Download presentation
Presentation is loading. Please wait.

1
Metabolism module Adrenal disorders Session 12 Lecture 1 Kufa Medical College

2
Objectives: The aim of this lecture is that, by its end, you should understand 1.The functions of the steroid hormone, 2.How its level is assessed 3.How adrenal cortex function is altered in common diseases.

3
Adrenal disorders Most commonly affect cortisol secretion –Hyper secretion – Cushing’s syndrome –Hypo secretion – Addison’s disease Can get hypersecretion of aldosterone –Conn’s syndrome

4
Cortisol functions Metabolic function: stress hormone, cortisol antagonizes the activity of insulin by: Inhibiting the cellular glucose uptake increases protein breakdown & lipolysis, (i.e. increases the activity of gluconeogenesis. [so called diabetogenic agent].

5
Electrolyte control: Cortisol involved in retention of water and electrolytes from renal tubules to ECF (blood and interstitial compartment). This explains why deficiency of this enzyme results in hypotension, while excess amounts results in hypertension.

6
Immunosuppressant & anti-inflammatory Agent: because it decreases the No. of leucocytes and also their migration and inhibits phospholipase A2, which is important for production of inflammatory molecules (prostaglandins and leukotrienes). For this reason, cortisol is used as a drug in the treatment of inflammatory conditions such as allergy and rheumatic diseases and to suppress immunity in tissue transplantation and cancer patients.
. For this reason, cortisol is used as a drug in the treatment of inflammatory conditions such as allergy and rheumatic diseases and to suppress immunity in tissue transplantation and cancer patients..")
7
Circulating cortisol level In blood, 95 per cent of cortisol is bound CBP, The other 5 per cent of hormone is free. The hormone is inactivated by liver cells and excreted in urine as free cortisol.

8
Q: Why serum cortisol levels increased more than normal? Excess ACTH (common): is part of a syndrome due to pituitary adenoma (Cushing's disease). It is either caused by non-pituitary carcinoma or by ACTH therapy. Both ACTH & cortisol high (feedback is active??) Excess Cortisol: due to tumours in adrenal cortex or cortisol therapy. High cortisol & low ACTH (what occur if the drug is dexamethazone? Why?)
: is part of a syndrome due to pituitary adenoma (Cushing s disease). It is either caused by non-pituitary carcinoma or by ACTH therapy. Both ACTH & cortisol high (feedback is active ) Excess Cortisol: due to tumours in adrenal cortex or cortisol therapy. High cortisol & low ACTH (what occur if the drug is dexamethazone. Why ).")
9
Q: What occur if serum cortisol levels increased more than normal? causes Cushing's syndrome

10
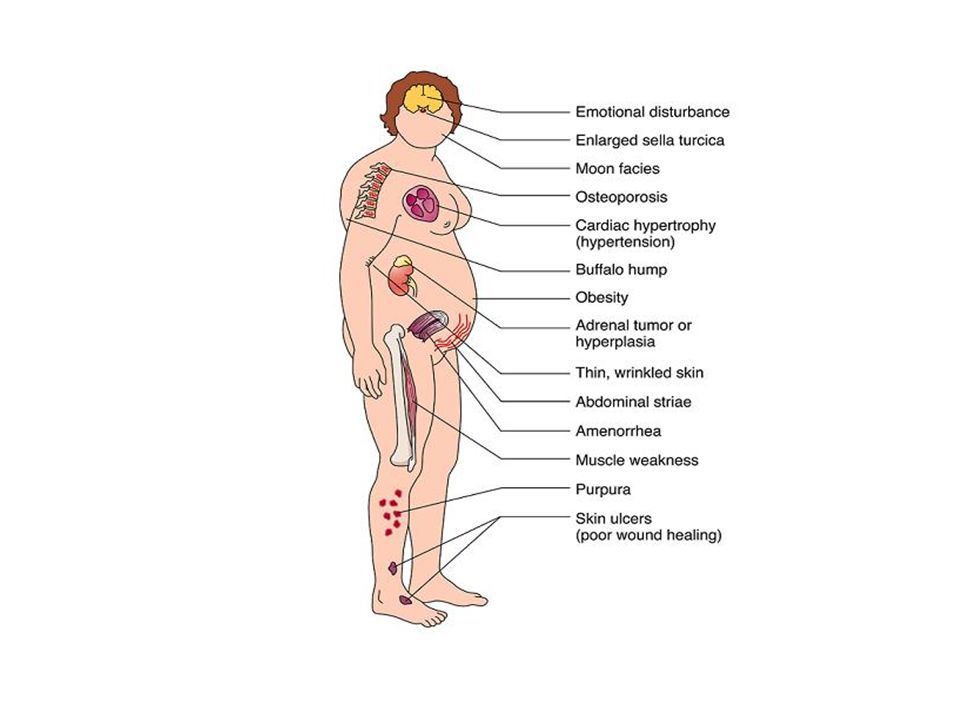
What are the symptoms and signs of Cushing’s syndrome? Clinical Features

12
Symptoms of Cushing’s Central weight gain Change of facial appearance Insomnia Depression Thin skin Hair growth Acne Poor libido Menstrual defects

13
Signs of Cushings ‘moon face’ Plethora (congested face) Thin skin Bruising Hypertension Pathological fractures Striae
 Thin skin Bruising Hypertension Pathological fractures Striae")
14
Signs of Cushing’s Central obesity Striae

15
Signs of Cushing’s Moon face in a child

16
Q: Explain WHY Excess cortisol causes the following: –Truncal obesity and moon face –Thin skin –Striae -Muscle weakness –Hyperglycaemia –Acne -Recurrent infections- Used in Rx of inflammatory conditions and allergy –Hirsutism -Menstrual disorders –Hypertension –Osteoporosis

17
Q: If Cushing's syndrome occurs, what are the metabolic consequences of high cortisol levels? As it is insulin antagonist, cortisol results in hyperglycemia Glycosuria We call it DM or glucose intolerance

18
Protein breakdown causes negative nitrogen balance (with muscle weakness), breakdown in collagen results in osteoporosis. Also, protein breakdown results in muscle wasting and thin skin with bruising. (striae atrophicae).
..")
19
Higher cortisol acts like aldosterone, enhances Na+ reabsorption (hypernatraemia) in exchange to H+ & K+ ions in the renal tubules. This means increased loss of K+ in urine (hypokalaemia) and H+ (alkalosis = pH > 7.45). If the cause of Cushing's syndrome is excess ACTH, this hormone will stimulate both androgen & cortisol production. androgen causes hirsutism, virilism and menstrual disturbances in female patients.
 and H+ (alkalosis = pH > 7.45). If the cause of Cushing s syndrome is excess ACTH, this hormone will stimulate both androgen & cortisol production. androgen causes hirsutism, virilism and menstrual disturbances in female patients..")
20
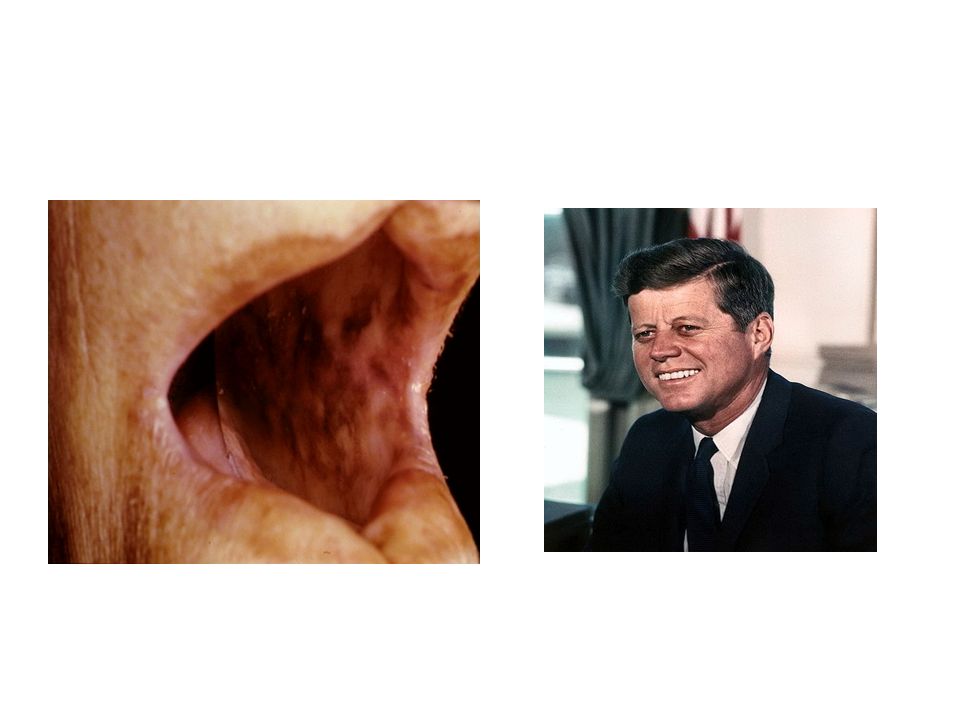
Effects of excess ACTH In addition to over-stimulation of cortisol ACTH also mimics Melanocyte Stimulating Hormone (MSH) Leads to excess skin pigmentation BUT in which TYPE? Only if ACTH is the cause.

21
Differential Diagnosis Alcoholism obesity Anorexia nervosa (high urine free cortisol) Familial cortisol resistance Familial partial lipodystrophy type I
 Familial cortisol resistance Familial partial lipodystrophy type I")
22
Q: what Laboratory tests we should do to investigate a suspected case of Cushing's syndrome? Serum cortisol: (both morning and evening levels) to see if there is any defect in circadian rhythm which lost in this case. Urine free cortisol: in 24hr urine samples is diagnostic when it is at very high levels.
 to see if there is any defect in circadian rhythm which lost in this case. Urine free cortisol: in 24hr urine samples is diagnostic when it is at very high levels..")
23
Tests for HPA axis: by checking both serum cortisol & ACTH, to know the cause of disease If both are increased, this secondary. If only cortisol is high while ACTH is very low, this primary disease. If both are low, it indicates drug therapy. (explain how?)
.")
24
Screening Test Overnight dexamethasone suppression test (1 mg at 11 pm, cortisol measured at 8 am) – normal <2 micrograms/dL Or 24 hour urine free cortisol (>140 nmol/day)
 – normal <2 micrograms/dL Or 24 hour urine free cortisol (>140 nmol/day)")
25
There are two types of dexamethasone suppression tests: the low-dose test the high-dose test. Low-dose overnight method – we give 1 mg of dexamethasone at 11 p.m., and blood drawn at 8 a.m. for a cortisol measurement. High-dose overnight method – Basal cortisol measured on the morning of the test. Then we will give 8 mg of dexamethasone at 11 p.m. blood is drawn at 8 a.m. for a cortisol measurement.

26
Treatment of Cushing’s Very poor prognosis if untreated Most commonly surgical removal of pituitary or adrenal tumour But need to reduce effects of excess cortisol first by drugs which reduce synthesis –Metyrapone – 11 -hydroxylase blocker

27
Iatrogenic disease Steroids commonly used long term to treat inflammatory conditions Can cause serious complications –Diabetes –Exacerbation of infections –Poor wound healing –Osteoporosis –Adrenal cortical atrophy (suppressed ACTH secretion)
")
28
Stopping steroids Effects of sudden steroid withdrawal can be very severe –Atrophied adrenal cortex cannot produce enough natural steroid –Always withdraw steroids progressively (Tapering)
")
29
Addison’s disease Destruction of adrenal cortex –Most commonly auto-immune –Infection mostly due to Tuberculosis (TB) Affects secretion of ALL hormones cortisol, mineralocorticoids and androgens Effects initially vague, but can proceed to Addisonian crisis –Often precipitated by stress or illness (WHY?)
 Affects secretion of ALL hormones cortisol, mineralocorticoids and androgens Effects initially vague, but can proceed to Addisonian crisis –Often precipitated by stress or illness (WHY )")
30
Symptoms and signs of Addison’s disease Symptoms –Tiredness, weakness, weight loss –Myalgia, GI disturbance, joint pain –Fainting Signs –Hyperpigmentation –Postural hypotension –Weight loss –Dehydration

31
Basis of symptoms & signs of Addison’s Lack of aldosterone –Electrolyte disturbances (Na +, K +, water) –Reduced circulating volume –Low blood pressure (Hypotension) Lack of cortisol –Reduced blood glucose – weakness –Reduced inhibition of ACTH (loss of –ve feedback) –Enhanced ACTH mimics MSH – pigmentation –(cortisol but not aldosterone regulate HPA axis)
 –Reduced circulating volume –Low blood pressure (Hypotension) Lack of cortisol –Reduced blood glucose – weakness –Reduced inhibition of ACTH (loss of –ve feedback) –Enhanced ACTH mimics MSH – pigmentation –(cortisol but not aldosterone regulate HPA axis)")
32
Aldosterone disorders: 1) Aldosterone deficiency is of two types: Primary adrenal hypo-function (Addison's disease): occurs due to damage of the adrenal cortex by disease. all hormones including aldosterone, cortisol and androgens are deficient loss of exchange of Na ⁺ to K ⁺ and H ⁺ in renal tubules. leads to hypotension, hypokalaemia and acidosis (pH < 7.35), while low cortisol level results in loss of negative feedback inhibition of HPA axis, leading to increased serum ACTH, thus increased melanin production ( Hyperpigmentation)
, while low cortisol level results in loss of negative feedback inhibition of HPA axis, leading to increased serum ACTH, thus increased melanin production ( Hyperpigmentation).")
34
Secondary adrenal hypo-function: Damage of hypothalamus or pituitary gland with normal adrenal gland In this disease only serum cortisol and androgen are low, while aldosterone is in normal range (why?). (cortisol but not aldosterone nor regulate HPA axis)
.")
35
Treating Addison’s An Addisonian crisis is a medical emergency and can lead to vascular collapse (shock): –Need to treat with high doses of hydrocortisone –Rehydrate with saline –Correct hypoglycaemia with glucose
: –Need to treat with high doses of hydrocortisone –Rehydrate with saline –Correct hypoglycaemia with glucose")
36
Treating Addison’s In the longer term –Replace cortisol –Replace mineralocorticoid –Can replace androgens

37
2) Aldosterone Excess; is also of two types — Primary aldosteronism (Conn's disease): in which adrenal cortex tumours secrete large amounts of aldosterone, which enhance exchange mechanism with subsequent hypernatraemia, hypokalaemia and alkalosis. Secondary aldosteronism: or oedema long-standing disease e.g. low renal blood flow due to cardiac failure or liver cirrhosis that stimulates renin- angiotensin system, production of large quantities of aldosterone. features are the same as primary type; hypernatraemia, hypokalaemia and alkalosis.

38
Congenital Adrenal Hyperplasia A range of genetic disorders –Partial loss of activity of enzymes in steroid biosynthesis –Changes balance of steroid secretion Changes in substrates Effects on feedback control systems

39
Synthesis of adrenal steroids Cholesterol ester Cholesterol (C27) Progesterone (C21) Mineralocorticoids (C21)Glucocorticoids (C21) Androgens (C19)
 Progesterone (C21) Mineralocorticoids (C21)Glucocorticoids (C21) Androgens (C19)")
40
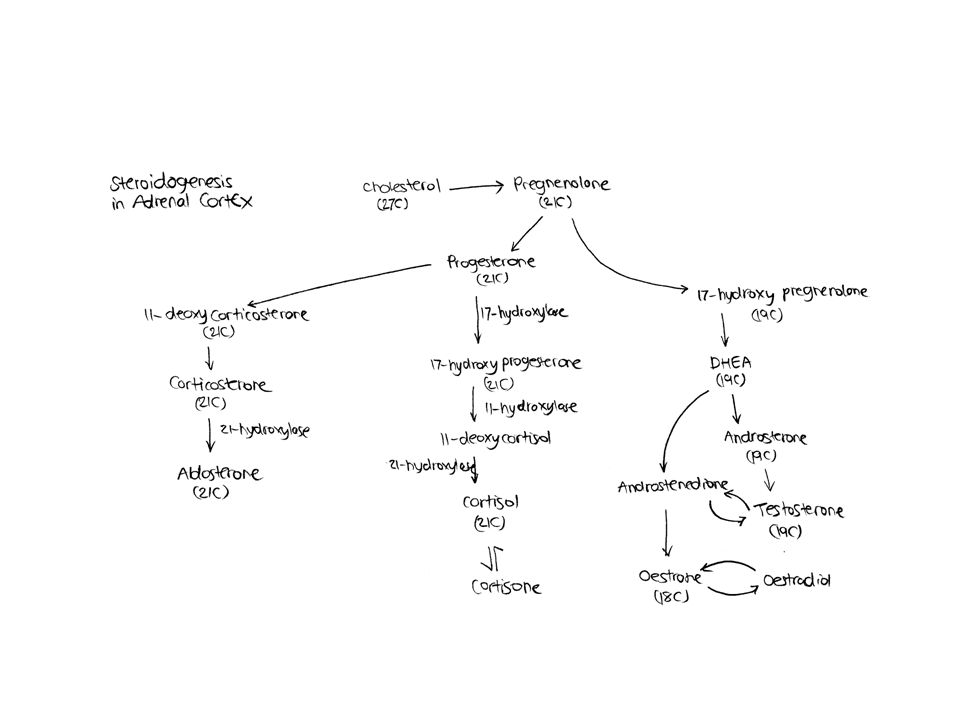
Congenital Adrenal Hyperplasia (CAH) Normally steroidogenesis involves several enzymatic reactions such as Hydroxylases, Dehydrogenases, and Isomerases. Abnormalities in hydroxylation reactions are the most common e.g. cortisol is synthesised by 3 subsequent hydroxylases, which are 17-, 21- and 11- hydroxylases. Congenital deficiency of 17- or 11-hydroxylase is very rare and involves only cortisol production.

41
21-hydroxylase is most common and affects both cortisol and aldosterone. low cortisol, resulting in loss of negative feedback inhibition, with production of large quantities of ACTH. ACTH increases the size and number of adrenal cortex cells (hyperplasia), with increased precursors of cortisol and aldosterone before enzymatic block. These precursors may be metabolized by an alternative pathway, especially androgen (its level rises), resulting in hermaphrodites in childhood with ambiguous genitalia of either sex. See figure
, with increased precursors of cortisol and aldosterone before enzymatic block. These precursors may be metabolized by an alternative pathway, especially androgen (its level rises), resulting in hermaphrodites in childhood with ambiguous genitalia of either sex. See figure.")
43
Effects of congenital adrenal hyperplasia Increased testosterone –Prenatal – masculinisation of external genitalia in female –Post natal Early puberty in males Virilisation in females

44
Treatment of CAH Replace cortisol (or equivalent) Replace mineralocorticoids
 Replace mineralocorticoids")
Similar presentations


, FRCP Consultant Endocrinologist>")


 By: Anna Heideman & Angela Mullins.>")










… gluconeogenesis in the liver.. Hyperglycemia… increased insulin output…>")



