cirrhosis having bacterial DNA in their serum and ascitic fluid, and that DNA is always present simultaneously in both body fluids. (Such Hepatology 2002 Francés, Gut 2004)
")
9
SBP-Pathogenesis Innate defenders against bacterial invasion include macrophages, dendritic cells, and natural killer cells. These cells synthesise proinflammatory cytokines and effector molecules, which assist in killing bacteria. Unfortunately, patients with advanced cirrhosis have been reported to have defects and dysfunction in many of these systems of protection. To make matters worse, some of the effector molecules and cytokines that help kill the bacteria have undesired side effects. NO and TNF are important mediators of vasodilation and renal failure that too often accompany SBP. Fiuza J Infect Dis 2000 &Such, Eur J Gastroenterol Hepatol, 2004

10
SBP-Diagnosis Early diagnosis and the initiation of prompt effective therapy have played key roles in decreasing the mortality associated with SBP. SBP should be suspected if a patient with known cirrhosis deteriorates. Ascitic fluid protein less than 1 g/ dl and height serum Bilirubin independently predict the first SBP. Patients with variceal bleeding or previous SBP are at particular risk. Patients may develop abdominal pain, tenderness, fever, and systemic leucocytosis, however these features may be absent and the diagnosis is made on the index of suspicion with examination of the ascitic fluid.

11
SBP-Diagnosis A diagnostic paracentesis should be performed
In any cirrhotic patient that develops compatible symptoms and/or signs of peritonitis In any cirrhotic patient who develops sudden unexplained deterioration in renal function or hepatic encephalopathy. In any patient with cirrhosis and ascites admitted to the hospital, independent of the presence or absence of compatible symptoms and/or signs of a peritoneal infection. Rimola et al., Hepatology 1985 Garcia-Tsao, Can J Gastroenterol. 2004

12
SBP-Diagnosis The diagnosis is established with the finding of an ascites polymorphonuclear count (PMN) >250/mm. Bacterial count in the ascites is low. Direct inoculation of routine blood culture bottles at the bedside with 10 cc of ascitic fluid has been reported to significantly increase the sensitivity of microbiologic studies Culture-negative neutrocytic ascites exists when the ascitic fluid cultures are negative yet the PMN count is >500 cells/mm Bacterascites exists when a positive culture coexists with a nonelevated ascites PMN count. (Caly J, Hepatol 1993&Garcia-Tsao, Can J Gastroenterol. 2004)
")
13
SBP-Diagnosis . Blood cultures are positive in 33%.
An ascites lactate level of >25 mg/dL was found to be 100% sensitive and specific in predicting active SBP in a retrospective analysis. The combination of an ascites fluid pH of <7.35 and PMN count of >500 cells/mm3 was 100% sensitive and 96% specific. A diagnostic thoracentesis should be performed in cirrhotic patients with new onset pleural effusion and in patients in whom SBP/infection is suspected but in whom there is no ascites or in whom the ascites PMN count is <250/mm3

14
SBP-Complication The most severe complication of spontaneous bacterial peritonitis is the hepatorenal syndrome, which occurs in up to 30 percent of patients and carries a high mortality rate. After resolution, SBP may recur, with an estimated 70 percent probability of recurrence at one year. (Sort et al. N Engl J Med 1999 &GrangeJ et ai., Hepatol 1998)
")
15
SBP-Treatment A minimal duration of five days of parenteral, third-generation cephalosporin such as cefotaxime 2 gm every 12 h is usually effective. Intravenous Amoxycillin-clavulanic acid is as effective as cefotaxime. Intravenous ciprofloxacin followed by oral treatment is also effective. These regimens are for initial empiric therapy and antibiotic choice should be reviewed once results of ascitic culture are known. (Sheila Sherlock2002).
.")
16
SBP-Treatment A trial that investigated oral ofloxacin found it as effective as intravenous cefotaxime in the treatment of SBP. This trial identified a small subgroup of patients with SBP that had an excellent prognosis (100% SBP resolution and 100% survival) and was characterized by having a community-acquired SBP, no encephalopathy and a BUN <25mg/dL. Navasa et al., Gastroenterology 1996
 and was characterized by having a community-acquired SBP, no encephalopathy and a BUN <25mg/dL. Navasa et al., Gastroenterology")
17
SBP-Treatment Intravenous albumin (1.5 g per kilogram of body weight at diagnosis and 1 g per kilogram 48 hours later) significantly lower rates of renal dysfunction (10% vs. 33%), hospital mortality (10% vs. 29%) and 3-month mortality (22% vs. 41%) compared to patients that did not receive albumin. The inpatient mortality rate of 10% is the lowest described so far for SBP. (Sort et al. N Engl J Med 1999 Garcia-Tsao, Can J Gastroenterol. 2004)
 significantly lower rates of renal dysfunction (10% vs. 33%), hospital mortality (10% vs. 29%) and 3-month mortality (22% vs. 41%) compared to patients that did not receive albumin. The inpatient mortality rate of 10% is the lowest described so far for SBP. (Sort et al. N Engl J Med 1999 Garcia-Tsao, Can J Gastroenterol. 2004)")
18
SBP-Treatment The group of patients that benefit from the addition of albumin was characterized by having a serum bilirubin >4mg/dL and evidence of renal impairment at baseline (BUN >30 mg/dL and/or creatinine >1.0 mg/dL)13. This regimen is empirical, and no information exists on the efficacy of lower albumin doses or other plasma expanders. (Ginès, N Engl J Med 2004 & Garcia-Tsao, Gastroenterology Garcia-Tsao, Can J Gastroenterol. 2004)
13. This regimen is empirical, and no information exists on the efficacy of lower albumin doses or other plasma expanders. (Ginès, N Engl J Med 2004 & Garcia-Tsao, Gastroenterology Garcia-Tsao, Can J Gastroenterol. 2004)")
19
SBP-Treatment Diuretic therapy increases the total protein and ascitic opsonic activity. Patients should be treated in the hospital until there is clear evidence of improvement, specifically resolution of symptoms/signs and a >25% decrease in ascites PMN count in a follow-up (48-hour) paracentesis. Spontaneous bacterial peritonitis is an indication to consider hepatic transplantation, particularly if recurrent. Garcia-Tsao, Can J Gastroenterol. 2004
 paracentesis. Spontaneous bacterial peritonitis is an indication to consider hepatic transplantation, particularly if recurrent. Garcia-Tsao, Can J Gastroenterol")
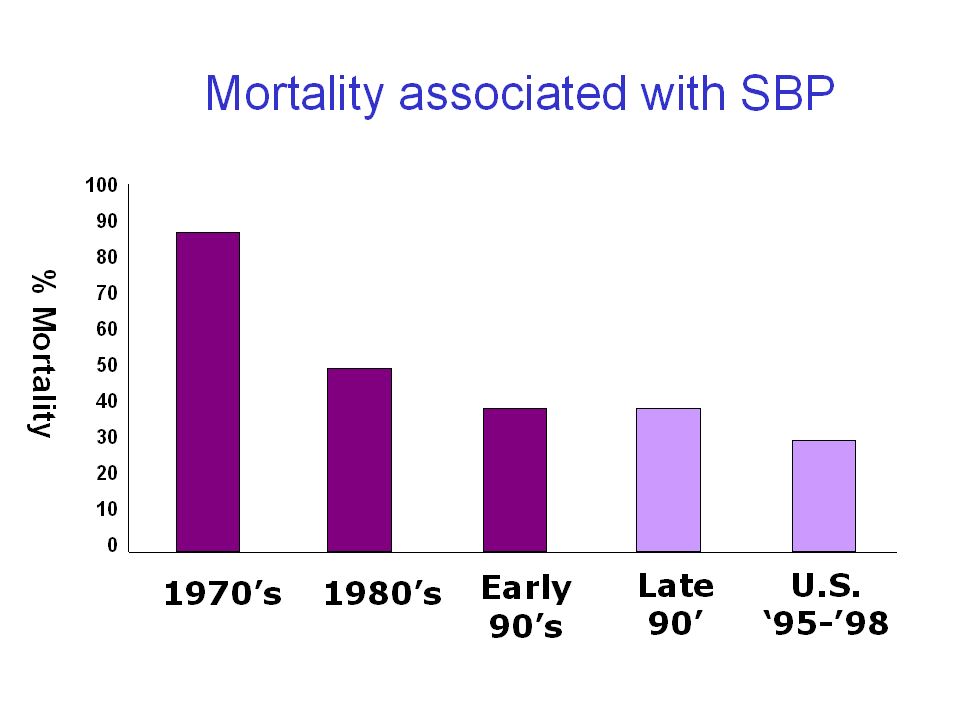
20
SBP-Prognosis In initial series published in the 1970’s, when the entity was first described, the mortality exceeded 80%; studies in the early 1980’s revealed an SBP mortality of 50% and in the early 1990’s, mortality had decreased to around 40%. In more recent prospective studies with well-defined criteria for the diagnosis of SBP, the mortality rate was 20-30% Ricart et al J Hepatol 2000 Thuluvath Am J Gastroenterol 2001& Garcia-Tsao, Can J Gastroenterol. 2004 .

22
SBP-Prophylaxis SHORT-TERM PRIMARY PROPHYLAXIS (PREVENTION OF BACTERIAL INFECTIONS IN PATIENTS WITH GI HEMORRHAGE) LONG-TERM SECONDARY PROPHYLAXIS (PREVENTION OF SBP RECURRENCE). PROPHYLAXIS IN PATIENTS WITHOUT PRIOR SBP OR GI HEMORRHAGE? Garcia-Tsao, Can J Gastroenterol. 2004
. PROPHYLAXIS IN PATIENTS WITHOUT PRIOR SBP OR GI HEMORRHAGE Garcia-Tsao, Can J Gastroenterol")
23
SBP-Prophylaxis 1-SHORT-TERM PRIMARY PROPHYLAXIS
A meta-analysis of five randomized controlled trials shows that short-term antibiotic prophylaxis not only resulted in a significant decrease in the incidence of infections (45% in controls vs. 14% in antibiotic-treated patients), including SBP (27% vs 8%) but was also associated with a significant improvement in survival (from 24% in controls to 15% in treated patients). The preferred antibiotic is norfloxacin 400 mg twice a day orally for 7-day. (Bernard; Hepatology 1999; Garcia-Tsao, Can J Gastroenterol )
, including SBP (27% vs 8%) but was also associated with a significant improvement in survival (from 24% in controls to 15% in treated patients). The preferred antibiotic is norfloxacin 400 mg twice a day orally for 7-day. (Bernard; Hepatology 1999; Garcia-Tsao, Can J Gastroenterol )")
24
SBP-Prophylaxis 2-LONG-TERM SECONDARY PROPHYLAXIS
In patients with previous episodes of SBP, long-term prophylaxis with oral norfloxacin 400 mg daily is initiated as soon as the course of antibiotics for the acute episode of SBP is completed and should be continued until disappearance of ascites, death or transplantation. There is a concern that long-term Prophylaxis will lead to emergence of resistant bacteria (Rimola et al., J Hepatol 2000 & Garcia- Tsao Gastroenterology 2001).
.")
25
SBP-Prophylaxis 3- PROPHYLAXIS IN PATIENTS WITHOUT PRIOR SBP OR GI HEMORRHAGE. Currently, there is insufficient data to support the use of long-term antibiotic prophylaxis in cirrhotic patients with ascites who are not bleeding and who have not had a previous episode of SBP. Patients with an ascites protein > 1.0 g/dL will not develop SBP in a follow-up period of 2 years and therefore do not require prophylaxis (Garcia- Tsao Gastroenterology 2001).
.")
26
SBP-Prophylaxis In patients with low ascites protein levels who have never had SBP or who are not hospitalized with GI hemorrhage, efforts should be made to identify other risk factors for SBP. In a recent study, a bilirubin >3.2 mg/dL and a platelet count <98,000 have been able to identify up to 55% of patients that will develop SBP. Results of prophylactic, placebo-controlled trials in this group of patients will confirm that these are in fact high risk patients and, more importantly, evaluate the efficacy of primary prophylaxis. (Grange; J Hepatol 1998 &Garcia-Tsao, Can J Gastroenterol. 2004)
")
27
SBP-Prophylaxis Vaccination of all cirrhotic patients with polyvalent pneumococcal vaccine is established as effective in reducing colonization in cirrhosis. In cirrhotic patients, same-day treatment centers should be used instead of hospitalization; if hospitalization is necessary, intensive care units and hospital days should be used in a miserly manner. (Zetterman, Semin Liver Dis 1995 Chang et al., Infect Control Hosp Epidemiol 1998)|
|")
28
In hospitals, skin cleanliness and universal precautions to diminish patient-to-patient colonization must be observed. Urinary and intravenous catheters should be avoided whenever possible, and proven techniques should be used to minimize infection when these are necessary. (Iber, American J Gastro 1999))
)")
29
Thank You

31
Bacterial infections in
liver cirrhosis

32
Bacterial infections is second in frequency to bleeding varices as a fatal complication of cirrhosis. Prospective series describe an incidence of infections in hospitalized patients of 15%, 20% and 47%. A recently published series reported the presence of bacterial infections (either at the time of admission or during hospitalization) in 32% of cirrhotic patients. These figures are in contrast with the hospital-cquired infection rate in the general hospital population reported to be between 5% and 7%.
 in 32% of cirrhotic patients. These figures are in contrast with the hospital-cquired infection rate in the general hospital population reported to be between 5% and 7%..")
33
Studies in the 1980’s showed that the most common infections were urinary tract infections, spontaneous bacterial peritonitis (SBP) and pneumonia, and also showed that approximately 70-80% of infecting organisms were gram-negative bacilli (GNB). In a recent large series SBP was the most common infection, followed by urinary tract infection, pneumonia and bacteremia. The causative organisms isolated in SBP and urinary tract infections were mainly GNB. In contrast, the most frequent bacteria isolated in pneumonia and bacteremias associated with invasive procedures were gram-positive cocci.

Similar presentations






























 is characterised by massive colonic dilation with symptoms and signs of colonic obstruction.>")